Adaptation of ISTH Guidelines on Vaccine Induced Thrombocytopenic Thrombosis to Clinical Practice and Analysis of Patient Cases
The International Society on Thrombosis and Haemostasis (ISTH) published guidelines for the diagnosis and treatment on Vaccine-Induced Thrombotic Thrombocytopenia (VITT) in April of 2021. Guidelines were inclusive of those persons at risk for VITT, screening, initial evaluation, and treatment. A study was conducted to evaluate case reports of patients with VITT in regard to diagnostic testing and treatment options as recommended by the ISTH. Ten case reports were identified employing the PubMed database where VITT was diagnosed in patients who received the Astra Zeneca vaccine. The average fibrinogen level was 166.9 mg/dL, the average platelet count was 47.2 x 109/L, and the average D-Dimer level was 39.3 mg/L. All cases of VITT exhibited a positive anti-PF4 assay. Anticoagulants administered to patients varied across cases however all patients received IVIG to increase platelet counts in patients. A one sample t test was performed to ascertain if statistical significance was present comparing average fibrinogen, platelet count, and D-Dimer levels to normal values. Statistical significance was found with platelet count and D- Dimer parameters. Organizations like the ISTH has provided timely therapeutic information and guidance to clinicians in combating SARS-CoV2 related clinical manifestations. These findings serve to illuminate the nexus between ISTH VITT guidelines and clinical adaptation.
Introduction
Since the WHO announced the SARS-CoV2 was a pandemic in March of 2020, a race was on to develop a vaccine to combat the novel coronavirus [1]. Some of the companies that embarked on developing a vaccine included Moderna, Pfizer, Johnson & Johnson, and AstraZeneca. Moderna began clinical trials for their vaccine in March of 2020 revealing an efficacy rate of 94 percent in November of that year [2]. Pfizer started clinical trials in April of 2020 with results revealed in July that their candidate vaccine was more than 90 percent effective [3]. The Johnson & Johnson Ensemble Clinical Trial conducted in December 2020 revealed an efficacy of 72 percent in the US from their single-shot candidate vaccine [4]. Clinical trials for the AstraZeneca vaccine candidate began in August of 2020 resulting in an efficacy of 74 percent [5]. This paper will focus on the ChAdOx1-S vaccine developed by AstraZeneca and the University of Oxford Jenner Institute. The AstraZeneca COVID-19 Vaccine is a replication-deficient (i.e. inactivated) chimpanzee adenovirus vector encoding a trimeric pre-fusion form of the SARS-CoV-2 spike (S) protein. Following intramuscular administration these spike proteins are expressed locally, allowing the immune system to mount a neutralizing antibody/cellular immune response. This initial exposure and priming of the immune system subsequently provides protection against future infection [6]. The vaccine is administered intramuscularly in two doses with an interval of four to twelve weeks. In March of 2021, clinicians started to report that a scant number of recipients of the ChAdOx1-S vaccine developed VITT (Vaccine induced Thrombotic Thrombocytopenia) within two weeks of vaccination [7]. It has been posited that the mechanism of VITT involves negatively charged DNA particles binding to positively charged PF4 on the platelet membrane causing internalization within antigen presenting cells; subsequent production of antibody targeting the nucleic acid-PF4 complex ensues engendering thrombocytopenia and thrombosis in patients [8].
The International Society of Thrombosis and Haemostasis (ISTH) was created in 1969 with the mission of advancing the understanding, prevention, diagnosis, and treatment of conditions related to thrombosis and haemostasis. In April 2021, this body published guidelines for the Diagnosis and Treatment on VITT in which they articulated diagnostic imaging and a platelet count of <150 x 109/L is required to diagnose VITT in persons who have received the AstraZeneca ChAdOx1-S vaccine. Additionally, the guidance states that a D-dimer, PT, APTT, fibrinogen assay, and PF4 antibody immunoassay should be done on all patients suspected of VITT. Treatment recommendations include IVIG and non-heparin anticoagulation avoiding vitamin K antagonists and platelet transfusions unless the patient is undergoing surgery [9]. To facilitate adaptation of guidelines to clinicians their guidance also recommends disseminating information in the guidance to national and regional societies and organizations. This study serves to analyze select case reports of VITT in regard to diagnostic tests and treatment recommended by the ISTH and to determine if there is statistical significance between VITT select parameters and respective normal values.
Materials
Study Design
Ten case reports were identified using the PubMed database involving patients diagnosed with VITT, with no previous history or family history of bleeding diathesis (Table 1). Case reports were excluded if patients received any other SARS-CoV2 vaccine other than the AstraZeneca ChAdOx1 vaccine. Parameters studied from the case reports included fibrinogen, platelet count, PF4 immunoassay, and D-Dimer. In addition, treatments were compared and contrasted among cases. The lower limit reference value employed for the one- sample t-test for fibrinogen, platelet count, and D-Dimer were 200 mg/dL, 150 x 109/L, and 0.2 mg/L, respectively.
Demographics
Patients in selected case reports included five females and five males aged 26 to 61 years of age.
Statistics
A one-sample t-test was performed using SPSS (v28) to determine if there is statistical significance between the mean fibrinogen, platelet count, and D-dimer in the ten case reports and normal values. A P value less than 0.05 is considered statistically significant (Table 1).
| Year | Post-Vac Symptoms (days) | |
|---|---|---|
| Lin, et al. | 2021 | 5 |
| Aladdin, et al. | 2021 | 14 |
| Rawahi, et al. | 2021 | 7 |
| Fanni, et al. | 2021 | 13 |
| Mancuso, et al. | 2022 | 9 |
| Comer, et al. | 2022 | 15 |
| Ihnatko, et al. | 2022 | 2 |
| McDonnell, et al. | 2021 | 9 |
| Khuhapinant, et al. | 2021 | 8 |
| Corica, et al. | 2021 | 8 |
Table 1: Selected VITT Case Reports.
Results
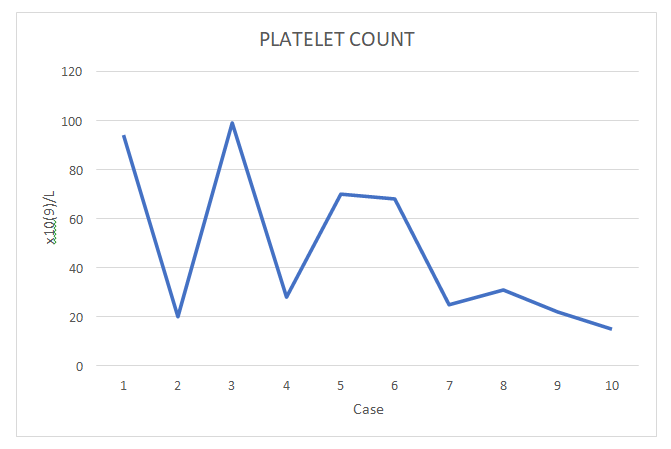
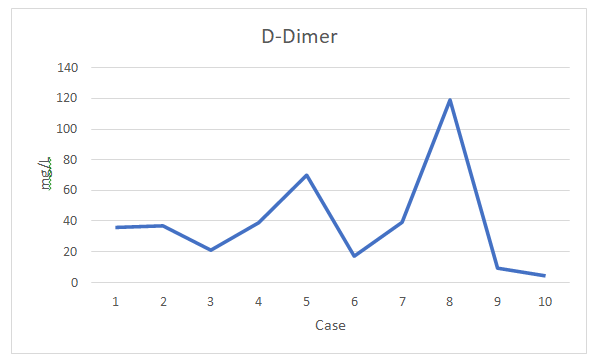
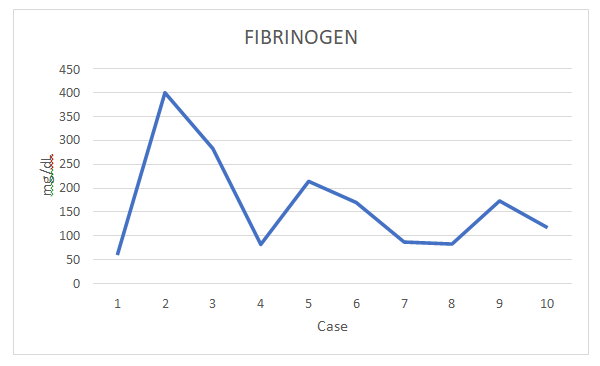
The average fibrinogen level among the ten cases was 166.9 mg/dL, the average platelet count was 47.2 x 109/L, and the average D-Dimer was 39.2 mg/L. The PF4 immunoassay was positive in all cases consistent with the diagnosis of VITT. The one sample t-test yielded statistically significant results for D-Dimer and the platelet count parameters (P<.05). Platelet counts ranged from 15 to 99 x 109/L (Figure 1), D-Dimer ranged from 4.3 to 119 mg/L (Figure 2), and fibrinogen levels ranged from 82 to 400 mg/dL (Figure 3).
Discussion
The incidence of VITT is estimated to range from 1 case per 26,500 to 1 case per 127,300 first doses of ChAdOx1 nCOV-19 administered, and 1 case per 518,181 second doses of vaccine administered [10]. All cases analyzed in this study evaluated patients for fibrinogen, platelet count, D-Dimer, and PF4 immunoassay as recommended by the ISTH. Radiographic imaging such as CT and MRI were carried out in all cases except for one; VITT was confirmed in that case by the PF4 immunoassay. Testing for the PT and APTT, as well as treatment modalities varied. Two cases did not include a PT or APTT, and three cases reported the INR in place of the PT. In the cases that did report the PT and APTT, three reported increased results. Unlike the platelet count, PF4 immunoassay, and D-Dimer parameters which were abnormal in all cases, the values for fibrinogen, PT, and APTT were variable. All case reports indicated IVIG was administered to ameliorate the thrombocytopenia in patients and raise the platelet count.
Anticoagulants employed by clinicians included fondaparinux, apixaban, dabigatran, and argatroban. The number of days to presentation of symptoms after receiving the ChAdOx1 vaccine ranged from 2 days to 14 days. Presentation symptoms such as headache, fever, abdominal pain, and nausea were similar across studies and aligned to the ISTH guidance on VITT. Emboli were found through radiographic studies in the pulmonary arteries, cerebral arteries, orbit, superior sagittal sinus, renal vein, and descending aorta.
The dissemination of the ISTH guidelines to clinicians was very effective and timely in view of the cases discussed and reporting of the first cases of VITT in March of 2021. At that juncture the WHO and EMA (European Medicines Agency) articulated to the public that the benefits outweigh the risks regarding the ChAdOx1 vaccine and rare cases of VITT; nonetheless select countries [Germany, France, Italy] briefly suspended vaccinations. The WHO has further articulated that the frequency of thrombus events is very rare and national regulators continue to monitor cases closely and update the public on changes to incidence [11]. While this study focused on the AstraZeneca vaccine, another Adenovirus vector vaccine was developed by Johnson & Johnson named AD26.COV2S. Cases of VITT have also been reported with the Johnson & Johnson vaccine. The responses by regulatory agencies like the WHO and FDA took the same posture as with the AstraZeneca vaccine deciding not to pause vaccinations. The expedient response by national and international medical groups and organizations in devising appropriate diagnostic information, presentation of symptoms, and effective treatment for VITT patients has led to amelioration of manifestations and clinical improvement.
The SARS-CoV2 pandemic has brought enumerable challenges to the public and healthcare sphere that prompted and compelled companies to harness their knowledge, experience, and ingenuity toward production of an effective vaccine that could be made available to the public after clinical trials had been performed and efficacy determined. As the last pandemic was more than 100 years ago the public was effectively navigating unchartered waters and relied on medical experts and their respective governments for guidance on strategies for slowing the spread of COVID-19. Organizations like the ISTH played in pivotal role in a plethora of issues surrounding the pandemic including the topic of this paper on detecting and managing patients with VITT who were administered the AstraZeneca vaccine. Their expert membership and committee compositions, visibility, and expediency provided clinicians with a blue print for treating and managing VITT patients effectively which aligned to other regulatory organizations and the decision to continue to disseminate the AstraZeneca vaccine globally.
References
-
WHO (2020) WHO Director-General’s opening remarks at the media briefing on COVID-19, World Health Organisation.
-
Bosely S (2020) Moderna Covid Vaccine has 94% efficacy, final results confirm. Support the Guardian .
-
Preidt R (2021) Pfizer vaccine 90% effective against severe COVID-19 for at least 6 months: Study. US News.
-
Mascellino MT, Di Timoteo F, De Angelis M, Oliva (2021) A Overview of the main anti-SARS-CoV-2 vaccines: mechanisms of action, efficacy, and safety. Infect Drug Resist 14: 3459-3476.
-
Knoll MD, Wonodi C (2021) Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 397(10269): 72- 74.
-
Emary KR, Golubchik T, Aley PK, Ariani CV, Angus B et al. (2021) Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS- CoV-2 variant of concern 202012/01 (B.1.17): an exploratory analysis of a randomized controlled trial. Lancet 397(10282): 1352-1362.
-
Pottegard, Lund LC, Karlstad O, Dahl J, Andersen M, et al. (2021) Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. BMJ 373: n1114.
-
McGonagle D, De Marco G, Bridgewood C (2021) Mechanisms of immunothrombosis in Vaccine-induced thrombotic thrombocytopenia (VITT) compared to natural SARS-CoV-2 infection. J Autoimmun 121: 102662.
-
(2022) International Society onThrombosis and Haemostasis.
-
Chan B, Odutayo A, Juni P, Stall NM, Bobos P, et al. (2021) Risk of Vaccine-Induced Thrombotic Thrombocytopenia (VITT) following the AstraZeneca/COVISHIELD Adenovirus Vector COVID-19 Vaccines, pp: 1-4.
-
WHO (2022) For a safer, healthier and fairer world, World Health Organisation.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies