Cholecystoduodnal Fistula-Gallstones Finds their Way
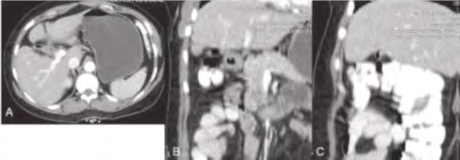
We present a case of 40 year female who was diagnosed with cholelithiasis few years back but was managed conservatively and on CECT after 10 year shows presence of cholecysto-duodnal fistula.
Case Report
A 40 year old female with history of gall stone for 12 years and pain epigastrium for 2 months. She has history of similar complaints few year back in 2009, which was recurrent in nature in particular after taking fatty meals, Got her USG done and was diagnosed with cholelitiasis which was also largely ignored and got relief from injectable pain subsides, and the pain subsided after 3-4 recurrences within in period of 6 months. Again in 2019 she presensented with pain epigastrium but less severe in nature then earlier. CECT was done and images showing fistulous communication between 2nd part of duodenum and gallbladder though not clearly demonstrated, gallbladder is contracted and contains air in its lumen. Features are suggestive of cholecystoduodnal fistula and chronic cholecystitis.
Discussion
Cholecystoduodnal fistula is fistulous communication between gall bladder and duodenum. It is mostly secondary to gallstones which migrate to the duodenum [1, 2]. It may be is some cases iatrogenic in origin, especially after sphincterotomy and after hepaticojejunostomy or choledochojejunostomy [3, 4, 5]. Although patients may be asymptomatic, possible complications include gallstone ileus, Bouveret syndrome or recurrent episodes of cholangitis. It has variable clinical presentation is there, it can be asymptomatic or may present with bouveret syndrome [6].
Enterobiliary fistula was first described by Bartholin in 1654. Sixty-eight per cent of cases occur between the gallbladder wall and duodenum and may cause gallstone ileus and Bouveret syndromes [7]. The key imaging diagnostic clues are
Conclusion
In patients with peptic ulcer disease and history of previous imaging suggesting cholelitihiasis while in present scan having no evidence of gall stones, one must consider the presence of a proximal choledochoduodenal fistula. Patients with recurrent episodes of cholangitis should be investigated for a distal choledochoduodenal fistula. A high index of suspicion is needed from radiologist too for this relatively difficult condition to diagnose [10, 11].
References
-
Stagnitti F, Mongardini M, Schillaci F, Dall’Olio D, Pascalis MD, et al. (2000) Spontaneous biliodigestive fistulae. The clinical consideration, surgical treatment and complications. G Chir 21(3): 110-117.
-
Xeropotamos NS, Nousias VE, Vekris AD, Katsanos KH, Tsianos EV, et al. (2004) Choledochoduodenal fistula: an unusual complication of penetrated duodenal ulcer disease. Ann Gastroenterol 17(1): 104-108.
-
Eliason EL, Stevens LW (1941) Spontaneous internal biliary fistulae. Am J Surg 51(2): 387.
-
Adam A, Dixon AK, Gillard JH, Schaefer-Prokop C, Grainger RG, et al. (2014) Grainger & Allison’s Diagnostic Radiology E-Book. Elsevier Health Sciences.
-
Haaga JR, Boll D Computed Tomography & Magnetic Resonance Imaging of the Whole Body E-Book-003, 180(4): 1033-1035.
-
Kyle J (1958) Choledochoduodenal fistula due to duodenal ulceration. Br J Surg 46(196): 124-127.
-
Hoppenstein JM, Medoza CB, Watne AL (1971) Choledochoduodenal fistula due to perforating duodenal ulcer disease. Ann Surg 173(1): 145-147.
-
Negi RS, Chandra M, Kapur R (2015) Bouveret syndrome: Primary demonstration of cholecystoduodenal fistula on MR and MRCP study. Indian J Radiol Imaging 25(1): 31- 34.
-
Pickhardt PJ, Friedland JA, Hruza DS, Fisher AJ (2003) CT, MR cholangiopancreatography, and endoscopy findings in Bouveret’s syndrome. American Journal of Roentgenology 180(4): 1033-1035.
-
Butler P, Mitchell AW, Ellis H (1999) Applied radiological anatomy. Cambridge University Press.
-
Sutton D (2003) Text Book of Radiology and Imaging. Churchill Livingstone, London, 2: 1453-1487.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO