Misdiagnosed Injuries of Unusual Gunshot Wounds in the Clinical Forensic Practice
Gunshot wounds are common in the forensic practice. The specific features of gunshot wounds usually make it easy to determine the entrance and exit wound. In some cases in the clinical practice, however, gunshot wounds can be misdiagnosed by the clinicians, especially when atypical ammunition has been used or in cases of long range shots, ricochet bullets and shots trough solid material. All of the above mentioned situations can cause morphological changes to the entrance wound which are not specific for a gunshot wound and can lead to misdiagnosis and inappropriate or delayed treatment of the patient, which in some cases can be fatal. This article discusses two cases of misdiagnosis and inappropriate treatment of patients in the clinical practice that were subjected to forensic expertise.
Introduction
Gunshot wounds are common in the forensic practice. Large percentage of the mortality rate is caused by gunshot wounds [1, 2, 3, 4]. The specific features of gunshot wounds make it easy to determine the entrance and exit wound whereas the typical entrance wound occurs when the bullet is traveling on a straight course with negligible yaw and strikes perpendicularly against the body surface. In this scenario, one would expect a punched out, circular defect surrounded by a thin abrasion rim. Variations of the wound appearance can occur due to bullet entry angle and the body surface struck making eccentric or even irregular abrasions surrounding the defect not uncommon [5, 6]. In some cases in the clinical practice gunshot wounds can be misdiagnosed by the clinicians, especially when atypical ammunition has been used or in cases of long range shots, ricochet bullets and shots trough solid material [5, 6, 7]. An atypical entrance wound or even multiple entrance wounds are primarily the result of an unstable, non-axial flight of a bullet or of missile deformation [6], but may also be caused by the use of atypical ammunition and weapons such as homemade firearms [5]. The disadvantages in using cartridges of a smaller caliber than those designed for the gun include: lack of accuracy, low velocity, barrel fouling, damage to the chamber, or leakage of hot gases from the barrel and chamber because these cartridges do not occlude the barrel [8, 9].
Case 1
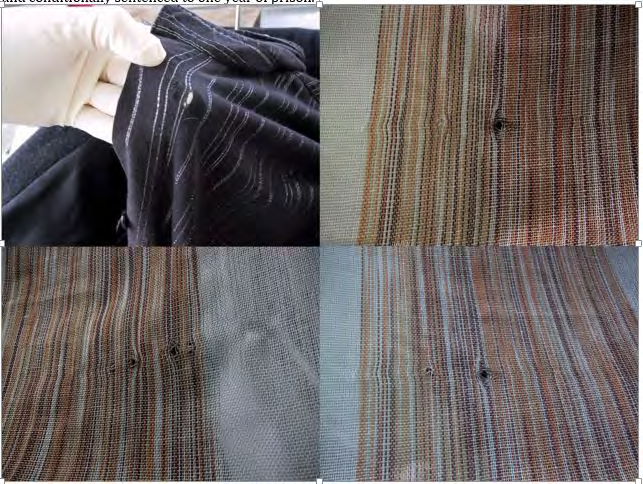
A 19-year old female was injured at the New Year’s celebration party in the central square of Skopje in 2004. She suddenly felt pain in the left side of her chest and immediately went to the urgent surgical center of the University Clinic in Skopje. She informed the medical staff that she thought she had probably been injured by a firecracker. Her clothes were removed without anyone examining them and the surgeon performing the physical examination used a surgical instrument (pean forceps) to see if there was any canal leading from the wound into the chest cavity (Figure 1). He did so by inserting the instrument from the front to the back. He noted there was no canаl and ordered an X-ray of the chest cavity. The X-ray of the chest cavity did not show the presence of a foreign body (corpora aliena), thus he decided to give her the following diagnosis followed by a question mark: Vulnus punctum, Vulnus sclopetarium?.
The girl was admitted to the hospital for surveillance. The next day she had menstrual bleeding with severe pain in her stomach and she confirmed that her menstrual bleeding was expected and that she usually had such pain during menstrual bleeding. In the next four days several abdominal surgeons examined her and they concluded that her abdominal pain was a result of the menstruation. In the medical documents they stated cut wound (Vulnus scissum) as a new diagnosis. On the fourth day of hospitalization she died and the clinicians asked for forensic autopsy.
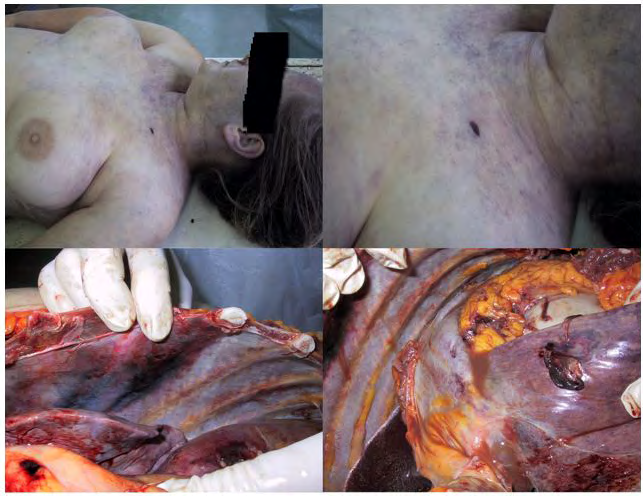
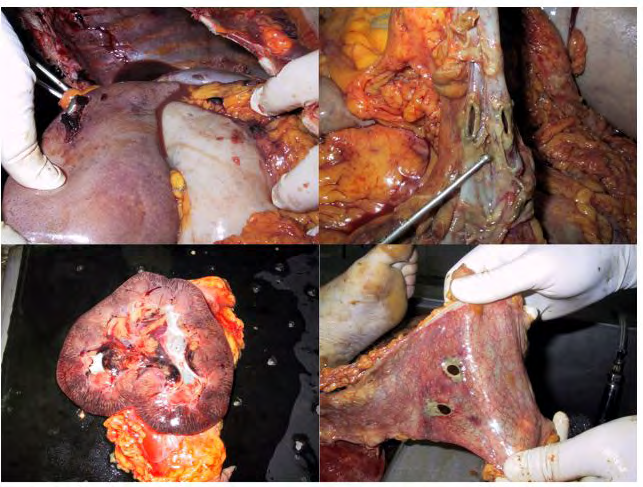
Autopsy revealed atypical entrance gunshot wound in the left subclavicular region, with 1cm length and 0.6 cm width, positioned transversally, with skin laceration of 0.6x0.2 mm. The wound canаl extended from the entrance wound downwards through the chest cavity, passing between the third and fourth rib injuring the intercostal muscle, thereby crushing the front side of the upper lobe of the left lung. It then continued with a circular defect on the left diaphragm lobe, two circular defects on the transversal colon that were surrounded by necrotic tissue, ending with a projectile found in the retroperitoneal cavity in the fatty tissue behind the left kidney (Figures 2 & 3). During autopsy, 700 ml of intestinal content was removed from the abdominal cavity with findings of diffuse purulent peritonitis. The cause of death was purulent peritonitis following gunshot wound. The investigating judge initiated criminal proceedings against all doctors involved in her treatment. One of the doctors was found guilty and conditionally sentenced to one year of prison.
Case 2
An older woman suddenly felt severe pain in her posterior thoracic region while she was gardening under a quince tree. She went to the General City Hospital where the doctor who examined her concluded that she had a puncture wound in the posterior thoracic region caused by the stalk of the quince fruit and sent her home. The next day she started spitting blood and went back to the hospital. This time the doctor ordered an X-ray of her chest cavity, but the radiologist did not see anything suspicious nor did he see any foreign body, therefore was she sent home with the diagnosis of Bronchial asthma (Asthma bronchiale). On the fifth day from the injury, the woman went back to the hospital because she was still spitting out blood and on this occasion the doctors performed an ultrasound exam which showed a metal particle in the thoracic cavity. She was operated on and the projectile was removed from her thoracic cavity. The investigating judge initiated criminal proceedings against all the doctors involved in her treatment. One of the doctors was found guilty and conditionally sentenced to one year of prison.
Discussion
Forensic expertise, especially autopsy, is of crucial importance to the determination of the cause, manner and circumstances of death. Therefore, it represents the golden standard in the evaluation of violent or unclear cases of death in line with Recommendation no. R (99) 3 of the Committee of Ministers to member states on the harmonization of medico-legal autopsy rules [10, 11]. The investigation of gunshot deaths often presents a challenge to the forensic pathologist. All available data from the death scene investigation, radiological and laboratory analyses and, in particular, autopsy findings have to be considered in order to reconstruct the events prior to the death and to accurately determine the manner of death.
The forensic pathologist needs in-depth knowledge and vast practical experience to handle cases that appear to go beyond the ordinary [12]. On the other hand, doctors in clinical practice can sometimes misdiagnose gunshot wounds especially if wounds lack the usual and expected features, such as the shape and appearance of the entrance wound, the trajectory of the projectile or the clinical findings. Misdiagnosis can result from multiple reasons such as misinformation, superficial approach, lack of experience, inappropriate local examination, lack of additional examinations, mistreatment, poor communication and collaboration, system error, lack of multidisciplinary approach, inadequate monitoring after a procedure and failure to take proper precautions.
In our case reports we showed one patient who was injured with a fatal outcome and another patient who developed health complications because of a delay in treatment. All of the reasons mentioned above did not exonerate the clinical doctors from their responsibility in the justice system. Cases of medical errors are processed through the civil court, whereas cases of gross negligence are handled by the criminal court. In most countries, the majority of the misdiagnosed gunshot wound cases are processed in the civil courts. In our two cases the convicted doctors were prosecuted under the criminal charge of reckless treatment of patients and gross negligence prescribed in the Criminal Code of Republic of North Macedonia under article 207. Article 207 reads that lack of diligence or care when administering treatment, inappropriate approach during diagnosis or treatment, regardless of whether it be on a conscious and voluntary basis or resulting from reckless omissions in the discharge of the doctor‘s legal duty having consequences to another party, does not release the doctor from guilt [13, 14].
Conclusion
Investigation of a possible incident of gunshot wound requires the collaboration of clinical doctors, forensic pathologists, radiologists, crime scene investigators, ballistics analysts and firearm examiners. When clinicians encounter atypical gunshot wound caused by the use of atypical ammunition, long-range shots, ricochet bullets or shots through solid material, they should be aware of certain features of the atypical entrance wound in order to diagnose and treat it promptly. Unlike typical gunshot wounds, the shape of atypical entrance wound can range from round to elliptical, large or even irregular with ragged, abraded margins. Furthermore, pseudo-stippling or pseudo- gunpowder tattooing around the bullet hole may be seen when the victim is near the ricochet target. Similarly, tumbling abrasions are produced when the bullet tumbles tangentially across the skin before entering the body. In the cases of a ricochet entrance wound, the bullet wipe is less pronounced compared to a direct shot [15, 16, 17].
It is important for the surgeons providing the treatment, to make careful excisions during surgical care of gunshot wounds and send them for histological analysis and tracing for gunshot residue particles, with a warning note not to put the excised tissue in alcohol or formalin to avoid the surface of the skin being washed.
Clinical doctors should pay close attention to the circumstances of the incident and obtain as much information from the patient, examine their clothes for any damage carefully handling them to avoid contamination [18]. Understanding and analysing the causes of medical errors is the only way of preventing them [19, 20].
References
-
Rubenstein A, Wood SK, Levine R, Hennekens CH (2019) Alarming trends in mortality from firearms among United States schoolchildren. Am J Med 132(8): 992-994.
-
Bauchner H, Rivara FP, Bonow RO, Bressler NM, Disis ML, et al. (2017) Death by Gun Violence-A Public Health Crisis. JAMA 318(18): 1763-1764.
-
Fowler KA, Dahlberg LL, Haileyesus T, Annest JL (2015) Firearm injuries in the United States. Prev Med 79: 5-14.
-
Lee LK, Fleegler EW, Farrell C, Avakame E, Srinivasan S, et al. (2017) Firearm Laws and Firearm Homicides: A Systematic Review. JAMA Intern Med 177(1): 106-119.
-
DiMaio VJM (1999) Gunshot Wounds Practical Aspects of Firearms, Ballistics, and Forensic Techniques. 2nd (Edn.), Washington, DC: CRC Press.
-
Tsokos M, Voigt Z, Ehrlich E (2012) A typical gunshot entry wound. Forensic. Sci Med Pathol 8(4): 460-462.
-
Stankov A, Jakovski Z, Pavlovski G, Muric N, Dwork AJ, et al. (2013) Air gun injury with deadly aftermath--case report. Leg Med (Tokyo) 15(1): 35-37.
-
du Toit-Prinsloo L, Morris NK, Saayman G (2014) Tandem bullet injury: an unusual variant of an unusual injury. Forensic Sci Med Pathol 10(2): 262-265.
-
Simmons GT (1997) Findings in gunshot wounds from tandem projectiles. J Forensic Sci 42(4): 678-681.
-
Kirchhoff SM, Scaparra EF, Grimm J, Scherr M, Graw M, et al. (2016) Postmortem Computed Tomography (PMCT) and Autopsy in Deadly Gunshot Wounds--A Comparative Study. Int J Legal Med 130(3): 819-826.
-
https://www.coe.int/t/dg3/healthbioethic/texts_and_ documents/RecR(99)3.pdf
-
Tattoli L, Schmid S, Tsokos M (2014) Three Rounds as Tandem Bullets: Unusual Findings in a Case of a Suicidal Gunshot to the Head. Forensic Sci Med Pathol 10(4): 613-618.
-
Official Gazette of the Republic of Macedonia No.96 of 10.11.2015.
-
Mullock A (2018) Gross Negligence (Medical) Manslaughter and the Puzzling Implications of Negligent Ignorance: Rose v R [2017] EWCA Crim 1168. Med Law Rev 26(2): 346-356.
-
Yong YE (2017) A Systematic Review on Ricochet Gunshot Injuries. Leg Med (Tokyo) May 26: 45-51.
-
Molina D, Rulon J, Wallace E (2012) The Atypical Entrance Wound: Differential Diagnosis and Discussion of an Unusual Cause. Am J Forensic Med Pathol 33(3): 250-252.
-
Kirchhoff SM, Scaparra EF, Grimm J, Scherr M, Graw M, et al. (2016) Postmortem computed tomography (PMCT) and autopsy in deadly gunshot wounds—a, comparative study. Int J Legal Med 130(3): 819-826.
-
Branas CC, Han S, Wiebe DJ (2016) Alcohol Use and Firearm Violence. Epidemiol Rev 38(1): 32-45.
-
Yazıcı YA, Sen H, Aliustaoglu S, Sezer Y, İnce CH (2015) Evaluation of the Medical Malpractice Cases Concluded in the General Assembly of Council of Forensic Medicine. Ulus Travma Acil Cerrahi Derg 21(3): 204-208.
-
Maeda B (2009) Medico-legal autopsies as a source of information to improve patient safety. Leg Med (Tokyo) 1: 76-9.
- Narcotics and Digital Forensics: Bridging Crimes in the Digital Age
- Ethics in Forensic Psychiatry: Principles, Dilemmas, and Human Rights
- Impact of Acute Stress on Attentional Orienting to Social Cues
- Head Injury and Intracranial Hemorrhage in Western Region of Libya
- A Forensic Study on Handedness: Examination of Handwriting Features in Right and Left Handed Writers
- Techniques for Latent Fingerprint Development Using Natural and Synthetic Powders: A Review