Abnormal Chromosome in Patients with Multiple Myeloma: A Cohor Study in Vietnam
Objective: To identify some common chromosomal mutation in patients with Multiple myeloma (MM) at Bach Mai hospital, from June 2016 to June 2021. Methods: We reviewed the cytogenetic results from 363 patients who were diagnosed with MM by IMWG diagnostic criteria 2014 at Bach Mai hospital. Results: Chromosomal abnormalities were detected in 35,3% (128/363) of the patients. Among these results, 128 cases (82,8%) had both numerical and structural chromosome abnormalities. Hyperdiploidy with structural cytogenetic aberrations was the most common finding (42,19%), followed by hypodiploidy with structural aberrations (23,44%). Amplification of the long arm of chromosome 1, loss 13/ del(13q) and abnormality involving 14q32 were the most frequent abnormalities which were observed in 39,84%, 24,2% and 21,9%. The most common numerical abnormalities were gains of chromosomes 9 with 28,57%.
Introduction
Multiple myeloma (MM) is a malignancy of the hematopoietic system caused by the monoclonal proliferation of plasmoblasts (plasma cells) in the bone marrow. The disease is characterized by complex genetic alterations at the cellular and molecular levels. Advances in Genetics in recent years have provided a better understanding of the pathogenesis and also provided the rationale for risk classification in MM [1, 2].
Currently, at the Center for Hematology and Blood
Transfusion, Bach Mai Hospital, bone marrow culture techniques to analyze marrow chromosomal formula and fluorescence in situ hybridization (FISH) techniques to identify gene mutations is a routine test for MM patients. There have been a number of authors studying chromosomal changes as well as gene mutations in this group of patients, but the sample size of these studies is still low and the abnormalities are detected (especially chromosomal mutations) limited.
In order to contribute to a deeper understanding of some common chromosomal mutations in MM, we conducted a study with the objective: “Abnormal chromosome in Vietnamese patients with multiple myeloma”.
Research Subjects and Methods
Research Subjects
Study subjects: 363 patients with confirmed diagnosis of MM came for examination and treatment at Bach Mai hospital from June 2016 to June 2021.
Patient selection criteria: The patient met the criteria for diagnosis of MM according to IMWG 2014 [3] at the Hematology and Blood Transfusion Center, Bach Mai Hospital from June 2016 to June 2021 and agreed to participate in the study.
Research Methods
Research period: From June 2016 to June 2021.
Research design: Retrospective, cross-sectional descriptive study. Sampling method: Convenience sampling.
Methods of data collection: Collecting results Analysis of the chromosomal formula of RA patients examined and treated at Bach Mai hospital.
Research Results
Bone marrow culture results
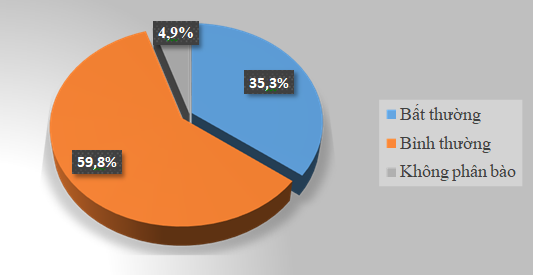
Comment: Figure 1 shows that after culturing 363 bone marrow samples, 128 samples (35.3%) were obtained with abnormal chromosomal formula results, 217 samples gave • Types of Chromosome Mutations Obtained normal chromosomal formula results (accounting for 59.8). %). There were 4.9% (18 samples) non- mitotic cultures.
| Mutant form | N | % |
|---|---|---|
| Only numerical chromosome mutations | 13 | 10,16 |
| Multiplier | 7 | 5,47 |
| Minority | 6 | 4,69 |
| Only structural chromosome mutations | 9 | 7,03 |
| Both numerical and structural chromosome mutations | 106 | 8281 |
| Almost tetraploid (81-103) | 3 | 2,34 |
| Almost triploid(58-80) | 11 | 8,59 |
| Multiplier (47-57) | 54 | 42,19 |
| Minority(39-45) | 30 | 23,44 |
| Diploid / Pseudo-diploid | 8 | 6,25 |
| TỔNG SỐ BỆNH NHÂN CÓ ĐỘT BIẾN | 128 | 100% |
Table 1: Types of chromosomal mutations obtained.
Comment: Among 128 cases with changes in chromosomal formula, the mutant form combining both quantity and structure accounted for the highest rate (82.81%) (Table 1). • Frequency of some common types of mutations in NTDs
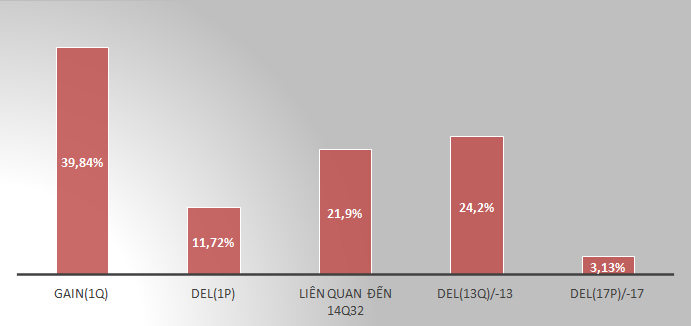
Comment: The frequency of gain(1q) mutations was 39.84%, followed by del(13q)/-13 mutations (24.2%) and mutations related to the IGH gene region (14q32). The lowest is the frequency of mutations del(17p)/-17 (3.13%) (Figure 2). • Frequency of quantitative mutations of each chromosome in DM
Comment
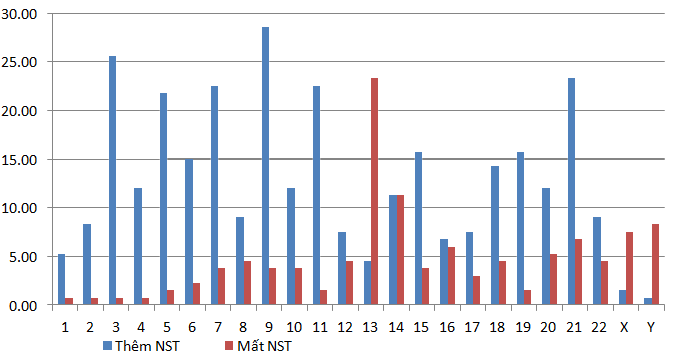
For extra chromosome mutations (Trisomy or Tetrasomy): The most frequently added chromosomes are 9 (28.57%), 3(25.56%), extra chromosomes 21,7,11, 5 have the same frequency (23.31%; 22.56%; 22.56%; 21.8%), respectively. The frequency of adding a Y chromosome is the lowest among the chromosomes (0.75%) (Figure 3).
For mutations that lose chromosomes (Monosomy): Loss of chromosome 13 has the highest frequency (23.31%), followed by loss of chromosome 14 (11.28%). The remaining chromosomes all have monosomy frequency less than 10%.
• Structural Mutation Frequency of Each Chromosome in Diabetes
60
| 13.53 9.02 9.77 9.77 6.77 4.51 2.26 | |||||||||||||||||||
| 6.77 | 2.26 | 4.51 | 6.02 |
Table 2: 1) similar to the research results of Shuhua Li and Hyeon -Ho Lim [7] also has 80% mutations in both structure and numbe
Comment: Structural mutations of chromosome 1 occur with the highest frequency (48.87%), the second highest are structural mutations of chromosome 14 (21.9%), then chromosome 11 with mutation frequency structure is 17.29% (Figure 4).
Discussion
Bone Marrow Culture Results
The advantage of the chromosomal formula analysis method is that it is possible to observe the totality of all chromosomes in the mitotic cluster, in addition to specific mutations, but also to analyze many other genetic lesions. According to Figure 1, out of 363 patients with MM who received bone marrow fluid culture to analyze chromosomal formula, there were 220 patients with normal chromosome results, 18 non- mitotic cultures (accounting for 4.9%). 35.3% of culture samples showed abnormal results when analyzed (128 samples).
Genetic variation of patients with MM is an important factor in disease prognosis. Chromosomal abnormalities are found in 30-50% of GERD cases [1, 4]. Our research results show that the rate of chromosomal mutations is in the above range, higher than the rate of 12% in the study of TLP Nguyen [5] and equivalent to the result of 33.2% of the author Maria. J. Calasanz and Juan C Cigudosa [6]. Also in this study, the author had 19 failed cultures (6.8%) [6], higher than our rate of 4.9%.
Types of Chromosomal Formula Mutations Obtained
When analyzing specifically 128 samples with changes in chromosomal formula, we found that more than 80% of samples carried both mutations in chromosomal number and structure (table 3.1) similar to the research results of Shuhua Li and Hyeon -Ho Lim [7] also has 80% mutations in both structure and number of chromosomes.
Author Anwar N. Mohamed, et al. [8] also showed that 77/120 cases (accounting for 64.2%) of chromosomal abnormalities in MM are multiple mutations (including polyploid mutations). Similarly, multiple mutations also accounted for 54% in the study of Shuhua Li, Hyeon-Ho Lim [7]. The rate of this type of mutation in our study is 58.6%, equivalent to the above authors.
The aneuploidy mutation (≤ 45chromosome) in MM is in the group of poor prognosis (excluding Y chromosome loss) [9], this type of mutation in our study was found in 36/128 patients, accounting for 28,13 %, similar to the rate of 28% that authors Shuhua Li, Hyeon-Ho Lim [7] gave, as well as the rate of 22% in the study of CS Debes-Marun [10] and higher than 14% according to the research of Maria J. Calasanz and Juan C. Cigudosa [6].
Pseudo-diploid mutation is a type of mutation where the chromosome cluster has 46 chromosomes, but there is still the phenomenon of adding or losing chromosomes in the patient’s chromosome set. This type of mutation accounts for a very low rate in our study (6.25%), equivalent to the result of 4% in the study of the authors Shuhua Li, Hyeon-Ho Lim [7], and much lower much higher than that of the author Maria J. Calasanz, Juan C.Cigudosa (29/72) [6] as well as the author Anwar N.Mohamed (13/120) [8].
Mutations with only multiples (47-57 chromosomes) (excluding structural mutations) belong to the standard prognostic group according to the risk classification in MM [2]. Our study results showed that 10.1% of patients belonged to this group of mutations, much lower than the rate of 36% in the study of CS Debes-Marun and GW Dewald [10] and higher than the rate of 6. % in the study of Shuhua Li and Hyeon-Ho Lim [7].
Differences in the rates of mutation types between studies may be due to differences in time, sample size, or because the study subjects were geographically distributed in different regions.
Frequency of Some Common Types of Mutations in MM
Amplification of 1q has been identified as a common mutation in MM genetic studies and is associated with poor prognosis in most studies. The mechanism of amplification of the q12-q23 region involves the break-fusion-connection (BFB, Breakage-Fusion-Bridge) cycles of 1q12 with bands on the long arm of chromosome 1, resulting in repeats Continuity of the q12-q23 region on chromosome 1, along with the amplification of a large number of genes in the range of 10-15 Megabases spread in the region 1q12-q23. 1q12 repeats facilitate the subsequent transformation of this amplicon region to other chromosomes [1].
Among our studies, the frequency gain(1q) reached 39.84%, the frequency del(1p) was 11.72% (Figure 3.2). This result is not much different from the study of Shuhua Li and Hyeon-Ho Lim [7] with the frequency gain(1q) and del(1p) being 50%, and 6%, respectively.
The authors McKenna RW and Kyle RA, et al. [2] suggested that the IgH gene region-related translocations on chromosome 14q32 are present in 55-70% of MM patients. In this study, we noted that changes related to the 14q32 region had a frequency of 21.9% (table 3.2), similar to the frequency of 23% of Calasanz, et al. [6], not significantly lower. Compared with the 36% frequency reported by the study of Shuhua Li and Hyeon-Ho Lim [7].
According to Anwar N Mohamed, et al. [8], 52% of cases of chromosomal metamorphosis have a mutation that either loses the long arm of chromosome 13 or loses both chromosome 13 (monosomy 13). Our study recorded a lower frequency of 24.2%, which is also lower than the 40% of Shuhua Li and Hyeon-Ho Lim [7].
Frequency of Mutations in the Number of Individual Chromosomes in Dmm
Multiplicative mutations are found in 50-60% of patients with changes in chromosomal formula, characterized by the addition of odd-numbered chromosomes such as 3,5,7,9,11,15,19 [1]. Our study also showed that the additive rate occurs mainly in odd chromosomes, in which trisomy (or tetrasomy) 9 has the highest frequency (28.57%), other chromosomes such as 3,5,7 ,11,21 has a frequency in the range of 21-25% (Figure 3). Authors Shuhua Li and Hyeon-Ho Lim [7] also gave the research results with the highest frequency of adding chromosomes +9, followed by chromosomes 15,19,5,7,3 (in descending order) on mutation frequency). Studying on 120 cases of MM with abnormal chromosomal formula, Anwar Mohamed, et al. [8] also concluded that the rate of the multiplicative mutation group usually has a higher frequency of addition than that of chromosome number 3,5, 7, 9, 11, 15, 19, 21. Thus, the results of the frequency of adding chromosomes in this study are similar to those of the above two authors.
Figure 3.3 shows that the frequency of monosomy is lower than the frequency of trisomy/tetrasomy in most chromosomes. In which -13 was the most common with 31, 18 cases (23.31%), followed by -14 (11.28%), -16 (6.02%). Also in the study of Shuhua Li and Hyeon-Ho Lim [7], the author showed that the most common deletion mutation is the loss of 13 chromosome (37/100 patients), followed by the loss of X , 14, 16, 17 chromosomes. The results of our study are similar to that of Shuhua Li [7], but there is not much difference compared to the results of Anwar N. Mohamed [8], with the frequency of common monosomy of the loss of 13 (38%), 14 (19%), 8(25%) chromosomes. Frequency of Structural Mutations of Each Chromosome in MM Figure 3.4 shows the frequency of structural mutations of each chromosome that we recorded in this study. The results showed that structural mutations of chromosome 1 had the highest frequency (48.87%), including gain(1q), del(1p), and translocations of chromosome 1 with other chromosomes. This was discussed in section 4.2.
Conclusion
- - 35.3% of MM patients have changes in chromosome formula:
- + 82.81% is a complex mutation with a poor prognosis, combining both the number and structure of chromosomes.
- + The highest frequency of gain(1q) mutations reached 39.84%, followed by del(13q)/-13 mutations (24.2%) and 21.9% were mutations related to the IGH gene region. (14q32). The frequency of mutations del(17p)/-17 was the lowest (3.13%).
- + Trisomy/tetrasomy mutations mainly occur in odd chromosomes, with the highest frequency + 9 (28.57%), then on chromosomes +3, +21, +5, +7, + 11, +19.
- + Most of the monosomy mutations of each chromosome occur with a frequency of less than 10%, the highest frequency is -13 (23.31%), -14 (11.28%).
- + The frequency of structural mutations of chromosome 1 was highest, reaching (48.87%), chromosome 14 was 21.9%, chromosome 11 was 17.29%, the remaining structural chromosomes mutations had less than 15%.
References
-
Sawyer JR (2011) The prognostic significance of cytogenetics and molecular profiling in multiple myeloma”, Cancer Genet 204(1): 3-12.
-
McKenna RW, Kyle RA, Kuehl WM, Harris NL, Coupland RW, et al. (2017) Plasma cell neoplasms, WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, pp: 241-249.
-
Rajkuma SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, et al. (2014) International Myeloma Working Group update criteria for the diagnosis of multiple myeloma. Lancet Oncol 15(12): e538-548.
-
Viguié F (2004) Multiple myeloma. Atlas Genet Cytogenet Oncol Haematol 8: 255-257.
-
Nguyen TLP (2012) Study on stage characteristics according to the ISS international staging system in Multiple myeloma at the National Institute of Hematology and Blood Transfusion. Thesis of Master of Medicine, Hanoi Medical university, Vietnam.
-
Calasanz MJ, Cigudosa JC, Odero MD, Ferreira C, Ardanaz MT, et al. (1997) “Cytogenetic Analysis of 280 Patients With Multiple Myeloma and Related Disorders: Primary Breakpoints and Clinical Correlations. Genes, Chromosomes & cancer 18(2): 84-93.
-
Li S, Lim HH, Woo KS, Kim SH, Han JY (2016) A retrospective analysis of cytogenetic alterations in patients with newly diagnosed multiple myeloma: a single center study in Korea. Blood Res 51(2): 122-126.
-
Mohamed AN, Bentley G, Bonnett ML, Zonder J, Al-Katib A (2007) Chromosome aberrations in a series of 120 multiple myeloma cases with abnormal karyotypes”, American Journal of Hematology 82(12): 1080-1087.
-
Kazmi SM, Nusrat M, Gunaydin H, Cornelison AM, Shah N, et al. (2015) Outcomes Among High-Risk and Standard- Risk Multiple Myeloma Patients Treated with High-Dose Chemotherapy and Autologous Hematopoietic Stem Cell Transplantation. Clin Lymphoma Myeloma Leuk 15(11): 687-693.
-
Debes Marun CS, Dewald GW, Bryant S, Picken E, Santana- Da´vila R, et al. (2003) Chromosome abnormalities clustering and its implications for pathogenesis and prognosis in myeloma. Leukemia 17(2): 427-436.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies