Complications and Associations in a Multiple Myeloma Cohort at Presentation
Background: Myelomatosis accounts for about 10% of haematological malignancies according to previous studies in different climes. The impact of some complications on treatment choice as well as survival outcomes is significant and worthy of study. Aims: To describe complications observed at presentation in this cohort of myeloma patients and to assess the associations of these complications with certain laboratory and clinical parameters. Results: There were 37 males and 29 females, median age 61 years (Range 37-85). Median values at presentation was Hb - 8g/dL, serum albumin 37 mg/dL and calcium 2.5 mmol/L. Bence Jones proteinuria was present in 50% (17/34), majority (78.8% -26/33) had IgG myeloma and 7 (21.2%) IgA. They had nephropathy 19% (4/21), osteolytic lesions 34.7% (17/49), pathological fractures 56.1% (23/41), anaemia 91.4% (53/58) and hypercalcaemia 42% (21/50). commonest presenting symptom was bone pain in 87.2% (48/55). There was significant correlation between hypercalcaemia and haematocrit (r=0.338, p=0.039) and platelet count (r= 0.331, p= 0.029). No relationship was found between hypercalcaemia and beta -2 microglobulin (r= 0.046, p= 0.0834) or serum immunoglobulin (r= -0.071, p= 0.745). Pathological fractures showed no significant association with haematocrit (r= -0.137, p= 0.453), platelet (r= -0.097, p= 0.642), beta -2 microglobulin (r= -0.037, p= 0.865) and serum immunoglobulin (r= -0.132, p= 0.545). Chi square value for the occurrence of renal Impairment and hypercalcaemia was found to be significant r= 8.048, p= 0.007 as well as pathological fractures (r=8.048, p=0.005). Conclusions: Myeloma is prevalent in males 1.5:1. Bone pain and anaemia are the commonest features at presentation. Bence Jones proteinuria is only seen in about half of the patients and lytic lesions in about a third. Pathological fractures, anaemia or hypercalcaemia at presentation, were not associated with tumor stage (β-2 microglobulin and albumin levels). Significant association exists between the occurrence of renal impairment and pathological fractures.
Introduction
Myelomatosis is a bone marrow malignancy consisting of clonal proliferation of plasma cells. This malignancy has been noted by previous researchers to be more prevalent among the Black population and in the older age group [1, 2, 3]. A clinical feature at presentation is used to define symptomatic disease as well as commencement of therapy. The occurrence of the complications of the disease, mainly due to marrow invasion and tumor secretion of cytokines, leads to hypercalcaemia, renal complications, anaemia, bone disease and infections – CRABI [4].
The impact of the presence of some of these complications as well as the frequency of these features may vary across patient groups and this may be due to environmental variations as well as differences in tumor genetics [5, 6]. The most common presenting feature of multiple myeloma is bone pain, observed in 84 - 96% of patients and pathological fractures in 44%. Nephropathy may occur due to myeloma protein deposition, hypercalcaemia, anaemia, infection or chemotherapy and has been noted to occur in 23 - 33% of patients at presentation [7, 8]. The presence of these complications adversely affect disease outcome and may add to mortality attributed to myeloma [9, 10, 11].
The occurrence of these complications at presentation may either be an indirect effect of tumor burden or a direct effect of tumor genetics with consequent aggressiveness. It has been known that the presence of some mutations - like the t(4,14) or other translocations involving the immunoglobin lambda locus [12, 13], renders myeloma clones resistant to several chemotherapeutic agents and may confer poorer prognosis [14]. An attempt to assess the association of some known makers of tumour burden with the occurrence of some of these common complications of myeloma would help to discern if a direct relationship exists between them.
Patients and Methods
The clinical data was collected prospectively from 66 patients with bone marrow confirmed diagnosis of multiple myeloma at the Haeme-Oncology Clinic and wards of the University of Nigeria Teaching Enugu. Data collected included patients demographic data, laboratory results (haematocrit, serum calcium, immunoglobulin, -2 microglobulin and Bence Jones protein) and radiographs. Ethical approval was obtained from the University of Nigeria Teaching Hospital, Health Research and ethical review board.
Statistical Analysis
Data analysis was done using IBM SPSS 20.0 Chicago Illinois. Median values and proportions were used to represent discrete and categorical variables respectively. The Pearsons correlation coefficient and Independent Sample T test was done to assess the relationship between discrete variables while Fischers Exact test was used for categorical variables. All statistical analysis was 2 tailed without assuming equal variance, with bootstrapping to take care of outliers. Significance was assumed for all p values 0.05.
Results
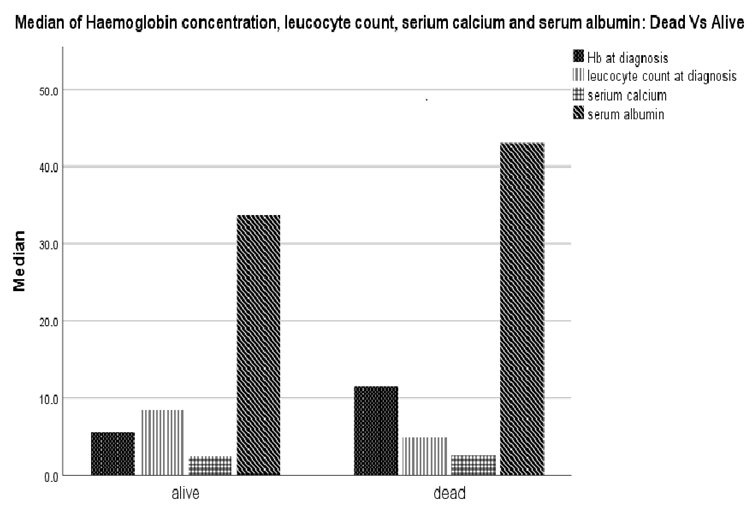
There 66 adults - 37 males (56.1%) and 29 (43.9%) females, giving a male: female prevalence ratio of 1.5:1. Their ages ranged from 37 to 85 years, with a median age of 61 years. The median haemogram values at presentation were Haemoglobin concentration (Hb) - 8g/dL, packed cell volume (PCV) - 0.216 L/L, leucocyte count - 6.1 x 109/L, platelet count - 198 x 109/L, serum albumin 37 g/dL and calcium 2.5 mmol/L. Bence Jones proteinuria was observed to be positive in 50% (17/34) of the patients, median -2 microglobulin levels of 5.2 mg/L while majority (78.8% -26/33) had IgG myeloma and only 7 (21.2%) were IgA, none of the patients had IgM myeloma. Figure 1 shows the median values of the serum albumin, calcium, white cell count and haemoglobin concentration at presentation in those patients that had dies compared to the living.
The complications observed were; nephropathy 19% (4/21), osteolytic lesions 34.7% (17/49), pathological fractures 56.1% (23/41), anaemia 91.4% (53/58) and hypercalcaemia 42% (21/50). The most common presenting symptoms was bone pain in 87.2% (48/55) at diagnosis. There was a significant correlation between hypercalcaemia and haematocrit (r=0.338, p=0.039); and platelet count (r= 0.331, p= 0.029). While no relationship was found between hypercalcaemia and -2 microglobulin (r= 0.046, p= 0.0834) or serum immunoglobulin (r= -0.071, p= 0.745).
Prevalence of pathological fractures at presentation was 56.1%% (23/41), in 12 males and 11 females. This was found to show no significant association with haematocrit (r= -0.137, p= 0.453), platelet (r= -0.097, p= 0.642), -2 microglobulin (z= -0.170, p= 0.913), serum albumin (z= -0.548, p= 0.648) as well as serum immunoglobulin (z= -0.605, p= 0.611).
Nephropathy at presentation was observed in 19% (4/21), more in males - 75% with a median age of 62.5 years in the affected population. Bence Jones proteinuria was not observed in any of the patients who had renal impairment on presentation. The patients in this group also had a lower median Hb of 6.5g/dL at presentation. Table 1 only one of the patients who had hypercalcaemia on presentation also had nephropathy, while 4 of them presented with symptomatic anemia.
Anaemia was observed at presentation in 91% (53/58) of patients, 30 males and 23 females. Only 13 of the patients had anaemia and hypercalcaemia while only 1 of the 4 patients with nephropathy also had anaemia at presentation. Presence of anaemia was not significantly associated with serum -2 microglobulin (z= -1.324, p= 0.203), albumin (z= -1.005, p= 0.374) as well as immunoglobulin (z= -0.605, p= 0.611).
The prevalence of hypercalcaemia was observed in 55.2% (16/29) of the patients - 10 males and 11 females.
This was significantly associated with PCV (z= -2.059, p= 0.041) and platelet count (z= -2.183, p= 0.029) but showed no significant association with -2 microglobulin (z= -0.210, p= 0.856), serum albumin (z= -0.561, p= 0.615) and immunoglobulin (z= -0.326, p= 0.772). The Chi square value for the occurrence of renal Impairment and hypercalcaemia was found to be significant r= 8.048, p= 0.007. This was also similar to the association with pathological fractures (r=8.048, p=0.005). Median values and proportions in patients who presented with nephropathy and pathological fractures are shown in Table 1.
| Parameters | All Patients | Pathological Fracture | Bone pain | Nephropathy | Anaemia | Hypercalcaemia |
|---|---|---|---|---|---|---|
| Sex (male/female) | 37/29 | 11-Dec | 25/23 | 1-Mar | 30/23 | 11-Oct |
| Age | 61 | 61 | 59.5 | 62.5 | 60 | 62 |
| Haemoglobin concentration | 8 | 8 | 7.8 | 6.4 | 7.9 | 7.2 |
| Packed cell volume | 21.6 | 23.5 | 21.3 | 28 | 21 | 20 |
| Bence Jones proteinuria (negative/positive) | 17/17 | 9-Apr | 15/13 | Mar-00 | 16/13 | 4-Jul |
| Serum β 2 microglobulin | 5.2 | 5.4 | 5 | NA | 5.2 | 5 |
| Serum albumin | 37 | 36 | 36 | NA | 31.5 | 32.5 |
| Serum calcium | 2.5 | 2.4 | 2.5 | 2.45 | 2.5 | 2.5 |
Table 1: Median values and proportions in myeloma patients with the common disease complications.
Discussion
Multiple myeloma (MM) is a plasma cell malignancy occurring with varying frequency across various populations [15]. The male: female ratios had been noted in some populations to be similar though in our cohort males were one and a half times more at risk of MM than females. Whether this can be explained by exposure to noxious agents peculiar to some occupations is yet to be proven. The median age of the cohort was found to be 61 years, this is closer to the median age of other myeloma cohorts of 65 years, though previous studies in Africa had proposed younger age incidence [7, 8]. At presentation majority of the patients were anaemic, had bone pains and pathological fracture while only a few had nephropathy. This had been reported by previous researchers [10, 16] though the factors (environmental and genetic) which contribute to the early occurrence of these complications are yet to be fully delineated. Anaemia in this cohort was found in majority though other cytopaenias were not common. This points to the fact that anaemia in MM is most likely not secondary to marrow invasion. Other mechanisms including immune haemolysis, nutritional deficiencies, effect of infections and chemotherapy, reduced erythropoetin levels and action of tumor-associated cytokines on haematopoiesis may all contribute to some extent.
The presence of pathological fractures and anaemia was observed as the predominant presenting feature. This suggests that fractures may be an indirect presentation of marrow invasion leading to anaemia and increasing bone fragility. However, fractures were not found to be more in people with lower haematocrit or platelet count in this group. This may imply that occurrence of this complication is most likely multi-factorial and is not clearly the direct impact of tumour burden. The occurrence of pathological fractures negatively impacts on the morbidity and survival in myeloma patients [10, 16]. There was no association between the occurrence of fractures and a low serum albumin, high serum immunoglobulin or 2 microglobulin levels, all notable indicators of disease severity and tumor bulk. This may be an indication that the occurrence of pathological fractures may be due to inherent genetic or environment factors peculiar to each patient as well as an interplay between the underlying cancer and the osteogenetic factors. In other words, this may be a complication that is unrelated with disease progression or tumor stage.
Renal impairment in multiple myeloma occurs as a result of several factors, ranging from; anaemia secondary to marrow invasion, hypercalcaemia, infections, chemotherapy or effect of myeloma kidney with its associated protein deposition. This was found in less than a quarter of the patients and did not show a significant association with the occurrence of BJP. This may be explained by the degree of loss of tubular function [17] that might occurred at the point of obvious clinical signs of renal impairment which my preclude excretion of this urinary marker. Also the degree of secretion of dysfunctional immunoglobulin chains varies across various myeloma subtypes and may not be easily detectable [18].
Anaemia is a common consequence of many haematological malignancy with marrow invasion. The causes of anaemia in MM has been observed in previous studies to be due to; nephropathy, marrow overcrowding, effect of tumor-associated cytokines and immune mediated haemolysis. The extent to which each of this factors contribute to the anaemia on presentation will depend tumor burden as well as the other genetic and environmental factors [6]. The presence of anaemia was not related to serum levels of albumin or -2 microglobulin and this further explains why anaemia though a disease defining parameter does not significantly impact on the disease stage [19].
Bence Jones proteinuria (BJP) was found is half of the patients in this cohort. The observation of a low BJP positivity had been reported by previous researchers and this further supports the fact that this test is not a reliable screening test for MM [20, 21] . Majority of myeloma cases in most patient populations are of IgG type, this was the case in this cohort though a higher proportion than expected were IgA. This may explain the lower survival rates observed by previous researchers in MM in Africa as IgA myeloma is known to have a poorer prognosis. The most frequent feature of MM at diagnosis was anaemia, followed by bone pain, pathological fracture and hypercalcaemia, consecutively. Bone pain had been reported in previous studies as the most common presentation however we discovered that sub-clinical anaemia may be present though unrecognized at this time [7, 21]. There is need for vigilance as persistent anaemia may worsen or initiate renal impairment in this group of patients already at risk of nephropathy due to deposition of myeloma proteins.
Hypercalcaemia in MM is a consequence of the overall osteoclastic\bone resorptive effect of the malignant plasma cells. This was observed to have a significant association with haematocrit and platelet count but not the serum -2 microglobulin or albumin, both indicators of disease stage. The serum calcium level is used to diagnose symptomatic disease though not directly indicative of disease stage, as was shown by the findings of this study.
It is instructive to note that neither the serum calcium, occurrence of pathological fractures, nephropathy or anaemia were associated with serum levels of albumin or -2 microglobulin, currently being used for staging of myeloma.
Conclusion
Myelomatosis commonly presents as anaemia and bone pain in individuals with a median age of 61 years. The most prevalent CRAB symptom observed in this cohort was anaemia. The serum -2 microglobulin and albumin levels were not significantly associated with the presence of CRAB features at presentation.
Declarations: Authors declare no conflict of interest in writing this manuscript.
References
-
Baughn LB, Pearce K, Larson D, Polley MY, Elhaik E, et al. (2018) Differences in genomic abnormalities among African individuals with monoclonal gammopathies using calculated ancestry. Blood Cancer J 8(10): 1-10.
-
Smith CJ, Ambs S, Landgren O (2018) Biological determinants of health disparities in multiple myeloma. Blood Cancer J 8(9): 1-7.
-
Waxman AJ, Mink PJ, Devesa SS, Anderson WF, Weiss BM, et al. (2010) Racial disparities in incidence and outcome in multiple myeloma: a population-based study. Blood 116(25): 5501-5506.
-
Dispenzieri A, Rajkumar SV, Gertz MA, Fonseca R, Lacy MQ, et al. (2007) Treatment of newly diagnosed multiple myeloma based on Mayo Stratification of Myeloma and Risk-adapted Therapy (mSMART): consensus statement. Mayo Clin Proc 82(3): 323-341.
-
Chng WJ, Kumar S, VanWier S, Ahmann G, Troska TP, et al. (2007) Molecular Dissection of Hyperdiploid Multiple Myeloma by Gene Expression Profiling. Cancer Res 67(7): 2982-2989.
-
Corre J, Munshi N, Avet-Loiseau H (2015) Genetics of multiple myeloma: another heterogeneity level? Blood 125(12): 1870-1876.
-
Acquah ME, Hsing AW, McGuire V, Wang S, Birmann B, et al. (2019) Presentation and survival of multiple myeloma patients in Ghana: a review of 169 cases. Ghana Med J 53(1): 52-58.
-
Nwabuko OC, Igbigbi EE, Chukwuonye II, Nnoli MA (2017) Multiple myeloma in Niger Delta, Nigeria: complications and the outcome of palliative interventions. Cancer Manag Res 9: 189-196.
-
Kazandjian D (2016) Multiple myeloma epidemiology and survival, a unique malignancy. Semin Oncol 43(6): 676-681.
-
Thorsteinsdottir S, Gislason G, Aspelund T, Sverrisdottir I, Landgren O, et al. (2020) Fractures and survival in multiple myeloma: results from a population-based study. Haematologica 105(4): 1067-1073.
-
Webster AC, Irish AB, Kelly PJ (2018) Changing survival of people with myeloma and end stage kidney disease: A cohort study using Australian and New Zealand dialysis and transplant registry 1963-2013. Nephrol Carlton Vic 23(3): 217-225.
-
Leich E, Weißbach S, Klein HU, Grieb T, Pischimarov J, et al. (2013) Multiple myeloma is affected by multiple and heterogeneous somatic mutations in adhesion- and receptor tyrosine kinase signaling molecules. Blood Cancer J 3(2): e102-e102.
-
Chang H, Sloan S, Li D, Zhuang L, Yi QL, et al. (2004) The t(4;14) is associated with poor prognosis in myeloma patients undergoing autologous stem cell transplant. Br J Haematol 125(1): 64-68.
-
Barwick BG, Neri P, Bahlis NJ, Nooka AK, Dhodapkar MV, et al. (2019) Multiple myeloma immunoglobulin lambda translocations portend poor prognosis. Nat Commun 10(1): 1911.
-
Altieri A, Chen B, Bermejo JL, Castro F, Hemminki K (2006) Familial risks and temporal incidence trends of multiple myeloma. Eur J Cancer 42(11): 1661-1670.
-
Sonmez M, Akagun T, Topbas M, Cobanoglu U, Sonmez B, et al. (2008) Effect of pathologic fractures on survival in multiple myeloma patients: a case control study. J. Exp. Clin. Cancer Res 27(1): 11.
-
Heher EC, Rennke HG, Laubach JP, Richardson PG (2013) Kidney Disease and Multiple Myeloma. Clin J Am Soc Nephrol CJASN 8(11): 2007-2017.
-
Hayes C, Shafi H, Mason H, Klapper E (2016) Successful reduction of plasma free-hemoglobin using therapeutic plasma exchange: A case report. Transfus Apher Sci 54(2): 253-255.
-
Greipp PR, San Miguel J, Durie BGM, Crowley JJ, Barlogie B, et al. (2005) International staging system for multiple myeloma. J Clin Oncol Off 23(15): 3412-3420.
-
Nnonyelum ON, Anazoeze MJ, Eunice NO, Emmanuel OO, Stella AT, et al. (2015) Multiple myeloma in Nigeria: a multi-centre epidemiological and biomedical study. Pan Afr Med J 22: 292.
-
Madu AJ, Ocheni S, Nwagha TA, Ibegbulam OG, Anike US (2014) Multiple myeloma in Nigeria: an insight to the clinical, laboratory features, and outcomes. Niger J Clin Pract 17(2): 212-217.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies