Role of Peripheral Blood Film in Renal Diseases
Peripheral blood smear examination is a diagnostic tool used in the assessment of various clinical conditions, including kidney diseases. While it is not a primary test for diagnosing kidney diseases, it can provide valuable insights into the presence of anemia, hemolysis, platelet abnormalities, infections, and other systemic changes that can be associated with kidney disorders. It is important to note that peripheral blood smear examination is just one aspect of a comprehensive diagnostic evaluation for kidney diseases and is not a direct method for diagnosing kidney diseases. Other tests, such as blood chemistry, urinalysis, kidney function tests imaging studies (e.g., ultrasound, CT scan), are essential for a complete assessment and accurate diagnosis. In this article, we have stressed on the role of simple and cheap test- peripheral blood film in renal diseases. We have discussed various renal diseases which show different findings on peripheral blood film. All the hematologists, nephrologists and hematopathologists should be aware of these findings.
Introduction
Chronic kidney disease (CKD) is defined by glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2, albuminuria of at least 30 mg per 24 hours, or both persisting for more than 3 months [1]. CKD is estimated to affects 8% to 16% of adult population worldwide [2]. Various causes of kidney disease could be broadly divided into primary renal diseases like Focal segmental glomerulosclerosis (FSGS), C3 glomerulopathy and systemic diseases involving kidney like Diabetic kidney disease (DKD). Evaluation of a patient with suspected renal disease includes detailed clinical examination, investigations including complete blood count, urine analysis, quantification of pro teinuria, kidney function test, estimation of GFR and relevant imaging studies [3]. A peripheral blood film (PBF), also known as a peripheral blood smear, is a simple, fast and cheap laboratory test used to evaluate the different types of blood cells, including red blood cells, white blood cells, and platelets [4]. It can provide helpful information about the underlying pathology of various diseases, including renal diseases. However, it is not typically used as a primary diagnostic tool for renal diseases;
nevertheless, it can provide valuable information when used in conjunction with other diagnostic tests. In renal diseases, the PBF may show abnormalities such as anemia, leukocytosis, or thrombocytopenia, which can aid to suggest the presence of an underlying renal disorder. It can provide helpful information about the underlying pathology of various diseases, including renal diseases. However, it is not typically used as a primary diagnostic tool for renal diseases, however certain findings on PBF, like rouleaux formation, schsitiocytes etc. suggest an underlying etiology of renal disease. These findings guide for further investigations like serum protein electrophoresis (SPEP), serum complement levels, kidney biopsy for definitive diagnosis of renal disease.
Chronic Kidney Disease (CKD)
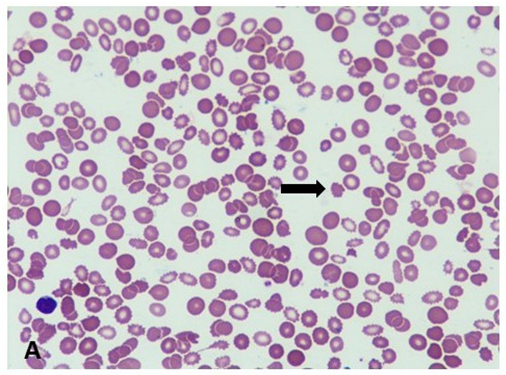
In patients with CKD anemia could be multifactorial and associated with poor outcome [5]. Anemia of renal disease is a common complication of kidney disease. It occurs when the kidneys are unable to produce enough of the hormone erythropoietin (EPO), which stimulates the production of red blood cells in the bone marrow. In healthy individuals, EPO is produced by the kidneys in response to low oxygen levels in the blood. However, in patients with chronic renal disease, the kidneys may not be able to produce enough EPO due to damage to the kidney by low circulating iron concentration and normal iron stores tissues or a decrease in the number of functioning kidney cells. This can lead to a decrease in the production of red blood cells, resulting in anemia [6]. PBF shows normocytic normochromic type of anemia and may also show presence of echinocytes. Also known as “burr cells” or “crenated cells,” echinocytes are a type of red blood cell that has a characteristic spiky or scalloped appearance on their surface (Figure 1). Iron deficiency anemia (IDA) is a common complication of CKD. Iron deficiency anemia could be an absolute deficiency characterized by low iron stores and low circulating iron concentrations or it could be functional deficiency characterized. Hepcidine plays an important role in IDA in CKD [7]. In patients with iron deficiency anemia, PBF examination shows microcytic hypochromic red cells along with elliptocytes, pencil cells and target cells [8]. These findings warrant for further investigation to confirm the diagnosis and initiate iron supplementation.
Hemolytic Uremic Syndrome or Thrombotic Thrombocytopenic Purpura
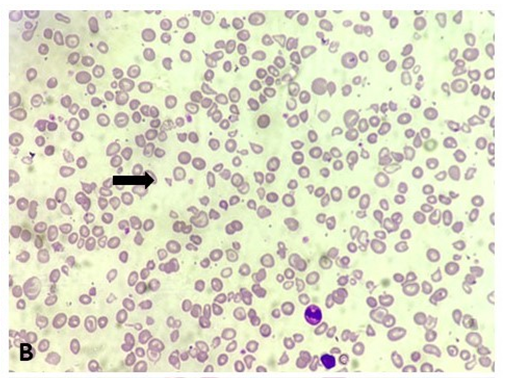
PBF may reveal several abnormalities, the most striking of which is the presence of schistocytes (also known as helmet cells or keratocytes). The intact red cells sustain mechanical damage as a result of being entrapped within the fibrin threads of the microthrombi that form inside the blood vessels, resulting in formation of these fragmented cells [9]. Schistocytes are irregular, fragmented red blood cells with sharp, pointed edges (Figure 2). It indicates the presence of microangiopathic hemolytic anemia due to mechanical shearing. In addition to schistocytes, the PBF may also reveal other signs of hemolysis, such as polychromasia and increased reticulocyte count (immature red blood cells). Thrombocytopenia may also be seen on the PBF, with a reduced number of platelets and the presence of small platelets, indicating platelet destruction. In an appropriate clinical setting of renal dysfunction, with or without hematuria and renal biopsy findings of glomerular and vascular thrombotic microangiopathy (TMA) suggest alternative pathway (AP) abnormalities. Genetic analysis of genes involved in pathogenesis of AP will confirm the diagnosis [10].
Renal Diseases Associated with Plasma Cell Dyscrasias, Amyloidoses, Waldenstrom Macroglobulinemia, and Cryoglobulinemic Nephropathies
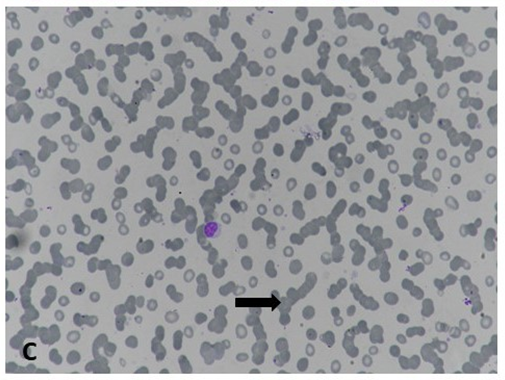
Plasma cell dyscrasias is associated with variety renal lesions including light chain cast nephropathy, light chain amyloidosis, monoclonal immunoglobulin deposition disease (MIDD), and rare lesions like proliferative glomerulonephritis with monoclonal deposits, light chain tubulopathy and TMA [11]. PBF may show abnormalities in the appearance of the blood cells, such as rouleaux formation, which is a stacking of red blood cells that resembles a stack of coins, and hyperviscosity, which is an increase in the thickness or stickiness of the blood along with bluish background staining on PBF as a result of paraproteinemia (Figure 3) [12]. 3 Circulating plasma cells in PBF are markers of highly proliferative disease and indicates poor outcome in cases of multiple myeloma [13]. PBF may also show the presence of cryoglobulins, which appear as clumps or aggregates of protein in the blood. However, the presence of cryoglobulins on PBF is not specific to cryoglobulinemia and can be seen in other conditions as well. Any of these PBF findings coupled with renal dysfunction and/or proteinuria warrants evaluation of an underlying paraproteinemia.
Sickle Cell Nephropathy
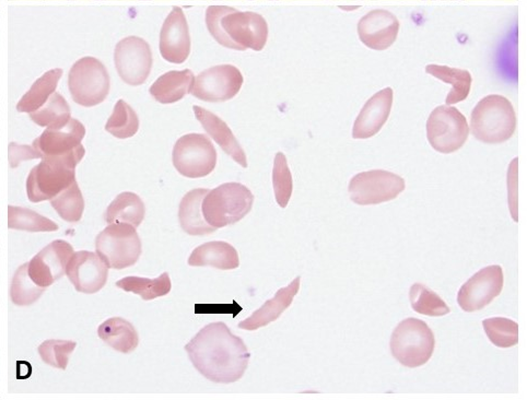
PBF may show the characteristic sickle-shaped red blood cells (crescent/banana shaped) or boat shaped cells, as well as other changes in the blood cells, such as increased white blood cell count and platelet count and other signs of hemolysis [14]. These changes are due to the underlying sickle cell disease and the associated inflammation and tissue damage that occur in the kidneys and other organs. The presence of sickle-shaped red blood cells in the PBF can also indicate the presence of sickle cell trait or sickle cell disease in individuals who may not have been previously diagnosed (Figure 4). Therefore, PBF may be useful in the initial screening of individuals with suspected sickle cell disease or in the follow-up monitoring of individuals with sickle cell disease who are at risk for kidney complications. These patients are more susceptible to develop renal medullary carcinoma [15].
Infections
Infections like microfilariasis and malaria can affect kidneys and can be diagnosed on PBF. Renal microfilariasis may show evidence of anemia/eosinophilia along with present of the parasite [16]. Renal damage occurs in about 40% of Plasmodium falciparum infections in which glomeruli, tubules or interstitium can be involved [17]. Patients affected with Plasmodium may show evidence of anemia and presence of malarial parasite on PBF in form of trophozoite, gametocyte, schizont or ring forms. PBF also helps in identifying the species of malarial parasite and thus to initiate appropriate antimalarial drug. Timely diagnosis and supportive therapy for AKI improves the survival and recovery of kidney function in these patients [18].
Leukemia’s/Lymphomas
Renal involvement of hematolymphoid malignancies is well described. Kidney diseases associated with hematolymphoid malignancies are due direct effect of disease process or due toxicity of chemotherapy. Spectrum of kidney disorders includes AKI, tumour lysis syndrome, electrolyte imbalance, direct infiltration of renal parenchyma, paraneoplastic glomerulopathies and rarely chemotherapeutic drug induced TMA [19, 20]. The neoplasms included non-Hodgkin lymphoma, chronic lymphocytic leukemia, acute lymphoblastic leukemia, Burkitt’s lymphoma, intravascular lymphoma, Hodgkin lymphoma and chronic myeloid leukemia [8, 9]. PBF evaluation is a well- established cost-effective and quick screening for any of these malignancies. In addition to providing the morphological clues, it can pave a way for a directed approach for further confirmatory tests (Flow cytometry panel, FISH or molecular genetics analysis).
Lupus Nephritis
The most frequent hematological manifestations for Lupus nephritis are presence of leucopenia (lymphopenia and granulocytopenia) and thrombocytopenia.10 Immune thrombocytopenic purpura (ITP) could be one of the manifestations of SLE [21]. In SLE patients thrombocytopenia is associated with presence of antiphospholipid antibodies [22]. In these settings PBF helps to distinguish true thrombocytopenia from pseudothrombocytopenia. Anemia can be as anemia of chronic disease (Normocytic normochromic) and autoimmune hemolytic anemia (Macrocytes, spherocytes, reticulocytosis) as well as in the form of microangiopathic hemolytic anemia (schistocytes). Many of these patients can also present with pancytopenia which can be readily identified and confirmed with a PBF evaluation [23].
To sum up, while the PBF is not a primary diagnostic tool for renal diseases, it can provide valuable information that can assist in the diagnosis and management of these conditions. However, the interpretation of the PBF results should always be done in conjunction with other clinical and laboratory findings. It can be used as part of a comprehensive diagnostic workup and can help guide further evaluation and management of patients with renal diseases.
References
-
(2013) Definition and classification of CKD. Kidney Int Suppl 3(1): 19-62.
-
Jha V, Garcia-Garcia G, Iseki K, Li Z, Naicker S, et al. (2013) Chronic kidney disease: global dimension and perspectives. The Lancet 382(9888): 260-272.
-
Davenport A (2020) Clinical investigation of renal disease. In: Firth J, et al. (Eds.), Oxford Textbook of Medicine. 6th (Edn.), Oxford University Press, pp: 4781-C21.4.F20.
-
Adewoyin AS, Nwogoh B (2014) Peripheral blood film - a review. Ann Ib Postgrad Med 12(2): 71-79.
-
Kovesdy CP, Trivedi BK, Kalantar-Zadeh K, Anderson JE (2006) Association of anemia with outcomes in men with moderate and severe chronic kidney disease. Kidney 69(3): 560-564.
-
Shaikh H, Hashmi MF, Aeddula NR (2023) Anemia of Chronic Renal Disease. StatPearls Publishing, Treasure Island.
-
Gutiérrez OM (2021) Treatment of Iron Deficiency Anemia in CKD and End-Stage Kidney Disease. Kidney Int Rep 6(9): 2261-2269.
-
Fletcher A, Forbes A, Svenson N, Thomas DW (2021) Guideline for the laboratory diagnosis of iron deficiency in adults (excluding pregnancy) and children. Br J Haematol 196(3): 523-529.
-
Boyer O, Niaudet P (2022) Hemolytic-Uremic Syndrome in Children. Pediatr Clin North Am 69(6): 1181-1197.
-
Angioi A, Fervenza FC, Sethi S, Zhang Y, Smith RJ, et al. (2016) Diagnosis of complement alternative pathway disorders. Kidney 89(2): 278-288.
-
Lin M, Haas M (2017) Paraprotein-associated thrombotic microangiopathy: expanding the spectrum of renal disease related to plasma cell dyscrasias. Kidney Int 91(3): 532-534.
-
Zhang Y, Pan J, Kang H, Peng S, Tung TH, et al. (2023) Characteristics of inpatients with newly diagnosed multiple myeloma in hematology, nephrology, and orthopedic departments. Ann Hematol 102(4): 801-809.
-
Granell M, Calvo X, Garcia-Guiñón A, Escoda L, Abella E, et al. (2017) Prognostic impact of circulating plasma cells in patients with multiple myeloma: implications for plasma cell leukemia definition. Haematologica 102(6): 1099-1104.
-
Aeddula NR, Bardhan M, Baradhi KM (2023) Sickle Cell Nephropathy. StatPearls Publishing, Treasure Island.
-
Holland P, Merrimen J, Pringle C, Wood LA (2020) Renal Medullary Carcinoma and Its Association with Sickle Cell Trait: A Case Report and Literature Review. Curr Oncol 27(1): 53-56.
-
Agarwal K, Gaur K, Khasim N (2021) Filariasis presenting with bicytopenia, progressive splenomegaly and acute renal failure: An unusual case report. Trop Doct 51(4): 588-590.
-
Junior GBDS, Pinto JR, Barros EJG, Farias GMN, Daher EDF (2017) Kidney involvement in malaria: an update. Rev Inst Med Trop São 59.
-
Kute V, Munjappa B, Patel H, Engineer D, Vanikar A, et al. (2012) Outcome and prognostic factors of malaria- associated acute kidney injury requiring hemodialysis: A single center experience. Indian J Nephrol 22(1): 33.
-
Ganguli A, Sawinski D, Berns JS (2015) Kidney diseases associated with haematological cancers. Nat Rev Nephrol 11(8): 478-490.
-
Chatzikonstantinou T, Gavriilaki M, Anagnostopoulos A, Gavriilaki E (2020) An Update in Drug-Induced Thrombotic Microangiopathy. Front Med 7: 212.
-
Fayyaz A, Igoe A, Kurien BT, Danda D, James JA, et al. (2015) Haematological manifestations of lupus. Lupus Sci Med 2(1): e000078.
-
Abu-Shakra M, Gladman DD, Urowitz MB, Farewell V (1995) Anticardiolipin antibodies in systemic lupus erythematosus: Clinical and laboratory correlations. Am J Med 99(6): 624-628.
-
Bashal F (2013) Hematological Disorders in Patients with Systemic Lupus Erythematosus. Open Rheumatol J 7(1): 87-95.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat