Knowledge of Premarital Genotype Screening Among Women Receiving Care at a Tertiary Centre in Ebonyi State, Nigeria
Background: Sickle cell disease is a major genetic disease with the greatest burden in sub-Saharan Africa, of which Nigeria is the epicenter. Premarital genotype screening for sickle cell disease is a tool of immense value in the prevention of the condition. This study sought to determine the level of knowledge on premarital genotype screening among women, identify their perceived relevance of premarital genotype screening in a bid to identify gaps in knowledge and provide basis for evidence based interventions. Methods: A descriptive cross-sectional study design was used, with the data collected using structured, intervieweradministered questionnaire. A total of 680 questionnaires were administered and retrieved. Results: The majority of respondents, 452(66.5%) were between 25-34 years while 506 (74.9%) had a tertiary education and predominant tribe and religion was Igbo and Christianity. About 85% were aware of SCD while about a quarter 183(26.9%) have no knowledge of premarital genotype screening sickle cell disease the premarital screening for the disease. Less than half, 227(45.7%) correctly knows that the relevance of premarital genotype screening. Almost half had negative attitude towards the premarital screening, with 88.97% recommending that the screening be made compulsory for all intending couples. Most (72.76%) of the respondents carried out the premarital screening when they got married. The educational attainment and previous knowledge of genotype status of the respondents significantly influenced the uptake of the screening (p-value = 0.0001, p=0.004 respectively). Conclusion: The level of awareness of premarital genotype screening did not translate to good knowledge since a good number of the respondents’ demonstrated negative perception towards its relevance. Public health education is needed to correctly deploy premarital genotype screening in reducing SCD burden.
Introduction
Sickle cell disease is a monogenic disorder that affects millions of people worldwide. Sickle Cell Disease (SCD) occurs when an individual has inherited two mutants (abnormal haemoglobin) (Hb) genes from both parents, at least one of which is HbS. The abnormal haemoglobin (HbS) is due to the substitution of glutamic acid with valine at position 6 of the β-globin chain of the adult human haemoglobin (HbA) [1]. This leads to the formation of haemoglobin molecule that is functionally unstable. When deoxygenated, the HbS haemoglobin polymerizes and form tactoids that distorts the red cell membrane leading to sickle shape change which causes shortened life span of the red blood cell and blockage of the small blood vessels. SCD is characterized by haemolytic anaemia, vaso-occlusive crises, relentless end organ injury and premature death. Homozygous inheritance of HBS produces the severest form of the disease- sickle cell anaemia (SCA). Sickle cell disease is the most prevalent genetic disease worldwide. Nigeria parades the largest burden of the disease with over 4 million persons living with the disease and 1 in 4 persons being carriers of sickle cell trait with the prevalence of about 20 per 1000 live births [1]. Sickle cell disease is a disease of public health concern because of the significant morbidity and under five mortality associated with it [2, 3]. Despite Public education intervention, recent studies have shown that the prevalence of SCD in Nigeria is yet to achieve appreciable reduction [4, 5]. Sickle cell disease is a preventable disease that imposes enormous pressure over healthcare institutions, creates psychosocial and financial problems for families of suffers and the community at large.
Premarital genotype screening is a vital tool in prevention of SCD. Premarital genotype screening is a medical test carried out for couples about to get married in order to determine their haemoglobin phenotype and compatibility. This provides them opportunity to make informed decision to prevent sickle cell diseases in the offspring [6]. Sickle cell trait (AS) is a risk factor for procreating children with SCD yet research has shown a poor awareness of genotype among mothers [7]. This may not be unrelated to the poor level of health information literacy among women in Nigeria [8]. In most developing countries, a high percentage of many women are not educated and adequate knowledge has been shown to lead to prevention of heritable diseases [9, 10]. Genetic diseases like sickle cell disease is more prevalent in developing countries like Nigeria. Studies on knowledge of women on premarital genotype testing in Ebonyi state is lacking. This study sought to determine the level of knowledge on premarital genotype screening among women, identify their perceived relevance of premarital genotype screening in a bid to identify gaps in knowledge and provide basis for evidence based interventions.
Materials and Methods
Study design: This was a hospital based descriptive cross- sectional study carried out among women attending the antenatal clinic of the Alex Ekwueme Federal University teaching hospital Abakaliki, Ebonyi State.
Sample size calculation: A sample size of 680 was obtained using the Right Size software. This was based on confidence level of 95%, confidence limit of 0.05, design effect of 1.5, 90% anticipated response rate and finding of 41.4% prevalence rate of good knowledge of premarital genotype screening reported in the study by Otovwe, et al. [11].
Study Tool: Demographics and awareness on premarital genotype screening was collected using closed-ended, interviewer-administered questionnaire with 20 questions (Annex 1).The questionnaire was in two sections: the first section focused on the socio-demographic characteristics of the respondents (age, sex, marital status and religion); the second section sought to establish respondents’ knowledge about premarital genotype screening for SCD.
Data analysis: Data entry and cleaning were performed prior to analysis using Microsoft Excel. Data were analyzed using IBM SPSS version 21 for Windows. Data presentation involved frequency tables and charts. Univariate and multivariate logistic regression were employed to identify correlates of knowledge of premarital genotype screening. Odds ratios with 95% confidence intervals were determined. A p-value of less than 0.05 was considered statistically significant.
Ethical consideration: This study was approved by the Research Ethics Committee of Alex Ekwueme Federal University Teaching Hospital Abakaliki. Written informed consent was obtained from all participants.
Results
(Table 1) A total of 680 women gave consent for the study and completed their questionnaires. The majority of participants; 452(66.5%) were between 25-34 years while 506 (74.9%) have attained tertiary level of education. The predominant tribe and religion was Igbo and Christianity respectively. About 85% have heard about sickle cell disease while 14.1% have no knowledge about it and only 5% have a family relation with sickle cell disease. Most, 622(91.5%) expressed knowledge of their genotype while 58(8.5%) doesn’t know theirs. Of the 622 participants aware of their genotype, the distribution shows 491(78.9%) have genotype AA, 128(20.6) have genotype AS while 3(0.5%) have genotype SS.
| Absolute number | Relative frequency (Percent) | |
|---|---|---|
| Age categories | ||
| 15 - 24 years | 82 | 12.1 |
| 25 - 34 years | 452 | 66.5 |
| 35 - 44 years | 144 | 21.1 |
| 45 - 54 years | 2 | 0.3 |
| Level of education | ||
| Nil | 3 | 0.4 |
| Primary | 32 | 4.7 |
| Secondary | 136 | 20 |
| Tertiary | 509 | 74.9 |
| Tribe | ||
| Igbo | 657 | 96.7 |
| Ijaw | 3 | 0.4 |
| Isoko | 2 | 0.3 |
| Yoruba | 2 | 0.3 |
| Others* | 16 | 2.3 |
| Religion | ||
| Christianity | 677 | 99.6 |
| Not specified | 3 | 0.4 |
| Heard about sickle cell disease | ||
| Yes | 584 | 85.9 |
| No | 96 | 14.1 |
| Relation with sickle cell disease | ||
| Yes | 34 | 5 |
| No | 646 | 95 |
| Genotype status known | ||
| Yes | 622 | 91.5 |
| No | 58 | 8.5 |
| Genotype among those with known status** | ||
| AA | 491 | 78.9 |
| AS | 128 | 20.6 |
| SS | 3 | 0.5 |
| SC | 0 | 0 |
Table 1: Findings on socio-demographic and genotype information of respondents. *Others- Idoma, Efik, Igala **Based on a denomina
Figure 1 Demonstrates that about a quarter of the participants have no knowledge of premarital genotype screening for sickle cell disease. From the 497 (78.1%) who have heard about premarital genotype screening for SCD, only 227(45.7%) correctly knows that its main relevance is to guide your decision on choosing compatible marriage mate while 30(6%) thinks its importance is just to make one know her SCD status. Almost half exhibited negative perception toward premarital genotype screening. Out of which, 193(38.8%) believed it can cause problems or family tension if their genotypes were not compatible while 47(9.5%) were unconcerned about its relevance.
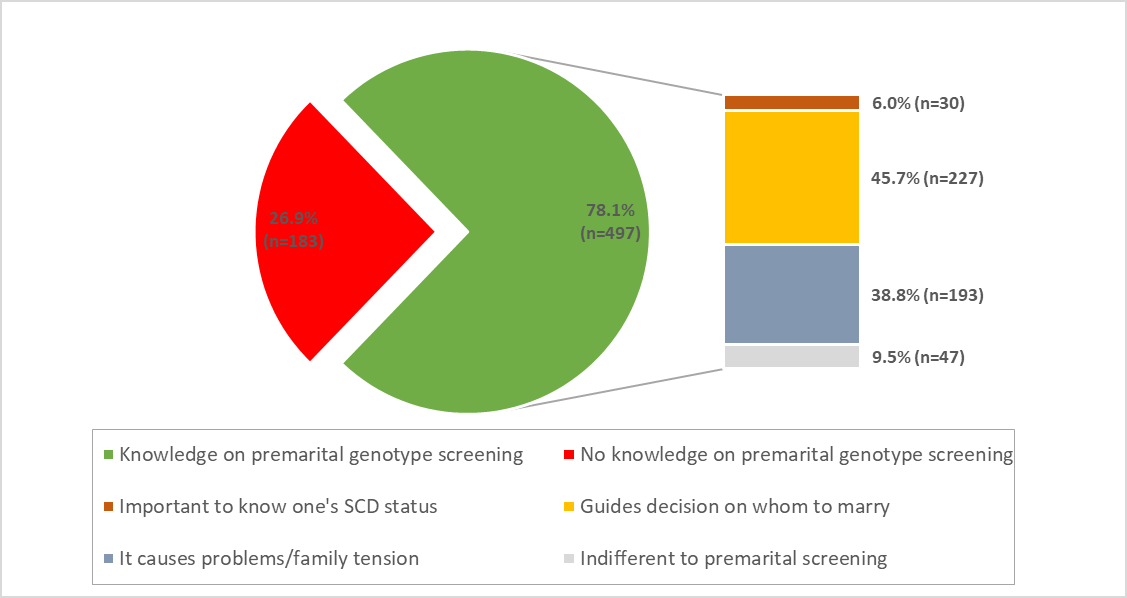
Table 2 Univariate and multivariate analysis revealed that educational levels and previous knowledge of genotype status were good predictors of knowledge on premarital genotype screening with a statistically significant value of p<0.05, however educational level had a stronger relationship.
| Variables | Knowledge on premarital genotype screening | Univariate | Multivariate | |||
|---|---|---|---|---|---|---|
| Yes n (%) | No n (%) | cOR (95% CI) | P | aOR(95% CI) | P | |
| Age | ||||||
| 15 – 24 years | 55 (67.1) | 27 (32.9) | 0.90 (0.67- 1.20) | 0.477 | 1.00 (0.75-1.36) | 0.957 |
| 25 – 34 years | 335 (74.1) | 117 (25.9) | ||||
| 35 – 44 years | 106 (73.6) | 38 (26.4) | ||||
| 45 – 54 years | 1 (50.0) | 1 (50.0) | ||||
| Education | ||||||
| Nil | 2 (66.7) | 1 (33.3) | 2.26 (1.56- 3.28) | 0.0001* | 2.09 (1.41-3.10) | 0.0001* |
| Primary | 18 (56.2) | 14 (43.8) | ||||
| Secondary | 83 (61.0) | 53 (39.0) | ||||
| Tertiary | 394 (73.1) | 183 (26.9) | ||||
| Known genotype status | ||||||
| Yes | 464 (74.6) | 158 (25.4) | 2.23 (1.28- 3.86) | 0.004* | 1.60 (0.89-2.86) | 0.117 |
| No | 33 (56.9) | 25 (43.1) | ||||
| Having a relation with SCD | ||||||
| Yes | 28 (82.4) | 6 (17.6) | 1.76 (0.71- 4.33) | 0.217 | 1.83 (0.74-4.57) | 0.192 |
| No | 469 (72.6) | 177 (27.4) |
Table 2: Univariate and multivariate analyses of factors related to knowledge on premarital genotype screening among study partic
Discussion
Nigeria has about 25% prevalence rate of carriers of the sickle cell gene, while about 2% of all the newborns in Nigeria are born with the sickle cell disease. Premarital genotype screening for sickle cell disease is a tool of immense value in the prevention of the condition. Its relevance in abating the societal burden of sickle cell disease cannot be over- emphasized. Awareness of mothers about their premarital genetic testing should influence their partner selection, guide their information transmission to their children and modify their health seeking behavior for medical and other risk factors that may impact pregnancy outcomes through prevention and treatment [12].
This study revealed that majority of the study participants was aware of sickle cell disease and premarital genotype screening. More than 80% have heard about SCD while 78.1% know about premarital genotype screening. Our finding agrees with previous studies where over 90% of the study population was aware of SCD and premarital genotype screening [13, 14, 15]. The high level of awareness for SCD by the participants in this study could reflect the knowledge base of the population due to sustained public enlightenment on SCD and their educational level [16]. Nigeria has the highest burden of sickle cell disease in the world; hence it has received robust publicity by stakeholders [17]. Over 90% of the respondents in this study had at least a secondary school education which could have played a role in their awareness for SCD and premarital screening. Obviously, the under-representation of participants with no formal education or only primary education could be explained by the fact that the study was carried out among women in the urban populace where awareness and access to education is high. Our finding of a majority being aware of SCD and premarital screening is in agreement with that of a study in Oman in which all the participants had at least a high school education and 89.3% knew about premarital genotype screening [18]. Abogaye, et al. in their study also reported that 50% of their participants heard about sickle cell from the school [19]. Similarly another contributory factor for the increased awareness of premarital genotype screening for SCD could be because almost all the study participants belong to the Christian religion where many churches have premarital screening as one of the mandatory prerequisite for couples to be joined in marriage [20]. This requirement enables the religious bodies to discourage marriages between incompatible couples thereby making them critical stakeholders in reducing the burden of SCD [21, 22]. It is advocated that other institutions that contract marriages for couples should adopt such regulations to complement the campaign effort to reduce SCD burden in Nigeria. Contrary to our finding on level of awareness for premarital genotype screening and SCD, a study in Plateau State, Nigeria, revealed that only 62% have heard of genetic disease, and just about half of the participants knew about premarital genotype screening probably due to the lower proportion of participants with tertiary education (44%) in the rural area of study [23]. Educational levels and previous knowledge of genotype status were good predictors of knowledge on premarital genotype screening. Education is important for improved well-being.
It is unsurprising that the majority of those who were knowledgeable about premarital genotype screening also knew their genotype status. This is probably because the knowledge of premarital screening can act as a catalyst for genotype testing. Most of the participants (91.5%) knew their genotype status of which 0.5% and 20.6% were SS and AS respectively. This proportion of carrier status for sickle cell disease is comparable to the documented prevalence of 24% for AS and SS in a previous study on prevalence of sickle cell disease in premarital screening in southwest, Nigeria [24]. It is a welcomed development that a majority of the women know their genotype unlike a report from Ghana where 68.5% of those studied did not know their sickling status [19]. There is a 25% chance marriage between SCD carriers (genotype AS) will result in a pregnancy with a child affected with sickle cell anaemia (SS). Premarital haemoglobin screening is an important strategy for the control of Sickle Cell Disease.
This study demonstrates that there is yet some knowledge gap to be filled regarding premarital genotype screening since 26.9% of study participants had no knowledge of premarital genotype screening and 14.1% have not even heard about sickle cell disease. This is unacceptable for a country like Nigeria with the highest burden of SCD. More so, less than half of the women in our study know that the importance of premarital genotype screening is to guide contracting marriage with a partner with a compatible genotype. Almost half of the respondents exhibited negative perception toward premarital genotype screening. They believed it can cause problems or family tension if their genotypes were not compatible while some felt that their premarital genotype screening result will not influence their choice of marriage partner. Our finding does not agree with the reports by Abioye-Kuteyi, et al. where almost all the respondents demonstrated a good attitude toward premarital genotype screening [25]. However it agrees with findings of Otovwe, et al. whose respondents opined that premarital genotype screening could reduce their chances of marriage [11]. The censure associated with sickle cell disease can make it difficult to entrench premarital genotype screening as exhibited in this study. There should be a re-modification of sickle cell disease enlightenment campaigns to be able to disabuse the minds of the populace on the wrong perception of premarital genotype screening. Premarital screening is intended to educate the couple and offer them accurate and unbiased information to assist them in making an informed decision to avoid having children with sickle cell disease.
Our study showed that educational level and previous knowledge of one’s genotype have positive correlation with the knowledge of premarital genotype screening. This shows that knowledge and relevance of premarital genotype screening is better among those with tertiary education since it’s expected that the higher one goes in educational level, from no formal education to tertiary education levels, the more knowledge is acquired. This was also opined by Ugwu in her study on awareness of premarital genotype screening among undergraduate university students that revealed that 91.2% were aware and lectures were the most frequent source of information [26]. This indicates the necessity of functional education. This is expected since education empowers an individual to access, understand and apply information from different sources such as schools, paper and electronic media. An educationally empowered woman is well disposed to acquire and implement the necessary information about her health and that of the society at large [27]. Comprehensive knowledge about sickle cell disease and its prevention through genotype screening should be taught at all levels of education including informal education settings. Genotype screening should be introduced as a mandatory test as early as at birth or primary school and individuals made aware of their genotype and counseled so that it can influence them to request for it while choosing a procreation partner.
Limitations of the study
The outcome of this study was based solely on the responses of the women which could be subject to bias.
In conclusion, most of the study participants are aware of premarital genotype screening especially among those with higher education levels. Almost half demonstrated negative perception towards the relevance of premarital genotype screening. This calls for concerted efforts in massive campaigns and public education on the importance of premarital genotype screening. Genetic education and counseling should be employed as a part of the components of public health education.
Conflicts of Interest: None to declare.
Acknowledgement: The authors wish to appreciate the scientific officers in haematology department AEFUTHA, for their assistance in administering the questionnaires to the mothers.
Funding: The authors fully funded this work.
References
-
Inusa BPD, Hsu LL, Kohli N, Patel A, Evbota KO, et al. (2019) Sickle Cell Disease-Genetics, Pathophysiology, Clinical Presentation and Treatment. Int J Neonatal Screen 5(2): 20.
-
Galadanci N, Wudil BJ, Balogun TM, Ogunrinde GO, Akinsulie A, et al. (2014) Current Sickle cell disease management practices in Nigeria. Int Health 6(1): 23-28.
-
Lubeck D, Agodoa I, Bhakta N, Danese M, Pappu K, et al. (2019) Estimated Life Expectancy and Income of Patients With Sickle Cell Disease Compared With Those Without Sickle Cell Disease. JAMA Netw Open 2(11): e1915374.
-
Diwe K, Iwu AC, Uwakwe K, Duru C, Merenu I, et al. (2016) Prevalence and patterns of sickle cell disease among children attending tertiary and non-tertiary health care institutions in a South Eastern state, Nigeria: A 10 year survey. J Res Med Dent Sci 4(3): 183-189.
-
Ambe JP, Mava Y, Chama R, Farouq G, Machoko Y (2012) Clinical features of sickle cell anaemia in northern nigerian children. West Afr J Med 31(2): 81-85.
-
Memish ZA, Saeedi MY (2011) Six-year outcome of the national premarital screening and genetic counseling program for sickle cell disease and β-thalassemia in Saudi Arabia. Ann Saudi Med 31(3): 229-335.
-
Ezenwosu OU, Itanyi IU, Nnodu OE, Ogidi AG, Mgbeahurike F, et al. (2021) Community based screening for sickle haemoglobin among pregnant women in Benue State, Nigeria: I-Care-to-Know, a Healthy Beginning Initiative. BMC Pregnancy Childbirth 21(1): 498.
-
Ekoko ON (2020) An Assessment Of Health Information Literacy Among Rural Women In Delta State, Nigeria. Library Philosophy and Practice.
-
Abubakar S, Lawan UM, Mijinyawa MS, Adeleke SI, Sabiu H (2010) Perceptions about sickle cell disease and its prevention among undergraduates of tertiary institutions in Kano state, Nigeria. Niger J Clin Med 3(1).
-
Alabi T, Alabi OS (2014) Female education: A sociological analysis of girl-child education in Nigeria. Int J Edu Pol Res Rev 1(1): 6-13.
-
Otovwe A, Sunday UI, Oghenenioborue Rume OB, Awulo DM (2019) Knowledge and Attitude of Premarital Genotype Screening Among Women of Child-Bearing Age in Kumo-Akko Local Government Area of GombeState Nigeria. Open J Public Health 1(2).
-
Odelola JO, Adisa O, Akintaro OA (2013) Attitude towards pre-marital genetic screening among students of Osun State Polytechnics in Nigeria. International Journal of Educational Administration and Policy Studies 5(4): 53- 58.
-
Adewoyin AS, Alagbe AE, Adedokun BO, Idubor NT (2015) Knowledge, Attitude and Control Practices of Sickle Cell Disease among Youth Corps Members in Benin City, Nigeria. Annals of Ibadan Postgraduate Medicine 13(2): 100-107.
-
Omuemu VO, Obarisiagbon OE, Ogboghodo EO (2013) Awareness and acceptability of premarital screening of sickle cell disease among undergraduates of university of Benin, Benin City. Journal of biomedical sciences 12(1): 91-104.
-
Gbeneol PK, Brisibe SF, Ordnioha B (2015) Knowledge, attitude and uptake of premarital screening for the Sickle trait among married couples in a semi-Urban Community in south-South Nigeria. Eur J Prev Med 3(3): 49-54.
-
Nnachi OC (2022) Maternal knowledge of sickle cell disease and its predictors in southeast Nigeria. J Bas Med Clin Sc 1(1): 19-26.
-
Aygun B, Odame I (2012) A global perspective on the sickle-cell disease. Pediatric Blood & Cancer 59(2): 386- 390.
-
Al Farsi OA, Al Farsi YM, Gupta I, Ouhtit A, Al-Farsi KS, et al. (2014) A study on knowledge, attitude, and practice towards premarital carrier screening among adults attending primary healthcare centers in a region in Oman. BMC Public Health 14: 380.
-
Aboagye JA, Aboagye QQ (2019) Sickle cell awareness, Depth of Knowledge and Attitude Towards Premarital Screening Among Students in Ghana. Afr J Mgt Res 26: 107-119.
-
Criminal Code Act (2022) Federal Republic of Nigeria criminal code.
-
Abubakar S, Lawan UM, Mijinyawa MS, Adeleke SI, Sabiu H (2010) Perceptions about sickle cell disease and its prevention among undergraduates of tertiary institutions in Kano state, Nigeria. Niger J Clin Med 3(1).
-
Dennis Antwi JA, Ohene Frempong K, Anie KF, Dzikunu H, Veronica A, et al. (2018) Relation Between Religios Perspectives and Views on Sickle Cell Disease Research and Associated Public Health Intervention in Ghana. J Genet Couns.
-
Oyedele EA, Emmanuel A, Gaji LD, Ahure DE (2015) Awareness and acceptance of premarital genotype screening among youths in a Nigerian community. International Journal of Medical and Health Research 1(1): 17-21.
-
Nnaji GA, Ezeagwuna DA, Nnaji I, Osakwe JO, Nwigwe AC, et al. (2013) Prevalence and pattern of sickle cell disease in premarital couples in Southeastern Nigeria. Niger J Clin Pract 16(3): 309-314.
-
Abioye Kuteyi EA, Oyegbade O, Bello I, Osakwe C (2009) Sickle cell knowledge, premarital screening and marital decisions among local government workers in Ile-Ife, Nigeria. African Journal of primary Healt Care & Family Medicine 1(1): 22-23.
-
Ugwu NI (2016) Pre-marital screening for sickle cell haemoglobin and genetic counseling: awareness and acceptability among undergraduate students of a Nigerian University. Int J Med Biomed Res 5(1): 43-49.
-
Madubuegwu EC, Onyia VO, Obiorah CB, Onah GN, Ibekaku UN (2021) Education of Rural Women for National Development: Exploring the Imperatives of Gender-Responsive Governance. International Journal of Academic and Applied Research 5(6): 53-62.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies