Circulating Megakaryocytes in Peripheral Blood: A Clue to Satisfactory Platelet Recovery Post Induction Chemotherapy in Acute Myeloid Leukemia
Thrombocytopenia is a common hematological abnormality in newly diagnosed acute myeloid leukemia (AML) which may be linked to the degree of marrow infiltration by leukemic blasts as well as altered cytokine milieu in a subset of AMLs. We report the presence of circulating megakaryocytes in peripheral blood as a sign of satisfactory platelet recovery post induction chemotherapy in a pediatric subject with a favourable risk WHO category I AML with synchronous extramedullary myeloid cell tumor; and present a brief review of literature on the role of platelet recovery in AML prognosis.
Introduction
Acute myeloid leukemia is a diverse group of clonal hematopoietic neoplasm characterised by proliferation of myeloid progenitors in the bone marrow; distinct molecular and immunophenotypic signature; and unpredictable biological behaviour and outcome following intensive chemotherapy. The risk stratification in AML relies heavily on combination of clinicohematological parameters, baseline immunophenotypic profile, and the underlying cytogenetic and/or molecular abnormalities that drive tumorigenesis; which in turn predict final outcome [1]. Recent introduction of next generation sequencing (NGS) based molecular testing have improved the identification of persisting molecular mutations in remission samples, with some of them predicting higher risk of relapse [2]. There have been sporadic studies which have tried to elucidate the role of platelet recovery following induction chemotherapy in AML subjects and tried to correlate the same with associated molecular alterations [3, 4].
In January 2021, a 13-year-old male child presented to the Out Patient Department of Medical Oncology/ Hematology of our Institute with a one-month history of gradual onset swelling (4 x 3 cm) over left lower back associated with pain, fever, and difficulty in walking for last fifteen days duration. Fine needle aspiration cytology of the lump revealed a malignant blue round cell tumor comprising of monotonous population of intermediate size tumor cells with scant to moderate, finely granular cytoplasm; occasional ones showing slender Auer rods; fine nuclear chromatin and multiple nucleoli; thus, consistent with a diagnosis of blastic extramedullary myeloid cell tumor (EMMT). His baseline routine hematological investigation at the time of initial presentation revealed normocytic normochromic anemia [hemoglobin (Hb); 85 g/L (ref.; 120- 140 g/L), mean corpuscular volume; 88 fL (ref.; 80 - 98 fL)], total leukocyte count (TLC); 8.9 x 109/L (ref.; 4 – 11 x 109/L) with 08% myeloid blasts in peripheral blood smear examination; and thrombocytopenia [platelet count (Plt); 80 x 109 /L; ref.; 150 - 450 x 109 /L]. His stained bone marrow aspirate (BMA) smears from right posterior superior iliac spine were hypercellular for age with presence of 40% myeloperoxidase (MPO) positive myeloid blasts with obvious Auer rods, maturing myeloid lineage comprising of > 10% marrow nucleated cell differentials; and suppressed erythroid and megakaryocytic lineage. These features were consistent with a diagnosis of acute myeloid leukemia (AML) with maturation. Conventional G-banding cytogenetic analysis of BMA sample revealed translocation t (8:21) (q22; q22); thus, consistent with a favourable risk WHO category I AML with synchronous EMMT of left lower back. He was started with cytarabine, daunorubicin and etoposide-based induction regimen as per UK MRC protocol with complete disappearance of back swelling.
His complete blood count at the time of day 33 (D33) follow up marrow evaluation revealed the following: Hb; 109 g/L, TLC; 5.2 x 109 /L with maintained differential count, no circulating blasts; and thrombocytosis (Plt; 550 x 109 /L). Peripheral blood smear examination revealed numerous large platelet clumps as well as scattered bare megakaryocytic nuclei and nuclear fragments at the feathered edges of the smear (Figures 1a, 1b). Follow up BMA and trephine biopsy demonstrated a low normal cellularity for age (average; 50%) with adequate and normally distributed maturing myeloid and erythroid elements and increased number of morphologically normal megakaryocytes (Figure 1c). There was no evidence of excess myeloid blasts or localized interstitial collections as confirmed by negative immunohistochemical staining for CD 34, CD 117, and MPO. The morphological and immunohistochemical features were suggestive of a regenerating marrow (post induction), and the patient was continued with scheduled next cycle chemotherapy. Conventional cytogenetic analysis performed on D33 BMA sample did not show translocation t (8:21) (q22; q22); and molecular testing was not performed due to financial constraints. He has no evidence of relapse or residual disease at sixteen-month post diagnosis.
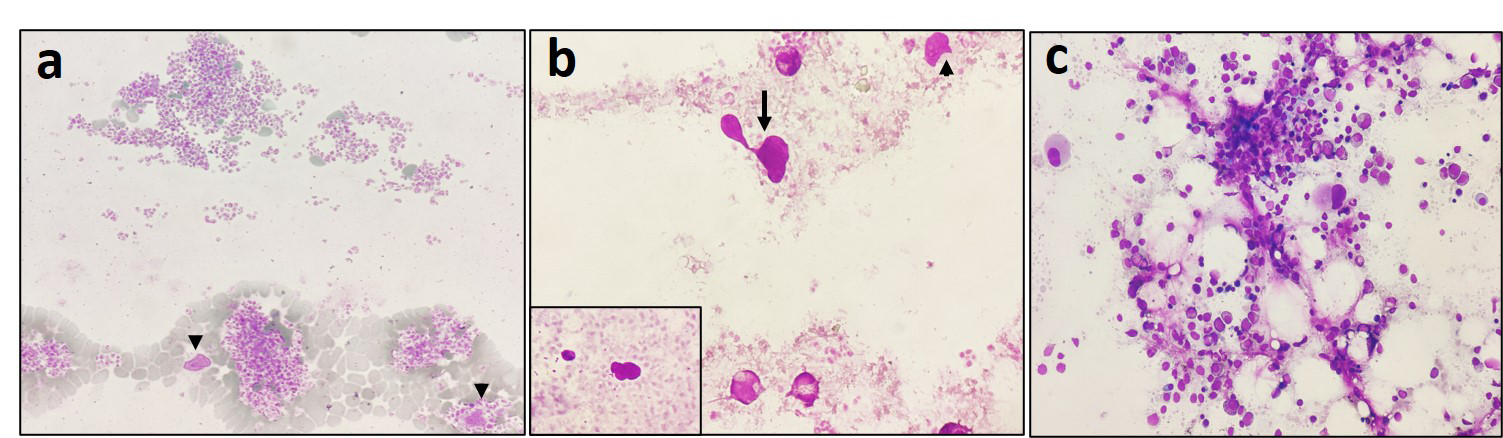
Figure 1: Peripheral blood smear from the case at the time of post induction bone marrow evaluation: Note the presence of large platelet clumps (a, x200) with scattered bare megakaryocytic nuclei (b, black arrow, and inset, x400) and nuclear fragments (black arrow head in a, b) at the tail end of the smear. Bone marrow aspirate smears (c, x400) showing low normal cellularity for age with maintained and adequate trilineage hematopoiesis and no excess blast suggestive of regenerating marrow. Leishman-Giemsa stain (a, b, c).
Discussion
Circulating bare megakaryocyte nuclei are unusual findings which may be rarely encountered in conditions such as reactive thrombocytosis of iron deficiency anemia and post dengue fever; myelodysplasia; or even in chronic myeloproliferative neoplasms such as chronic myeloid leukemia, essential thrombocythemia (ET), or even in primary myelofibrosis [5, 6]. Megakaryocytes circulating in peripheral circulation may be a normal (physiological) phenomenon considering the outcome from invitro studies performed on lung cancer subjects where it was demonstrated that megakaryocytes leave bone marrow to be circulated in pulmonary arterial circulation before getting arrested in pulmonary capillaries in order to shed platelets. Therefore, pulmonary capillaries may serve as a gateway to peripheral blood for megakaryocytes [7].
Implication of circulating bare megakaryocyte nuclei in AML is not fully clear; and this may represent a satisfactory marrow recovery following induction chemotherapy. Previous studies in AML subjects have reported that good platelet recovery or even rebound thrombocytosis (RT) (> 500 x 109/L) post induction to be an independent predictor of good overall survival (OS) and disease-free survival (DFS) in such subjects [3]. Schnell and colleagues [4] in their cohort of AML (N=291) reported that rebound thrombocytosis was inversely correlated with degree of thrombocytopenia; RT+ patients were more likely to have mild thrombocytopenia (<100 x 109/L) or severe thrombocytopenia (<20 x 109/L). There was no significant association between post induction platelet recoveries with parameters such as age, gender, serum LDH, marrow tumor burden, blast morphological phenotype, or leukocyte count. RT was common among NPM1 mutated (P=0.022) and European Leukemia Net (ELN) favorable subgroup (P<0.0001) where as those with complex karyotypes and adverse ELN category (P < 0.0001) had poor Plt recovery post induction. WHO category I AML [t (8; 22), t (15; 17), inv (16), NPM1 mutated, CEBPA muted] had better platelet recovery (≥ 500 x 109/L) compared to adverse cytogenetic abnormalities (lowest for chromosome 7 alteration group, P=0.0018). RT (+) group had a superior overall survival (OS) (median 125 vs 41 months, log rank P = 0.0497) and disease-free survival (DFS) (log rank P = 0.0622) than RT (-) sub group. Transcription factors favouring late megakaryocytic differentiation such as NFE2 was reported to be upregulated in RT (+) subgroup pointing to a pathophysiologic link. There was no correlation of RT with expression levels of MPL, GATA1, and GATA2 in mononuclear cells at diagnosis. There were negative correlations between platelet recovery with expression levels of MYB, KLF4, and NF1A genes, with significant differences of expression levels of all three markers between RT (+) and RT (-) subgroups. On multivariate Cox proportion analysis, platelet count of ≥ 500 x 109/L post induction (P=0.031) [95% Confidence Interval (CI): 0.592–0.902], age at diagnosis (P=0.023, CI: 1.004– 1.052), and ELN subgroup (P=0.018, CI: 0.336–0.779) were found to be independent predictor of survival [4].
In summary, circulating megakaryocytes in peripheral blood may be an indicator of satisfactory platelet recovery post induction chemotherapy in acute myeloid leukemia which may have an impact on outcome. Satisfactory platelet recovery post induction chemotherapy may be associated with favourable molecular phenotypes in AML.
References
-
Arber DA, Brunning RD, Le Beau MM, Falini B, Vardiman JW, et al. (2017) Acute myeloid leukemia with recurrent genetic abnormalities. In: Swerdlow SH, Campo E, et al. (Eds), classification of hematopoietic and lymphoid tissues. Revised 4th Edn, World Health Organization IARC, Lyon.
-
Jongen-Lavrencic M, Grob T, Hanekamp D, Kavelaars FG, Al Hinai A, et al. (2018) Molecular minimal residual disease in acute myeloid leukemia. N Engl J Med 378(13): 1189-1199.
-
Malkan UY, Gunes G, Isik A, Eliacik E, Etgul S, et al. (2015) Rebound thrombocytosis following induction chemotherapy is an independent predictor of a good prognosis in acute myeloid leukemia patients attaining first complete remission. Acta Haematol 134(1): 32-37.
-
Schnell BR, Seipel K, Bacher U, Jeker B, Mueller BU, et al. (2019) Rebound thrombocytosis after induction chemotherapy is a strong biomarker for favorable outcome in AML patients. HemaSphere 3:2.
-
Ku NK, Rashidi H (2017) Unusual finding of a megakaryocyte in a peripheral blood smear. Blood 130(23): 2573.
-
Garg N, Gupta RJ, Kumar S (2019) Megakaryocytes in peripheral blood smears. Turk J Haematol 36: 212-213.
-
Dejima H, Nakanishi H, Kuroda H, Yoshimura M, Sakakura N, et al. (2018) Detection of abundant megakaryocytes in pulmonary artery blood in lung cancer patients using a microfluidic platform. Lung Cancer 125: 128-135.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies