Factors Affecting Heparin Induced Thrombocytopenia: A Case Series Study
Heparin-induced thrombocytopenia (HIT) is a condition that can affect patients who are exposed to heparin across a variety of disease states. A case series study was conducted to evaluate the effect of patient age, unfractionated heparin dose and nadir platelet count on the 4T score in a multiple regression analysis. The number of cases selected was ten. The regression analysis showed that patient age and nadir platelet count were statistically significant (P<.05) and the R-squared value was 0.7. A Pearson correlation coefficient analysis also revealed a low positive correlation between heparin dose and platelet count (r = 0.3). These findings add to the body of knowledge encompassing unfractionated heparin which remains a widely used anticoagulant for patients with thrombotic disease and other conditions and procedures. Future studies should continue to evaluate factors that affect HIT including outcomes between Type I and Type II HIT.
Introduction
Heparin induced thrombocytopenia (HIT) can be described as a severe complication of exposure to heparin that is associated with a fall in platelet count and occurrences of thrombosis with venous thrombosis of lower limbs being the most common [1]. This condition was first reported in 1958 in which ten patient cases were described, all presenting with arterial embolism after receiving therapeutic doses of heparin; six of the ten patients died [2]. The prevalence of HIT is estimated to be approximately 20,000 cases per year in the United States; the mortality rate is 30 percentage [3, 4]. There are two forms of HIT. Type I is described as a non- immunologic response to heparin therapy, mediated by a direct interaction between heparin and circulating platelets causing platelet clumping or sequestration. Type I is self- limiting and affects approximately ten to thirty percent of patients and typically occurs within the first 48 to 72 hours after receiving heparin; the platelet count typically remains above 100,000/µL. In contrast, Type II HIT is immune- mediated occurring five to ten days after heparin therapy and is associated with platelet counts less than 100,000/µL or a decrease in platelet count less than fifty percent of baseline values [5]; antibodies form which target a complex of heparin and platelet factor 4 on the platelet membrane, triggering a positive feedback mechanism releasing additional PF4 from alpha granules within the platelet organelle zone.
Confirmation of HIT is procured by a PF4/heparin immunoassay and the 4T scoring system described by Warkentin TE, et al. [6]. The 4T scoring system is widely used in clinical practice and employs four criteria: 1) thrombocytopenia, 2) timing of platelet count fall, 3) thrombosis or other sequelae and 4) other causes of thrombocytopenia (Table 1). A score of 0 to 3 reflects low probability, 4 to 5 intermediate probability, and 6 to 8 high probability of HIT.
| 2 points | 1 point | 0 points | |
|---|---|---|---|
| Thrombocytopenia | >50% decrease, or nadir of 20,000-100,000/μL | 30-50% decrease, or nadir of 10,000-19,000/μL | 30% decrease or nadir <10,000/μL |
| Timing of Platelet Count Fall | 5-10 days, or ≤1 day if heparin exposure within past 30 days | >10 days or not certain or <1 day if heparin exposure within past 30-100 days | ≤4 days (no recent heparin) |
| Thrombosis or other sequelae | Thrombosis, skin necrosis, or after heparin bolus, acute systemic reaction | Progressive, recurrent, or silent thrombosis; erythematous skin lesions | |
| Other cause of thrombocytopenia | None evident | Possible | Definite |
Table 1: Scoring System for HIT.
HIT is most often associated with patients receiving unfractionated heparin (UFH). Unfractionated heparin has a molecular weight range between 3000 and 30,000 daltons [7] and is composed of a sulphated polysaccharide whose negative charge binds to the positively charged protein antithrombin. This ionic interaction leads to a conformational change of antithrombin and subsequent inhibition of thrombin and other coagulation proteins (IXa, Xa, XIa, XIIa) exerting an anticoagulation effect in patients being treated for thrombotic conditions or prophylaxis thereof. Low molecular weight heparin (LMWH), in contrast, has a molecular weight between 4000 and 5000 daltons with a predilection for inhibiting Factor Xa given its truncated structure [fewer than 18 saccharides] compared to UFH. LMWH also exhibits a lower ability to bind to platelets which explains the decreased incidence of HIT associated with LMWH drugs such as enoxaparin. A meta-analysis revealed that the risk of developing HIT in patients receiving LMWH is 0.2 percent, compared to 2.6 percent with UFH [8]. Another difference between LMWH and UFH is the clearance mechanism; in the former the drug is cleared via the renal system, in the latter the drug is cleared by the reticuloendothelial system through saturation of endothelial cells or monocytes, and the renal system. Both formulations can be used in treating patients with venous thromboembolism (VTE), acute coronary syndrome (ACS), atrial fibrillation, and pulmonary embolism (PE). Given the high mortality rate a case series multiple regression study was done to investigate factors that may affect the development of HIT. Factors included in the study and operationalized in the methods section are patient age, UFH dose, nadir platelet count, and the 4T score.
Methods
Case reports of HIT were identified using PubMed and included in the study if the article contained factors studied (4T score, patient age, UFH dose, and nadir platelet count). The nadir platelet count is defined as the lowest platelet count recorded after receiving UFH. Of fifteen case reports identified, ten were selected based in inclusion criteria (Table 2). The dependent variable was the 4T score; independent variables included nadir platelet count, UFH dose, and patient age. The multiple regression analysis was performed using SPSS (v29). All variables were classified as continuous or scale. Statistical significance was established at P<.05. The R-squared value and unstandardized predictive value were also computed.
| 4T Score | Nadir Platelet Count | UFH Dose (total units) | Patient Age/Gender/Condition | |
|---|---|---|---|---|
| Altamirano-Solorzano, GA 2021 | 6 | 25,000/μL | 50,400 | 48 Male COVID-19 |
| Karki S et al, 2023 | 7 | 26,000/μL | 1,60,000 | 66 Male DVT prophylaxis |
| Iwasaki et al, 2023 | 7 | 51,000/μL | 18,532 | 57 Male Hepatocellular carcinoma |
| Faucher, L et al, 2023 | 7 | 38,000/μL | 12,500 | 86 Male PE |
| Nikooghadam, SM et al, 2023 | 6 | 43,000/μL | 6500 | 36 Female Pregnancy |
| Jing Liu et al, 2019 | 5 | 20,000/μL | 5000 | 37 Male Gastric tumor |
| Tugulan C et al, 2021 | 8 | 66,000/μL | 64,000 | 65 Male Coronary Artery Disease |
| Shen L et al, 2022 | 5 | 84,000/μL | 11,000 | 74 Male Atrial Fibrillation |
| Phan et al, 2020 | 5 | 44,000/μL | 8000 | 43 Male COVID-19 |
| Ahmed M et al, 2019 | 7 | 82,000/μL | 60,000 | 39 Female Gun shot wound, colon resection |
Table 2: Case Reports included in multiple regression analysis.
Results
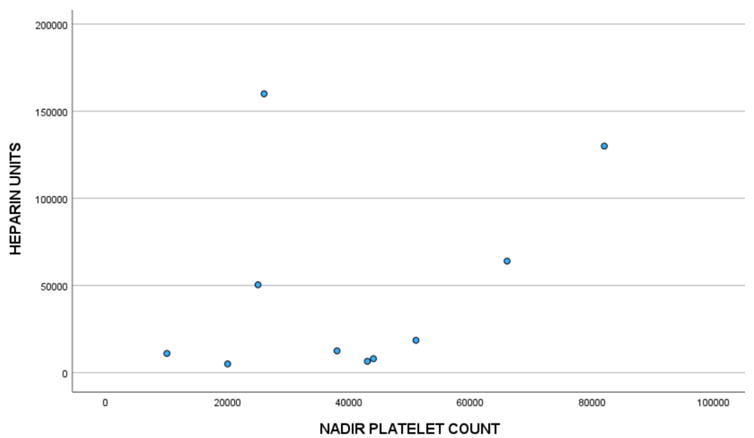
The multiple regression analysis revealed that the patient age variable and nadir platelet count variable were statistically significant, P = .049 and .023, respectively. The patient age range was 36 to 86 years, and range for the nadir platelet count was 10,000 to 82,000/µL (Table 2). Statistical significance was not evident in the UFH dose variable. The R-squared value was 0.764 indicating that 76.4 percent of the variation in the 4T Score can be explained by the predictor (independent) variables. Figure 1 depicts the unstandardized predictive values of all three independent variables on the dependent variable and line of best fit. Figure 2 represents a scatterplot of total UFH units administered versus nadir platelet count resulting in a Pearson correlation coefficient of 0.3, deemed to be a weak correlation.
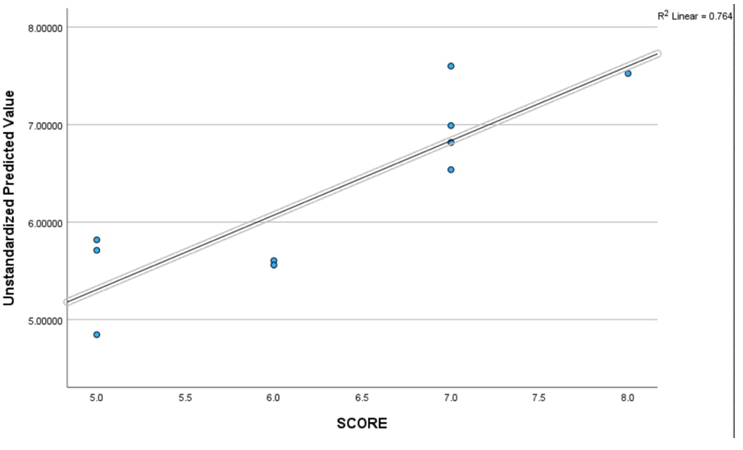
Figure 1: Multiple regression scatterplot depicting the linear relationship between the unstandardized predicted value (y-axis) representing a composite of patient age, UFH dose, and nadir platelet count statistical parameters on the 4T Score (x- axis). The R-squared value indicates that 76.4 percent of the variance in the 4T Score can be explained by patient age, UFH dose, and nadir platelet count.
Discussion
This study represents an analysis of ten case reports of patients diagnosed with HIT using multiple regression. The independent variables nadir platelet count and patient age were found to be statistically significant. Previous studies have found that as persons age the platelet count decreases by approximately ten percent, particularly in person’s ≥ 70 years of age. Segal and Moliterno reported that in a sample of 12,142 participant’s persons aged 70 to 90 years old had a mean platelet count 18,000/µL lower than young adults and this decrease was unrelated to any condition linked to low platelet counts [9]. Santiago et al studied 804 persons aged 2 to 93 years of age and observed the platelet count decreased with increasing age [10]. While the pathophysiological mechanism surrounding decreased platelet counts among older persons has not been elucidated researchers have proposed the drop in platelets may be caused by a diminished hematopoietic stem cell reserve in the bone marrow [11]. In this study there were two patients ≥70 years of age, 86 and 74, whose platelet counts both normalized after UFH was discontinued, 173,000/µL and 249,000/µL, respectively. These findings negate the notion that including Age in the analysis aligns to a confounding variable based on studies that persons in their age group have decreased platelet counts; rather, the drop in platelet count is likely caused by the UFH dose they received. The beta coefficient in the multiple regression analysis for the patient age variable was positive, .031, indicating a direct relationship between the predicator variable and outcome variable; that is for a one unit increase in patient age the outcome variable [4T score] will increase by .031. The statistical significant value may also relate to the presence of thrombosis in patients which is a cogent criteria in determination of the 4T score.
The nadir platelet count was also a statistically significant variable. While thrombocytopenia is viewed as the cardinal manifestation of HIT and the nadir platelet count may represent a fourth of total criteria outlined in Table 1 that encompasses the 4T score, the literature is devoid of a regression analysis utilizing the nadir platelet count as a predictor variable in combination with other variables that are not included in derivation of the 4T score. The range of nadir platelet counts found in this study, 10,000 to 82,000/µL aligns with other reports of HIT with similar diagnoses [12, 13, 14]. The beta coefficient was also positive for this variable (.032) indicating a direct relationship between nadir platelet count and 4T score.
The UFH dose variable was not statistically significant and the Pearson correlation coefficient was positive albeit weak as depicted in Figure 2. The reason for this finding may be due to the affinity of heparin to cellular constituents of endothelial cells and monocytes that define the reticuloendothelial cell clearing mechanism. Saturation of heparin to these cells may interfere with an immune response in forming antibodies that bind to the heparin/PF4 complex on platelets and subsequent findings of thrombocytopenia that can affect a high 4T score.
Saffle JR, et al. [15] conducted a study in which thirty-nine patients received a standard dose of UFH (5000 units every 12 hours) for a period of ten days. Investigators reported no thrombocytopenia was observed in any of the patients [15]. No papers in the literature have analyzed changes in the 4T score and doses of UFH. The Saffle et al study strictly evaluated UFH doses with respect to a single criterion of the 4T score, thrombocytopenia. Luzzatto G, et al. [16] conducted a study involving fifty chronic dialysis patients with end stage renal disease. Patients received UFH totalling 750-16,000 IU per dialysis session. The mean platelet count of patients after exposure to UFH was in the normal range [198,000/µL], with six patients exhibiting thrombocytopenia, albeit none of the patients demonstrated symptoms of HIT. These results reflect the staunch variability seen in patients who receive UFH and resulting platelet counts that in large measure were deemed to be in the normal reference range. The thrombosis criterion of the 4T score has not been correlated to heparin dose in the literature.
Patients in this study were administered alternative therapies to UFH once HIT was diagnosed. These included fondaparinux, apixaban, argatroban, enoxaparin, rivaroxaban and platelet transfusions. All patients recovered from HIT with the exception of one patient that died from sepsis and had a history of coronary artery disease developing HIT after mitral valve replacement; this patient received argatroban once HIT was evident [17].
There were only ten cases found in the literature containing inclusion criteria and this low number is a limitation of the study. COVID-19 has been associated with both venous and arterial thrombosis, and low platelet counts in patients [18]. While two patients were diagnosed with COVID-19 this is not viewed as a limitation as platelet counts in both patients normalized after alternative therapies to UFH were administered, and investigators articulated that the drop in platelet counts were directly linked to UFH exposure.
Conclusion
In this case series study a multiple regression analysis was done revealing statistical significance with the patient age and nadir platelet count variables on the 4T score. Future studies should be conducted employing a higher number of cases with stratification of patient age <70 years and ≥ 70 years to better assess the relationship between Age and HIT.
A fourth variable that should be included in future studies is the Type of HIT in comparing clinical information and outcomes between Type I and II.
References
-
Arepally GM, Padmanabhan A (2021) Heparin induced thrombocytopenia: a focus on thrombosis. Arterioscler Thromb Vasc Biol 41(1): 141-152.
-
Weisman RE, Tobin RW (1958) Arterial embolism occurring during systemic heparin therapy. AMA Archives of Surgery 76(2): 219-227.
-
Arepally GM, Cines DB (2020) Pathogenesis of heparin- induced thrombocytopenia. Transl Res 225: 131-140.
-
Ahmed M, Habis S, Samotowka M, Ahmed M, Michael C (2019) Mesenteric Ischemia caused by heparin-induced thrombocytopenia. Cureus 11(1): e3900.
-
Patriarcheas V, Pikoulas A, Kostis M, Andriani C, Evangelos D (2020) Heparin induced thrombocytopenia: pathophysiology, diagnosis and management. Cureus 12(3): e7385.
-
Warkentin TE, Aird WC, Rand JH (2003) Platelet- endothelial interactions: sepsis, HIT, and antiphospholipid syndrome. Hematology Am Soc Hematol Educ Program pp: 497-519.
-
Hirsh J, Anand SS, Halperin JL (2001) Mechanism of action and pharmacology of unfractionated heparin. Arteriosclerosis, Thrombosis and Vascular Biology 21(7): 1094-1096.
-
Martel N, Lee J, Wells PS (2005) Risk for heparin induced thrombocytopenia with unfractionated and low molecular weight heparin thromboprophylaxis: a meta- analysis. Blood 106(8): 2710-2715.
-
Segal JB, Moliterno AR (2006) Platelet counts differ by sex, ethnicity, and age in the United States. Ann Epidemiol 16(2): 123-130.
-
Santiago M, Ziyatdinov A, Moix N, Agnes M, Manuel S, et al. (2016) Age and gender effects on 15 platelet phenotypes in a Spanish population. Comput Biol Med 69: 226-233.
-
Rossi DJ, Bryder D, Seita J, Hoeijmakers J, Weissman L, et al. (2007) Deficiencies in DNA damage repair limit the function of hematopoietic stem cells with age. Nature 447(7145): 725-729.
-
Choi JH, Luc JG, Weber MP, Morris RJ, Massey HT, et al. (2019) Heparin-induced thrombocytopenia during extracorporeal life support: incidence, management and outcomes. Ann Cardiothorac Surg 8(1): 19-31.
-
Niliys H, Cuker A, Haug S, Nakas C, Schmidt A, et al. (2023) A machine-learning model for reducing misdiagnosis in heparin-induced thrombocytopenia: a prospective, multicenter, observational study. EClinical Medicine 55: 101745.
-
Rostami M, Mansouritorghabeh H (2023) Significance of heparin induced thrombocytopenia in COVID-19: a systematic review and meta-analysis. J Thromb thrombolysis 56(2): 241-252.
-
Saffle JR, Russo J, Dukes GE, Warden D (1980) The effect of low dose heparin therapy on erum platelet and transaminase levels. J Surg Res 28(4): 297-305.
-
Luzzatto G, Bertoli M, Cella G, Fabris F, Zaia B, et al. (1998) Platelet count, Anti-heparin/platelet factor 4 antibodies and tissue factor pathway inhibitor plasma antigen level in chronic dialysis. Thrombo Res 89(3): 115-122.
-
Tugulan C, Change DD, Bates MJ (2021) HIT after mitral valve replacement. Ochsner Journal 21(2): 200-204.
-
Barrett TJ, Bilaloglus S, Cornwell M, Hochman J, Berger JS, et al. (2021) Platelets contribution to disease severity in COVID-19. J Thromb Haemost 19(12): 3139-3153.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies