Contribution of 18FDG PET in Atypical HORTON Disease
The aim of this paper is to illustrate the value of 18F-FDG PET scans in the management of Horton's disease through a case report and to review the literature on the characteristics of this condition and the various imaging tests used in the diagnostic process.
Introduction
The pathogenic basis of vasculitis is inflammation of the vessel wall. This inflammation can affect all three tunics of the vessel, i.e. the endothelium, the media and the adventitia. The ability to visualise this inflammation without the need for invasive techniques is a definite advantage. FDG PET scans can be used for the diagnosis and initial assessment prior to treatment of medium- and large-calibre arterial vasculitides (Horton’s, rheumatoid arthritis, Takayashu) in patients presenting a suggestive picture or in patients presenting a fever with unexplained long-term inflammatory syndrome, as well as for the therapeutic follow-up of lesions that are initially fixating prior to treatment.
Objective
In this work, we present the case of a patient in whom rheumatologists suspected Horton’s disease in the absence of any functional signs, particularly in the external carotid territory.
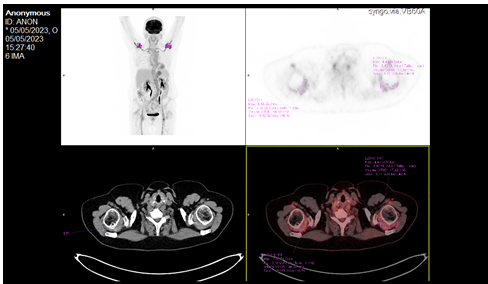
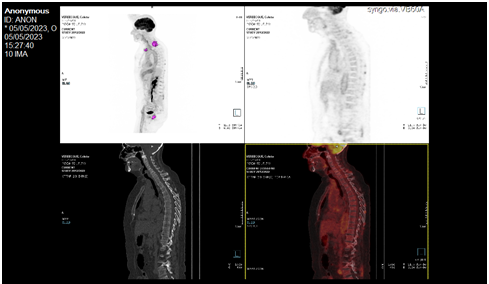
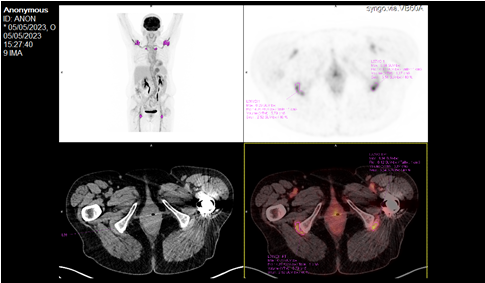
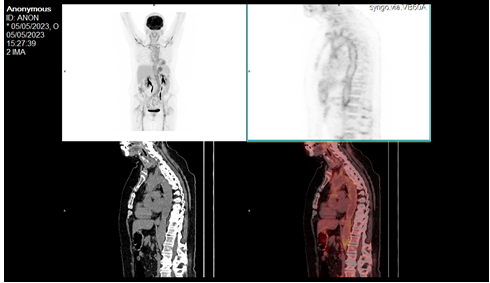
A 71-year-old female patient consulted for a deterioration in her general condition, with fever progressing over 4 months, loss of 5 kg over several months, and asthenia with night sweats. The history also revealed scapulalgia and neck pain with a history of phlebitis of the right lower limb two years previously, for which no aetiology was identified and for which the patient is still receiving treatment with Xarelto®(Rivaroxaban). The clinical examination was practically normal. She had a blood test (CBC, liver function tests, blood sugar) which showed no significant abnormalities apart from a slight increase in GGT (gamma-glutamyl transferase) ; this was supplemented by an elevated ESR of 26 (normal <20), concluding that she had a biological inflammatory syndrome. She also underwent a thoracic-abdominal-pelvic CT scan, which was unremarkable apart from a discrete isolated homogeneous splenomegaly. In view of this discreet splenomegaly, with nothing to compare it with, and the absence of any other abnormality on the CT scan that might explain the clinical and biological picture, a PET scan was ordered to look for vasculitis of the large vessels: The diagnosis was made, revealing marked hypermetabolism of the walls of the large vessels and moderate hyperactivity in the periarticular and sternoclavicular regions, as well as in the tendon insertions of the hips, shoulders and interspinous region (Figures 1-5) all of which suggested vasculitis of the large trunks, and therefore possible Horton’s disease, especially as there were scintigraphic signs of pseudopolyarthritis rheumatica.

The patient was put on corticosteroid therapy at 0.7 mg/ kg, i.e. Prednisone 60 mg/day, with adequate dietary calcium intake (3 dairy products, 1 fruit and 1 vegetable/day). As for vitamin D, her GP suggested a treatment with Colecalciferol 50,000U every month. One month later, the patient regained his weight and his shoulder pain disappeared; the clinical examination revealed well-defined pulses without murmurs (temporal, carotid and radial), and abdominal and cardiac palpation and auscultation were unremarkable. Biologically, the CRP had risen to 21.6 from 128 mg/l. The decision was made to reduce the prednisone by 10% every 15 days, while encouraging the patient not to drop the corticosteroid abruptly, and then to maintain monthly biological monitoring with CBC, CRP, ionogram, blood sugar and ESR.
Discussion
Systemic vasculitides are a group of diseases characterised by damage to the blood vessels. The walls of these blood vessels are the site of inflammation resulting in narrowing or obstruction of their lumen, thus impeding the passage of blood to the various organs. These vasculitides are classified according to the size of the blood vessels affected by the inflammation [1].
Giant cell arteritis (GCA), or Horton’s disease, is a vasculitis of the large arteries. GCA affects people over the age of 50, but occurs mainly from the age of 70 onwards, affecting women 3 times out of 4. The name « giant cell arteritis » is the most commonly used terminology worldwide, replacing the term « Horton’s disease; traditionally used in French-speaking countries. This inflammatory vascular disease is located preferentially in the branches of the external carotid arteries, the ophthalmic arteries and their branches and the vertebral arteries, and this explains its main clinical manifestations in the head. In one in three cases, GCA is accompanied by aortitis, which is usually sub- clinical, and some GCA present as isolated aortitis [2]. It is probably underestimated clinically because the lesions are often asymptomatic and histological confirmation is rarely obtained [3].
There are no pathognomonic markers for HA. Contrary to popular belief, C-reactive protein (CRP) appears to be at least as sensitive as sedimentation rate (ESR) in diagnosing HA. On the other hand, the specificity of these two markers is low, but increases slightly with their combination [4].
Key Points (Diagnosis)
- Any unusual headache of recent onset in a person over 50, particularly after the age of 70, should raise the suspicion of GCA.
- Other suggestive signs include visual signs (transient or permanent loss of vision or diplopia), claudication (or pain) of the jaw, hyperaesthesia of the scalp, protrusion and induration of the temporal arteries, PPR and general signs.
- An GCA should also be considered in the case of any persistent isolated inflammatory syndrome.
- Temporal artery biopsy (TAB) is the gold standard for diagnosing GCA.
- A diagnosis of GCA can also be made in the event of a hypoechoic halo of the temporal arteries, observed on Doppler ultrasound by an experienced operator.
- Evidence of aortitis or inflammatory involvement of the main branches of the aorta by 18FDG PET, CT angiography, MRI angiography or Doppler ultrasound is also diagnostic of CAG.
With regard to metabolic imaging, which is the subject of this work, 83% of patients with Horton’s arteritis have PET- scan positive lesions in the subclavian, aortic and femoral arteries [5].
A broader reflection on the nature of the arterial fixations observed on 18FDG PET seems appropriate in the light of the data in the literature. Clinical and experimental studies of the biodistribution of 18-FDG have described constant and relatively intense uptake of this tracer in the brain and urinary tract. Myocardial uptake is less constant, and more often than not dependent on fluctuations in metabolism during the transition from glucose to fatty acids. Binding that varies in intensity and frequency can also be seen in the liver, spleen, bone marrow, skeletal muscle, thyroid and digestive tract [3].
However, physiological vascular uptake of 18fluorodeoxyglucose is virtually nil, providing an excellent target/background ratio [6]. And with good reason: after intravenous injection of 18FDG, blood clearance of the radiotracer is so rapid that after one hour post-IV, circulating activity is minimal or even negligible. Consequently, any arterial fixation of the glucose tracer cannot be attributed solely to its presence in the circulatory system [3]. However, the mechanisms of 18FDG uptake in medium- and large- calibre arteries are still hypothetical. FDG uptake parallels disease activity. This results in arterial hyperfixation and enables the extent of lesions and disease activity to be visualised in a single acquisition. The abnormalities typically observed are located in the large vessels (aortic arch, descending thoracic aorta, subclavian, axillary and primary carotid arteries), are often bilateral and symmetrical and are characterised by linear and continuous hypermetabolism [6]. The literature has already demonstrated the ability of metabolic imaging to identify sub-clinical aortitis, which is likely to progress to aortic dissection or aneurysm, for example [7].
Joint inflammation (bursitis, synovitis) or periarticular inflammation, particularly of the scapular and pelvic girdles, seen on scintigraphic images in the form of extracapsular hypermetabolism, is, apart from the clinical and biological data, a possible differential sign in favour of Pseudopolyarthritis rheumatica [8]. Sometimes PPR appears to be isolated, but a few months later arteritis develops, particularly in arterial branches arising from the aorta or in the aorta itself, leading to the conclusion of Horton’s disease [6].
In addition, PET scans do not provide sufficient resolution to visualise temporal inflammatory disease, due to the small diameter of the temporal arteries (<2 mm) and the proximity of very intense normal cerebral metabolism, which may also « mask » weaker vascular fixation [9]. In other words, although 18FDG PET can visualise medium- and large-calibre arteritis, it cannot be used to make an aetiological diagnosis. PET alone cannot formally conclude that it is Horton’s arteritis, and temporal artery biopsy is not always helpful, given the segmental and focal nature of the vascular involvement [10]. Hence the importance of a broader diagnostic approach, which involves combining clinical-biological, morphological and histological criteria with metabolic criteria [10].
The clinical cases described in the literature illustrate the potential interest and provide documented proof of metabolic imaging in the assessment of the extension of AGC, unlike angiography, CT and/or MRI, enabling sub-clinical inflammatory arteriopathy to be detected by means of a single whole-body analysis and exploration. Lastly, because it is non-invasive, 18FDG PET is the test of choice for assessing the progress of the inflammatory process in the post-therapy monitoring of patients. FDG-PET is therefore an additional diagnostic tool that can be of considerable help in atypical or TAB-negative forms of Horton’s disease, shortening diagnostic and therapeutic timescales [11].
The prognosis for CAG is generally good. Some studies report a slight excess of mortality compared with the general population, but this does not appear to be the case in France.
Deaths from cardiovascular causes may be more frequent, both at diagnosis and after several years. For the moment, no reliable marker or factor is known to determine the vital prognosis of a person with CAG. The disease or its treatment may also lead to sequelae.
Conclusion
This observation once again highlights the contribution of PET, particularly for the diagnosis of atypical forms of GCA in the absence of diagnostic criteria suggestive of the picture: 18FDG PET can reveal arterial hypermetabolism in extracranial localisations of gigantocellular arteritis, without clinical or radiological translation.
References
-
Terrier B, Guillevin L (2014) Vascularites Systemiques. Service de medecine interne, Paris.
-
Alfred MAHRP (2019) Arterite a Cellules Geantes (Horton). Groupe d’Etude Francais des Arterites des gros vaisseaux (GEFA).
-
Belhocinea T, Kayeb O, Delanayec P, Cormanc V, Baghaied M, et al. (2002) Maladie de Horton et atteintes arterielles extratemporales : utilité de la tomographie par émission de positons au 18FDG. A propos de trois observations et d’une revue de la littérature. Revue de Médecine Interne 23, pp: 584-591.
-
Tsetsou S, Michel P, Ribi C, Hirt L, Pasquier RD, et al. (2015) Arterite de Horton: Recommendations lausannoises de prise en charge. Revue medicale Suisse 11(461): 411-417.
-
JCS Joint Working Group (2011) Guideline for management of vasculitis syndrome (JCS 2008) Japanese Circulation Society. Circ J 75(2): 474-503.
-
Pedinielli A, Petrot IK, Fardet L (2012) Une maladie de Horton diagnostiquee grace a la tomographie par emission de positons (TEP). Presse Med 41(12): 1304- 1306
-
Masson C (2010) Rhizomelic pseudopolyarthritis, Horton’s disease. Diagnostic and monitoring criteria. Rheumatism Review Monographs 77(2): 76-81.
-
Ortega HM, Rhodes LA, Tan AL, Tanner SF, Conaghan PG, et al. (2007) Evidence for a different anatomic basis for joint disease localization in polymyalgia rheumatica in comparison with rheumatoid arthritis. Arthritis Rheum 56(10): 3496-3501.
-
Gontier E, Boucheneba S, Cambonb A, Martinc AC, Carmoi T, et al. Pericardite revelant une maladie de Horton : apports de la TEP/TDM au 18F-FDG a propos de deux cas. Presentations affichees Medecine Nucleaire 37: 145-178.
-
Ponge T, Agard C, Barrier JH (1999) Biopsie d’artere temporale. Rev Prat 49: 602-604.
-
Hunder GG (2000) Classification/diagnostic criteria for GCA/PMR. Clin Exp Rheumatol 18: S4-S5.
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO
- Water Management for of Proton Exchange Membrane Fuel Cells Marketing and Sensitive Balance