The Melded Conglomerate-Composite Hemangioendothelioma
Composite hemangioendothelioma is an infrequent vascular neoplasm characteristically comprised of complex intermingling of benign, low grade malignant and malignant vascular components and intermediate biological behaviour. Preponderantly confined to distal extremities, especially hands and feet, neoplasm commonly implicates the adult population. The inadequately circumscribed lesion is confined to deep seated dermis or subcutaneous tissue and represents with an admixture of vascular lesions as epithelioid hemangioendothelioma, retiform hemangioendothelioma, low grade angiosarcoma, lymphangioma or variants of haemangioma as spindle cell haemangioma, capillary haemangioma, cavernous haemangioma, hobnail haemangioma or epithelioid haemangiom.
Introduction
Composite hemangioendothelioma emerges as an exceptionally discerned vascular neoplasm associated with intermediate biological behaviour. Characteristically, tumefaction is comprised of complex intermingling of benign, low grade malignant and malignant vascular components. The uncommon vascular neoplasm of intermediate malignant potential is exceptionally accompanied by regional lymph node and distant metastasis. Upon low power examination, tumefaction demonstrates significant morphologic variation. Segregation of composite hemangioendothelioma from various vascular neoplasms may be challenging although the neoplasm exhibits significantly variable vascular histological configurations within a singular lesion. Tumefaction may arise as a congenital lesion, within infancy, paediatric subjects or adolescents. However, adults are predominantly implicated and neoplasm may be observed in up to eighth decade [1, 2].
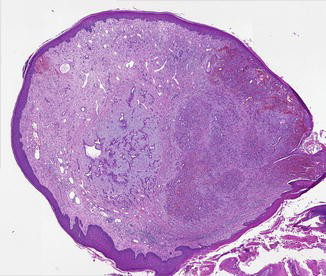
Majority of lesions are situated upon distal extremities, especially hands and feet. Additionally, sites such as head and neck, dorsal region, mediastinum, bone, inguinal lymph nodes, renal parenchyma or spleen may be implicated [1, 2]. Of obscure aetiology, individuals delineating composite hemangioendothelioma may exhibit history of lymphedema. Tumefaction may concur with Kasabach-Merritt or Maffucci’s syndrome. Clinically, lesions of extended duration appear multinodular and demonstrate a reddish blue hue [1, 2]. Grossly, composite hemangioendothelioma manifests as a nodular tumefaction of bluish, purple or reddish blue hue. Multiple nodules may be discerned. Tumefaction appears to infiltrate circumscribing soft tissue [2, 3].
Upon microscopy, an inadequately circumscribed lesion appears to be confined to deep seated dermis or subcutaneous tissue. Tumefaction may infiltrate into encompassing soft tissue [2, 3]. Upon low power examination, morphological features appear to vary between diverse tumour zones [3, 4].
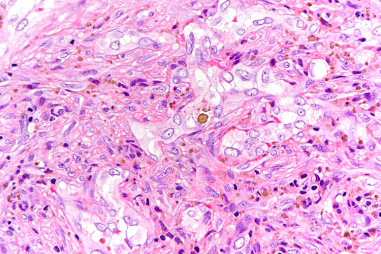
Neoplasm demonstrates admixture of divergent vascular components and may represent commingling of epithelioid hemangioendothelioma, retiform hemangioendothelioma, low grade angiosarcoma, lymphangioma or variants of haemangioma as spindle cell haemangioma, capillary haemangioma, cavernous haemangioma, hobnail haemangioma or epithelioid haemangioma [3, 4]. Aforesaid diverse components appear intensely intermingled and segregation of various ‘pure’ vascular components may be challenging. Tumour cells appear as epithelioid endothelial cells and demonstrate vacuolated, pseudo-lipoblastic appearance. Mitotic activity is minimal [3, 4].
| Mitotic score | Mitosis/10 HPF | Mitosis / mm² |
|---|---|---|
| Score 1 | 0-9 mitosis/10 HPF | 0-5 mitosis/mm² |
| Score 2 | 10-19 mitosis/ HPF | 6-11 mitosis/mm² |
| Score 3 | >19 mitosis /10 HPF | >11 mitosis/mm² |
Table 1: ** Mitotic score of soft tissue sarcomas.
HPF: High Power Fields. Table 1: Mitotic score of soft tissue sarcomas.
Mitotic count is predominantly calculated from mitotically active areas, devoid of tumour necrosis. Mitosis may be quantified within 10 consecutive high power fields (HPF) upon 40x objective or 1 HPF x 400 = 0.1734 mm2 area wherein appropriate high power fields encompassing 1 mm2 area is contingent to individual microscope.
| Tumour Necrosis | |
|---|---|
| Score 0 | Absence of tumour necrosis |
| Score 1 | <50% tumour necrosis |
| Score 2 | ≥50% tumour necrosis |
Table 2: Tumour score associated with necrosis.
Tumour necrosis is appropriately evaluated upon cogent gross examination and categorized upon histological sections.
Tumour cells appear immune reactive to CD31, CD34, ERG, FLI1 or factor VIII. Tumour cells appear immune non- reactive to human herpes virus 8(HHV8) [5, 6].
Composite hemangioendothelioma requires segregation from neoplasms as retiform hemangioendothelioma, Dabska type hemangioendothelioma, Kaposiform hemangioendothelioma, epithelioid hemangioendothelioma, Kaposi’s sarcoma or angiosarcoma [5, 6]. Cogent histological evaluation is an optimal, recommended methodology for obtaining a definitive diagnosis. Appropriate tumour discernment upon examination of miniature tissue samples may be challenging on account of varied morphological spectrum expounded by the neoplasm [5, 6]. Optimal and recommended therapeutic guidelines remain obscure on account of infrequency of the neoplasm. However, surgical extermination of the neoplasm may be adopted with curative intent. Localized radiotherapy and chemotherapy may be employed for treating reoccurring and metastatic disease [5, 6].
Prognostic outcomes are contingent to localized tumour reoccurrence and tumour aggressiveness appearing in ~50% of neoplasms. Localized tumour reoccurrence may occur within 18 months to 10 years following initial surgical excision. Proportionate regional lymph node or distant metastasis is minimal. Tumour reoccurrence or distant metastasis may occur regardless of angiosarcoma- like foci discerned upon morphological evaluation [5, 6]. Irrespective of variable morphological spectrum expounded by the neoplasm, the biological behaviour remains identical. Precise tumour discernment is crucial for accurate therapy and ascertainment of prognostic outcomes [5, 6].
Conclusion
Tumour cells appear immune reactive to CD31, CD34, ERG, FLI1 or factor VIII and immune non- reactive to human herpes virus 8(HHV8). Composite hemangioendothelioma requires segregation from neoplasms as retiform hemangioendothelioma, Dabska type hemangioendothelioma, Kaposiform hemangioendothelioma, epithelioid hemangioendothelioma, Kaposi’s sarcoma or angiosarcoma. Cogent histological evaluation is an optimal, recommended methodology for obtaining a definitive diagnosis. Optimal, recommended therapeutic guidelines remain obscure on account of infrequency of the neoplasm. However, surgical extermination of the neoplasm may be adopted with curative intent.
References
-
Linos K, Dermawan JK, Pulitzer M, Abbas A, Cristina RA, et al. (2024) Untying the Gordian knot of composite hemangioendothelioma: Discovery of novel fusions. Genes Chromosomes Cancer 63(1): e.23198.
-
Deng Y, Li M (2023) Composite hemangioendothelioma- report of two cases located in bone and review of the literature. BMC Musculoskelet Disord 24(1): 676.
-
Huang W, Zhou Y, Yang Q, Liming L, Lei K (2023) Extraosseous Uptake and Multiple Metastases of Splenic Composite Hemangioendothelioma on 99m Tc-MDP Scintigraphy. Clin Nucl Med 48(12): 1107-1110.
-
Bui CM, Balzer B (2023) Multiply Recurrent Composite Hemangioendothelioma of Penis with Histologic Progression to High-Grade Features. Dermatopathology (Basel) 10(1): 41-45.
-
Schaeffer T, Glatz K, Eckstein FS, Matt P (2023) Composite haemangioendothelioma in the heart: a case report. Eur Heart J Case Rep 7(8): ytad343.
-
Balko J, Ozaniak A, Krskova L, Zuzana S, Robert L, et al. (2023) Patient with composite haemangioendothelioma containing angiosarcoma-like areas in the setting of congenital lymphoedema mimicking Stewart-Treves syndrome: a case report. Diagn Pathol 18(1): 76.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies