Mesenchymal Chondrosarcoma of the Maxillary Sinus: Reporting Case with Good Response to Radiotherapy
Introduction: Mesenchymal chondrosarcoma (MC) is a rare variant of chondrosarcoma (CS) that accounts for up to 3- 10% of all CS. The head and neck localization is rare and may involve the sinonasal tract, jaws, larynx or skull base. It has been described as an aggressive neoplasm with high tendency for recurrences and delayed metastasis. Case report: We reported a case of a 41-years-old women complaining of right facial pain. Examination revealed hemorrhagic mass with bucco-palatal extension and causing displacement upper 2nd premolar teeth. Computed tomography (CT) scan revealed a lytic tumor arising of the left maxillary bone and extending into the orbit and the infratemporal fossae. Transoral biopsy was performed according to Caldwell luc technique. Histological examination and immunohistological study confirmed the diagnosis of high grade MC .Since the tumor was unresectable, the treatment was definitive concomitant chemoradiation (CCR) at the dose of 64Gy over 46 days by intensity modulation radiation therapy (IMRT), with a good response. The patient remains free of disease 12 months after treatment. After that she had a recurrent non metastatic disease, Combination chemotherapy with vincristine, doxorubicin, cyclophosphamide, ifosfamide, Mesna and etoposide was administered. Conclusion: MC of the sinonasal tract is an aggressive tumor with a predilection for young women. Recurrences develops in approximately one-third of patients and seems to predict a poor prognosis. Multimodal treatment based on surgery radiation and chemotherapy appears to improve clinical outcome.
Introduction
Mesenchymal chondrosarcoma (MC) is a rare variant of chondrosarcoma (CS) that accounts for up to 3-10% of all CS [1]. The head and neck localization is rare and may involve the sinonasal tract, jaws, larynx or skull base. There is predilection for maxillofacial skeleton; less often involves the soft tissue site in head and neck. It has been described as an aggressive neoplasm with high tendency for recurrences and delayed metastasis [2]. They usually occur in middle aged individuals, but are rare in young patients, with predilection for anterior portion of maxilla [3]. The diagnosis is challenging and may be assisted by molecular pathologic techniques. Management is mainly surgical. Although adjuvant radiation appears to convey some benefit by reducing tumor bulk when these lesions have extended beyond bony confines, there is no evidence to suggest that this is associated with improved outcome. The review of literature shows that a very few cases of maxillary MC have been reported so far in the English literature.
Case Report
A 41-years-old Moroccan woman was referred to our hospital with a history of right facial pain since one month. Physical examination revealed hemorrhagic mass with bucco-palatal measuring 5x4.5cm extension and causing displacement upper 2nd premolar teeth.
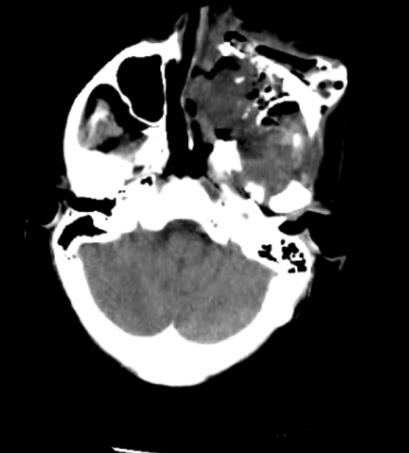

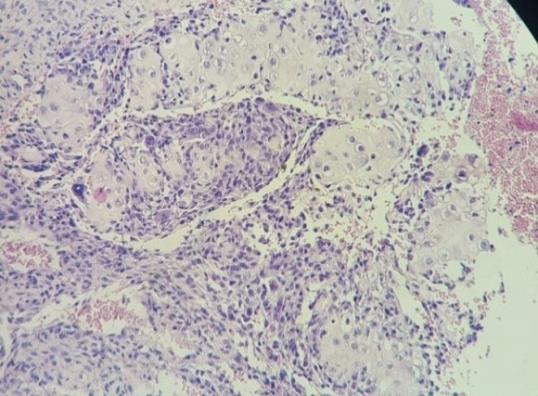
Computed tomography (CT) scan revealed an heterogeneously enhancing mass in the left maxillary sinus, the posterolateral wall of the maxillary sinus was invaded and the mass had progressed into the pterygopalatine fossa and infratemporal fossa (Figure 1). Transoral biopsy was performed according to Caldwell luc technique. Microscopic examination of a biopsy sample from the tumor and immunohistological study confirmed the diagnosis of high grade MC. Tumor cells were diffusely reactive for CD99 (Figures 2A-2C).

(DVH), (Figures 3A-3C), weekly portal imaging were performed to insure the treatment quality. We associated cisplatin (CDDP) 100 mg/m² (J1=J21). The adverse events due to radiation was grade 2 mucositis. Grade1 radiodermatitis and grade 2 conjunctivitis. After radiotherapy. We can observe spectacular tumor shrinkage; the patient remains free of disease 12 months after therapy.
International Journal of Nuclear Medicine & Radioactive Substances
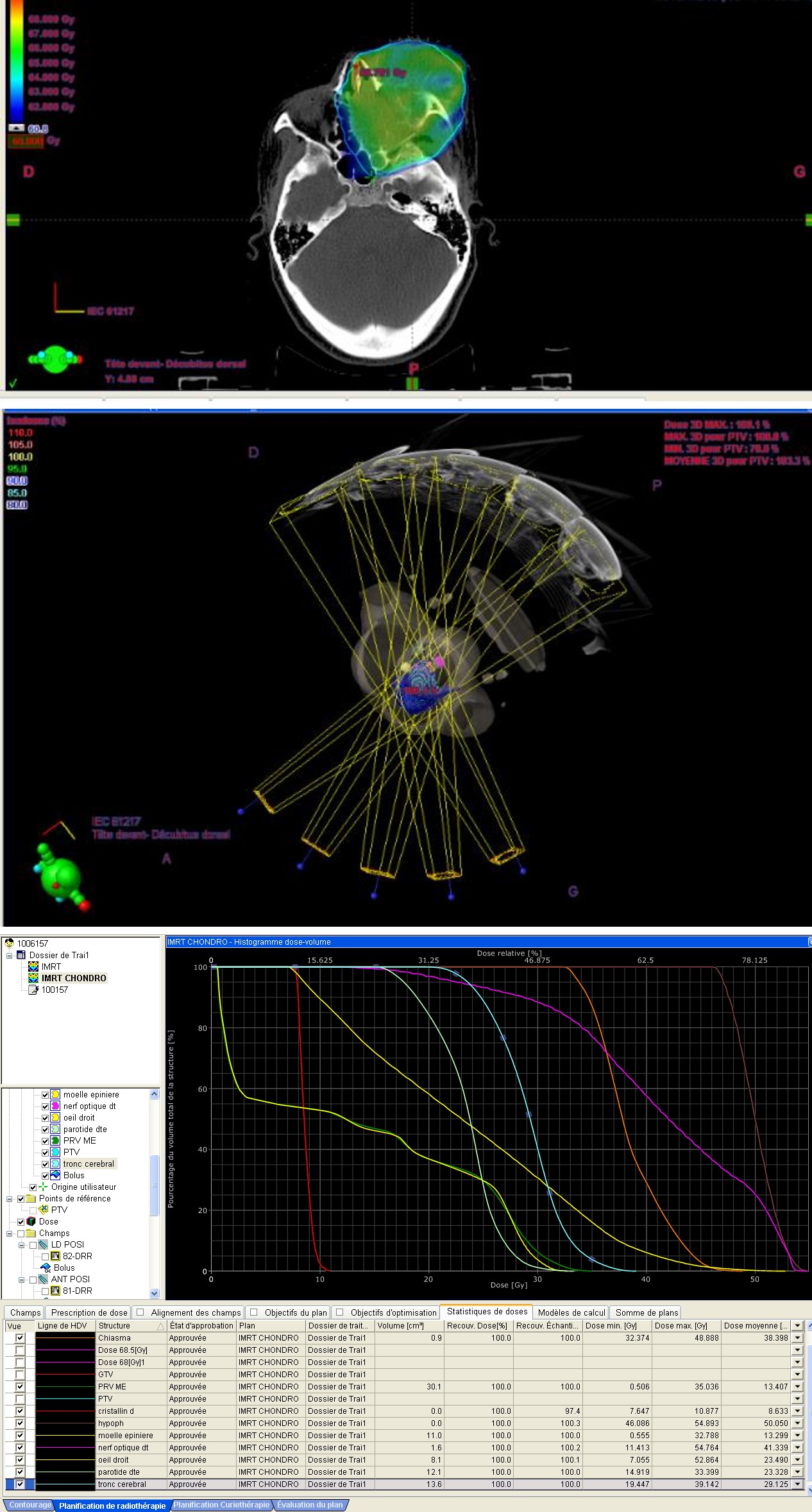
Figure 3A: Disposition of multiple beams using IMRT.
Figure 3B: Tumor coverage by 95 % of the prescribed dose.
Figure 3C: Histogramme dose volume DVH.
After a one year, she had a recurrent non metastatic disease, chemotherapy regimen originally reported to be effective for high-grade sarcomas was VAC-IE. Day 1: vincristine 2mg total dose+ doxorubicin 30 mg/m2/day (days 1) + cyclophosphamide 1200mg/m²/day+ mesna1200mg/m², day21: ifosfamide 1800 g/m2/day (days 1–5) + etoposide 100mg/m² (day1- 5) The patient received three courses of triweekly chemotherapy, which proved to be effective, the main adverse events due to chemotherapy were leukopenia (grade 3, courses 1), neutropenia (grade 3, courses 1), and febrile neutropenia (grade 3, course 3). The patient required subcutaneous G-CSF (granulocyte-colony stimulating factor) injection every course. No cardiac- related events or hemorrhagic cystitis was observed. After 3cycles, she developed a large facial fistula, returning to the clinical oncology department to continue chemotherapy.
Discussion
Chondrosarcoma of the head and neck is very rare. Only a few cases have been presented in the English
International Journal of Nuclear Medicine & Radioactive Substances
literature. By definition, it is a locally aggressive or malignant group of cartilagenous matrix-producing neoplasms tumor and neoplastic osteoid should not be present according to the World Health Organization (WHO) [4]. Most of Chondrosarcoma occur in 3rd–6th decade of life [3], the present case also falls in 4th decade.
The maxilla is the most affected bone and usually has slow growth, but it can be locally aggressive with a high rate of recurrence. Other primary sites in the head or neck are the jaw, nasal cavity and maxillary sinus [5], the present case was reported in the left maxillary sinus.
MC show no specific clinical signs and symptoms. The predominant symptom is usually a painless mass or swelling (53%), as in the present case. However, other reported symptoms are nasal obstruction (32%), epistaxis (32%) tooth mobility (24%) [6].
Histologically, diagnosis is always a challenge because cartilaginous neoplasms have a biphasic pattern consisting of well-differentiated cartilage lobules, which resemble those seen in a low-to intermediate grade chondrosarcoma, and a proliferation of undifferentiated blue small round cells that simulate the cell type of Ewing’s sarcoma [7, 8]. Evan's and co-workers have attempted to associate the histologic grade (Grade I to III) of chondrosarcoma with the ultimate biologic behavior of the tumor, depending upon the cellularity, nuclear size, and presence of mitotic figures, multinucleation, spindle cell formation and mineralization in the form of osseous development at the edge of the cartilaginous lobules [9]. We used the WHO (2013) [5] classification of bone tumors (grades I– III).We also add that in bone sarcomas, the histologic subtype often determines grade. For example, mesenchymal chondrosarcoma and the dedifferentiated chondrosarcoma are always considered high grade [5]. Immunohistochemically, chondroid areas are positive for vimentin and CD99, but not for S-100 protein [7, 10].
The level of evidence upon which treatment recommendations is based is relatively low. The consensus is that surgical treatment is the most effective therapy for Chondrosarcoma. Complete resection is considered the standard treatment for Chondrosarcoma and has been reported to be an individual prognostic factor for local recurrence and overall survival mainly in extremity cases [11]. Dissection of the cervical lymph node is not routinely performed due to a low incidence of lymph node metastases [7]. Sei YL, et al. [12] experienced 8 cases during a 15-year period at Yonsei University Medical College, they conclude that complete excision of the primary site is of utmost importance for successful treatment. Although the number of cases was small, and despite considerable controversy, they speculate that postoperative radiotherapy may have some role in the treatment of chondrosarcoma, considering the 2 cases reported with positive margin that were successfully treated with postoperative radiotherapy.
However, in the head and neck region, it is sometimes difficult to completely resect the tumor with a safe margin. Even if it is operatively resectable, wide surgical resection can cause not only cosmetic and functional deterioration but also elevate the risk of perioperative complications. In such cases, the concomitant chemo radiation CCR therapy can be used to decrease the size of the tumor and making the definitive therapy more effective, as we show here in the present case. Radiation is performed for palliative cases, unresectable cases or as an adjunctive therapy in cases of residual disease, but not as an initial or single treatment [5].
Chondrosarcoma are relatively radio resistant tumors and therefore, after multidisciplinary discussions, very few of these patients are offered radiotherapy [12]. Due to the limited number of cases, the efficacy of CCR on head and neck lesions is also obscure. The second problem is the anatomical close relation between the tumor and these critical normal structures limits the dose that can be delivered with conventional radiation treatment. Charged particle radiotherapy combined with three dimensional treatment planning results in superior dose distribution that allows delivery of high tumor dose with acceptable dose to the normal tissues [13]. The prognosis for patients with MC is poor because of the tumor’s tendency to local recurrences or metastasis even after a long disease free interval. The main prognostic factors are surgical resection, stage, grade and primary site. The mesenchymal and dedifferentiated forms are known to have poor prognoses. Tumor recurrence is relatively common and usually occurs due to an incomplete resection of the tumor. It also may be due to the local spread of the disease or surgical technique issues [5]. The overall 5-year survival for low grade chondrosarcoma after complete resection is between 55-75% [14]. The reported patient has done well after 1 year of previous CCR and despite recurrence, could be managed by chemotherapy and is doing well on follow-up for the last more than 6 months.
Hence adequate treatment and a lifelong follow-up after surgery is recommended for patients with mesenchymal Chondrosarcoma of the maxillofacial region. The case we present here is only a case report, and International Journal of Nuclear Medicine & Radioactive Substances
the follow-up period is still very short. As with MC of the extremities, metastasis or local recurrence can occur after a certain period, and we are currently following-up the present patient very closely. We hope more data concerning the use of CCR on head and neck lesions are reported and that the benefit is clearly revealed. Recent data identified alterations in CDKN2A/ RB1 as predictors of decreased double strand break formation after radiotherapy in chondrosarcoma tissue, whether selection for radiotherapy can be based upon an intact Rb pathway should be further investigated [15]. A recurrent HEY1-NCOA2 gene fusion has been identified in nearly 80% of MCs, and more recently a novel t(1;5)(a42;q32) translocation resulting in an IRF2BP2-CDX1 has been described in an extra osseous MC. Analysis of tumors for these alterations can be used in diagnostically challenging cases to aid in diagnosis [16].
Conclusion
Chondrosarcoma of head and neck is a very rare tumor with malignant potential. Diagnosis is made on the basis of radiological and pathological features. Prognosis depends upon the grade of the tumor and location of primary tumor. The tumor being radio-resistant, widest possible exposure and wide surgical excision are considered the treatment of choice. Post-operative follow- up is mandatory as the recurrent disease is more difficult to treat.
Consent
Written informed consent for publication of this report and images was obtained from the patient.
Acknowledgement
The authors thank Dr. Amal Douida working in pathology lab of university hospital Hassan II fez for her thorough assistance in gathering pathological report and images.
References
-
Jaitley V, Gupta S. (2011) Mesenchymal Chondrosarcoma of maxilla: A rare case report. Med Oral Patol Oral Cir Bucal 16(4): 493-496.
-
Knott PD, Gannon FH, Thompson LD (2003) Mesenchymal chondrosarcoma of the sinonasal tract: a clinicopathological study of 13 cases with a review of the literature. Laryngoscope 113(5): 783-790.
-
Kumar SRR, Anuradha A, Kumar NK, Kuberappa HP, Venkata RK, et al. (2017) Mesenchymal chondrosarcoma: An unusual lump in posterior maxilla. Int J case rep Image 8(5): 300-304.
-
Fletcher CDM, Bridge JA, Hogendoorn PCW (2013) WHO classification of tumors of soft tissue and bone, IARC, Lyon.
-
Quevedo FC, Quevedo FB, Barauna Neto JC, Napolitano E, Dirce MC et al. (2017) Case report: Chondrosarcoma of the head and neck. Human Pathol: Case Reports 7: 4-7.
-
Kumar M, Suresh K, Patil M, Pramod R, Yusuf R, et al. (2014) Mesenchymal chondrosarcoma of posterior maxilla: Report of a case with brief literature review. Ann Med Health Sci Res 4(1): 49-52.
-
Kumaraswamy Naik LR, Pushparaja S, Teerthanath S, Jagdish MH, Shroff SE (2008) Mesenchymal chondrosarcoma affecting the mandible. J Oral Maxillofac Pathol 12(1): 29-33.
-
Riedel RF, Larrier N, Dodd L, Kirsch D, Martinez S, et al. (2009) The clinical management of chondrosarcoma. Curr Treat Options Oncol 10: 94- 106.
-
Evans HL, Ayala A, Romsdahl NM (1977) Prognostic factors in Chondrosarcoma of bone. A clinicopathologic analysis with emphasis on histologic grading. Cancer 40(2): 818-831.
-
Pellitteri PK, Ferlito A, Fagan JJ, Suárez C, Devaney KO, et al. (2007) Mesenchymal chondrosarcoma of the head and neck. Oral Oncol 43(10): 970-975.
-
Spillane AJ, A’Hern R, Judson IR, Fisher C, Thomas JM (2000) Synovial sarcoma: a clinicopathologic, staging, and prognostic assessment. J Clin Oncol 18(22): 3794-3803.
-
Sei YL, Young CL, Mee HS, Jae YS, Won SL, et al. (2005) Chondrosarcoma of the Head and Neck. Yonsei Med J 46(2): 228-232.
-
Abhishek J, Avik KJ, Biswajit S (2008) Chondrosarcoma of nose and paranasal sinus-a rare presentation. Indian J Otolaryngol Head Neck Surg 60(3): 284-286.
-
Aniece C, Parmod K, Des Raj B, Poonam S, Pervez K (2008) Chondrosarcoma of the Maxilla-Recurrent 10(2). International Journal of Nuclear Medicine & Radioactive Substances
-
de Jong Y, Ingola M, Briaire-de Bruijn IH, Kruisselbrink AB, Venneker S, et al. (2019) Radiotherapy resistance in Chondrosarcoma cells; a possible correlation with alterations in cell cycle related genes. Clin Sarcoma Res 9: 9.
-
William MM, John DR, Mark TS, Bruce KS, Nancy PM (2016) Mesenchymal Chondrosarcoma. Int J Particle Therap Fall 3(2): 300-304.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO