Prenatal Diagnoses of Congenital CNS Anomalies
Background: Congenital anomalies affecting the central nervous system are among the most prevalent. The most common central nervous system anomalies are neural tube defects, which affect roughly 1-2 of every 1000 newborns. Objectives: We detect the accuracy of ultrasound to diagnose CNS abnormalities. Patients and Methods: Descriptive cross-sectional study on 567 patients coming for antenatal care at Sohag Governorate undergoing mid anatomical scan between September 2021 and December 2022. After getting approval from the ethical committee at Sohag University and written consent from each woman. Clinical or post-natal neuroimaging using computed tomography or magnetic resonance imaging validated the prenatal diagnosis in situations where pregnancy progressed and the fetus survived. The total number of miscarriages, stillbirths, and infant deaths was recorded. Results: Diagnostic accuracy of ultrasound in diagnosis of congenital neurological anomalies: 2D&3D US had 100% sensitivity and 100% specificity with positive predictive value 100% and negative predictive value 100% in all parameters. Conclusions: Based on these findings, we can say that ultrasonography is useful for detecting and diagnosing some defects of the fetal central nervous system.
Introduction
The central nervous system (CNS) is composed of the brain and the spinal cord. They both develop from the embryonic ectoderm alongside other structures like the skin. Their development begins as early as the 3rd and 4th weeks of embryonic life, starting with the process of neurulation, which is the development of the neural tube. The neural tube closes spontaneously rostrally and caudally. In the fifth to sixth week, the first appearance of the brain, the prosencephalic development ensues. The primitive brain is comprised of prosencephalon, mesencephalon, and rhombencephalon. The prosencephalon divides further into telencephalon and diencephalon through a series of developmental stages, namely: formation, cleavage, and development of the midline [1, 2, 3]. Any form of developmental alteration in these leads to the malformation of the developing brain [4].
Fetal central nervous system (CNS) abnormalities are second only to cardiac malformations in their frequency of occurrence. Early and accurate diagnosis at prenatal US is therefore essential, allowing improved prenatal counseling and facilitating appropriate referral [5]. Central nervous system (CNS) malformations are some of the most common of all congenital abnormalities. Neural tube defects are the most frequent CNS malformations to about 1–2 cases per 1000 births [6].
Prenatal detection and accurate definition of CNS malformations are important because these anomalies frequently have a severe prognosis and are often associated with genetic syndromes [7]. The development of the brain and spinal cord is an extremely complicated process which continues into the second decade before final maturity is achieved. Abnormality in the development of CNS is common, up to 75% of fetal deaths and 40% of deaths in infancy are due to CNS malformations [7]
Fetal neurological abnormalities are six main categories at prenatal US. Developmental anomalies include neural tube defects and neuronal migration disorders. Posterior fossa disorders include Dandy-Walker malformation variants and Chiari II malformation. Ventricular anomalies include aqueductal stenosis. Midline disorders include those on the spectrum of holoprosencephaly, agenesis of the corpus callosum, and septo-optic dysplasia. Vascular anomalies include veins of Galen malformations. Miscellaneous disorders include hydranencephaly, porencephaly, tumors, and intracranial hemorrhage [5].
Aim of the Work
We detect the accuracy of ultrasound to diagnose CNS abnormalities with postnatal conformation.
Patients and Methods
This descriptive cross-sectional study was carried out on 569 patients coming for antenatal care at Sohag Governorate undergoing mid anatomical scan from September 2021 to December 2022 after approval from the ethical committee at Sohag University and obtaining a written consent from each woman.
Criteria of Patient Selection
Inclusion Criteria: Pregnant women have mid-anatomical scan at 20-22 weeks.
Methods
All patients were subjected to the followings:
- Complete history was taken from patient’s age body mass index (BMI), consanguinity, maternal history, and family history.
- General examination.
- Radiological investigations:
- Two-dimensional Ultrasound (US) was performed to detect the presence of antenatal anomalies.
Two-Dimensional Ultrasound Technique
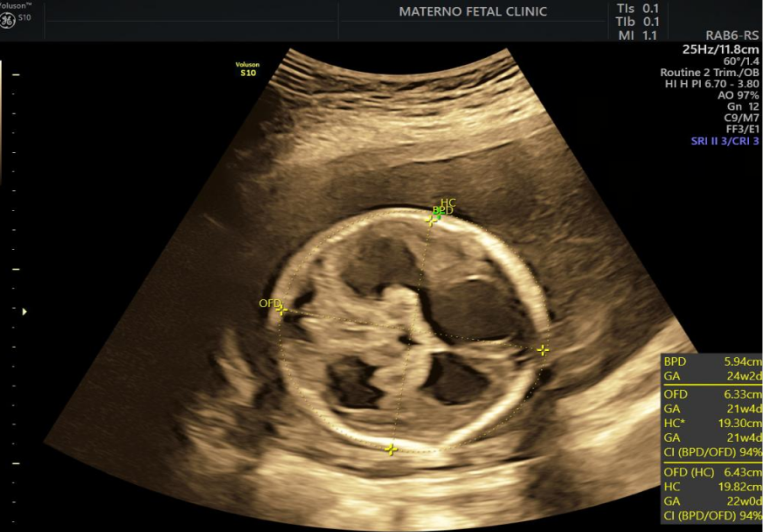
Antenatal examination of the anomalies was done for all pregnant women using two-dimensional US (The Voluson E8 color Doppler US diagnostic instrument) during the second trimester. First, the abdominal convex array probe C1-5-D was adopted, and the probe frequency was set to 2.0 MHz. The lower abdomen was scanned for the presence of any anomalies [8]. Four standard recommended views- trans ventricular, falx, cavum, and posterior fossa or trans cerebellar views-provide an overview of fetal intracranial anatomy during the second trimester anatomy scan.
Fetal Outcome and Follow Up
All of the newborns in the research had a postnatal checkup and confirmation of the defects by a pediatric expert to ascertain their individual health. Clinical or post-natal neuroimaging using computed tomography or magnetic resonance imaging validated the prenatal diagnosis in situations where pregnancy progressed and the fetus survived. The total number of miscarriages, stillbirths, and infant deaths was recorded.
Statistical Analysis
SPSS v26 was used for the statistical analysis (IBM Inc., Chicago, IL, USA). The average and standard deviation of numerical variables were provided (SD). Percentages and frequencies were used to illustrate qualitative factors (percent).
Results
This study was a descriptive cross-sectional study conducted on 567 pregnant women coming for antenatal care at Sohag governorate undergo mid anatomical scan. The age ranged from 16 to 48 years with a mean value (± SD) of 29.72 (±5.97) years. BMI ranged from 19 to 41 kg/m2 with a mean value (± SD) of 28.92 (±4.06) kg/m2. Consanguinity was present in 44 (7.76%) patients and not in 523 (92.24%) patients (Table1, Figure1).
| N=567 | ||
|---|---|---|
| Age (years) | Mean ± SD | 29.7 ± 5.97 |
| Age (years) | Range | 16 - 48 |
| BMI (kg/m2) | Mean ± SD | 28.9 ± 4.06 |
| BMI (kg/m2) | Range | 19 - 41 |
| Consanguinity | Yes | 44 (7.76%) |
| Consanguinity | No | 523 (92.24%) |
Table 1: Demographic data of the studied mothers.
Maternal medical history was negative in 50 (87.72%) patients and positive 7 (12.28%) patients. Positive maternal medical history was Positive TOURCH infection in 5 (8.77%) patients, teratogenic drugs in 1 (1.75%) patient and brain atrophy in 1 (1.75%) patient (Table 2, Figure 2).
| N=57 | ||
|---|---|---|
| Maternal Medical History | Negative | 50 (87.72%) |
| Maternal Medical History | Positive | 7(12.28%) |
| Maternal Medical History | Positive TOURCH infection | 5 (8.77%) |
| Maternal Medical History | Positive teratogenic drugs | 1 (1.75%) |
| Maternal Medical History | Brain atrophy | 1 (1.75%) |
Table 3: Maternal medical history of the studied patients with neurological anomalies.
Family history was negative in 37 (64.91%) patients and positive in 20(35.09%) patients. Positive congenital in other siblings in 9 (15.79%) patients, microcephaly, epilepsy, hydrocephalus, Deafness, CHD and hydrocephalus in 1 (1.75%) patient and Brain atrophy in 6 (10.53%) patients (Table3, Figure3).
| N=57 | ||
|---|---|---|
| Family History | Negative | 37 (64.91%) |
| Family History | Positive | 20(35.09%) |
| Family History | Positive congenital in other siblings | 9 (15.79%) |
| Family History | Microcephaly | 1 (1.75%) |
| Family History | Brain atrophy | 6 (10.53%) |
| Family History | Epilepsy | 1 (1.75%) |
| Family History | Hydrocephalus | 1 (1.75%) |
| Family History | Deafness, CHD | 1 (1.75%) |
| Family History | Hydrocephalus | 1 (1.75%) |
Table 2: Family history of the studied patients.
CHD: Congenital heart disease Table 3: Family history of the studied patients.
Prevalence of neurological congenital anomalies in sohag governorate.
Mid anatomical scans were performed on 567 pregnant women neurological who presented for antenatal scan in the Sohag governorate. It was noticed that (90% n=510) females in the current study had not congenital anomalies in her baby and (10% n=57) had neurological congenital anomalies in her baby findings as shown in Figure 4, so the prevalence of neurological congenital anomalies detected by ultrasound in Sohag governorate was 10%.
Antenatal diagnosis showed microcephaly in 8 (14.04%) patients, Microcephaly, hepatosplenomegaly in 2 (3.51%) patients, Dandy-walker syndrome in 7 (12.28%) patients, Joubert syndrome in 2 (3.51%) patients, Hydrocephalus in 16 (28.07%) patients, Hydrocephalous, CHD, Biventricular dilation hydrocephalus, Holoprosencephaly, hydrocephalus, Hydrocephalus aqueductal stenosis, Holoprosencephaly, cleft lip and palate, Intracranial calcification IUGR, Occipital encephalocele meningomyelocele, Left cerebral hemisphere atrophy, Left ventriculomegaly agenesis of corpus callosum, Retrocerebellar dermoid cyst, Spina bifida, middle cerebral artery aneurysm and intracranial hemorrhage in 1 (1.75%) patient, corpus callosum agenesis in 4 (7.02%) patients, anencephaly in 3 (5.26%) patients and vein of Galen aneurysm in 2 (3.51%) patients (Table 4).
| Antenatal Diagnosis | Microcephaly | 8 (14.04%) |
| Antenatal Diagnosis | Microcephaly, hepatosplenomegaly | 2 (3.51%) |
| Antenatal Diagnosis | Dandy-walker syndrome | 7 (12.28%) |
| Antenatal Diagnosis | Joubert syndrome | 2 (3.51%) |
| Antenatal Diagnosis | Hydrocephalus | 16 (28.07%) |
| Antenatal Diagnosis | Hydrocephalous, CHD | 1 (1.75%) |
| Antenatal Diagnosis | Biventricular dilation hydrocephalus | 1 (1.75%) |
| Antenatal Diagnosis | Holoprosencephaly, hydrocephalus | 1 (1.75%) |
| Antenatal Diagnosis | Hydrocephalus aqueductal stenosis | 1 (1.75%) |
| Antenatal Diagnosis | Holoprosencephaly, cleft lip and palate | 1 (1.75%) |
| Antenatal Diagnosis | Intracranial calcification IUGR | 1 (1.75%) |
| Antenatal Diagnosis | Occipital encephalocele meningomyelocele | 1 (1.75%) |
| Antenatal Diagnosis | Left cerebral hemisphere atrophy | 1 (1.75%) |
| Antenatal Diagnosis | Left ventriculomegaly agenesis of corpus callosum | 1 (1.75%) |
| Antenatal Diagnosis | Retrocerebellar dermoid cyst | 1 (1.75%) |
| Antenatal Diagnosis | Corpus callosum agenesis | 4 (7.02%) |
| Antenatal Diagnosis | Spina bifida | 1 (1.75%) |
| Antenatal Diagnosis | Anencephaly | 3 (5.26%) |
| Vein of Galen aneurysm | 2 (3.51%) | |
|---|---|---|
| Middle cerebral artery aneurysm | 1 (1.75%) | |
| Intracranial hemorrhage | 1 (1.75%) | |
Table 4: Antenatal diagnosis of the studied patients.
CHD: Congenital heart disease. Table 4: Antenatal diagnosis of the studied patients.
Postnatal confirmation was Clinically in 19 (33.33%) patients, Hydrocephalus markedly dilated ventricles ambiguous genitalia in 1 (1.75%) patient, Clinically meningitis 1st day, hydrocephalus in 1 (1.75%) patient, CT confirmation in 6 (10.53%) patients, - Brain atrophy, Dandy-walker syndrome (hydrocephalus CT), Hydrocephalus, HIE, CT non communicating hydrocephalus, CT communicating hydrocephalus, hypogenesis corpus callosum VSD, CT molar tooth, mild brain atrophy, CT semi lobar holoprosencephaly, Butterfly vertebra and Clinically, CT markedly dilated ventricular system decreased brain volume in 1 (1.75%) patient, MRI Confirmation in 11 (19.3%) patients, MRI brain atrophy, Biventricular dilation hydrocephalus MRI diffuse brain atrophy, MRI multi cystic brain encephalomalacia at 5th month of age, MRI mild hypoplastic corpus callosum, dilated ventricles PVL, MRI Left ventriculomegaly, MRI confirmation, inter hemisphere cyst and MRI, squint in 1 (1.75%) patient (Table 5).
| Postnatal confirmation | Positive | Negative | |||
|---|---|---|---|---|---|
| Clinically | 19 (33.33%) | Positive | Negative | ||
| Clinically | 19 (33.33%) | Positive | Negative | ||
| Hydrocephalus markedly dilated ventricles ambiguous genitalia | 1 (1.75%) | 57 | 0 | ||
| Clinically meningitis 1st day, hydrocephalus | 1 (1.75%) | 0 | 510 | ||
| CT confirmation | 6 (10.53%) | ||||
| Brain atrophy | 1 (1.75%) | ||||
| Dandy-walker syndrome (hydrocephalus CT) | 1 (1.75%) | ||||
| Hydrocephalus, HIE | 1 (1.75%) | ||||
| CT non communicating hydrocephalus. | 1 (1.75%) | ||||
| CT communicating hydrocephalus, hypogenesis corpus callosum VSD. | 1 (1.75%) | ||||
| CT molar tooth, mild brain atrophy | 1 (1.75%) | ||||
| CT semi lobar holoprosencephaly | 1 (1.75%) | ||||
| Butterfly vertebra | 1 (1.75%) | ||||
| Clinically, CT markedly dilated ventricular system decreased brain volume | 1 (1.75%) | ||||
| MRI Confirmation | 11 (19.3%) | ||||
| MRI brain atrophy | 1 (1.75%) | ||||
| Biventricular dilation hydrocephalus MRI diffuse brain atrophy | 1 (1.75%) | ||||
| MRI multi cystic brain encephalomalacia at 5th month of age | 1 (1.75%) | ||||
| MRI mild hypoplastic corpus callosum, dilated ventricles PVL | 1 (1.75%) | ||||
| MRI Left ventriculomegaly. | 1 (1.75%) | ||||
| MRI confirmation, inter hemisphere cyst. | 1 (1.75%) | ||||
| MRI, squint | 1 (1.75%) |
Table 6: Postnatal confirmation of the studied patients.
In our study, 57 cases of neurological Mal formation detected by ultrasound and all were confirmed postnatally either clinically or by radiological imaging CT or MRI.
Diagnostic accuracy of ultrasound in diagnosis of congenital neurological anomalies: 2D&3D US had 100% sensitivity and 100% specificity with positive predictive value 100% and negative predictive value 100% in all parameters (Table 6, Figure 5-10).
| Postnatal confirmation | ||||
|---|---|---|---|---|
| Clinically | 19 (33.33%) | Positive | Negative | |
| Clinically | 19 (33.33%) | Positive | 57 | 0 |
| Hydrocephalus markedly dilated ventricles ambiguous genitalia | 1 (1.75%) | Negative | 0 | 510 |
Table 5: Diagnostic accuracy of ultrasound in diagnosis of congenital neurological anomalies.




Antenatal diagnosis showed microcephaly in 8 (14.04%) patients, Microcephaly, hepatosplenomegaly in 2 (3.51%) patients, Dandy-walker syndrome in 7 (12.28%) patients, Joubert syndrome in 2 (3.51%) patients, Hydrocephalus in 16 (28.07%) patients, Hydrocephalous, CHD, Biventricular dilation hydrocephalus, Holoprosencephaly, hydrocephalus, Hydrocephalus aqueductal stenosis, Holoprosencephaly, cleft lip and palate, Intracranial calcification IUGR, Occipital encephalocele meningomyelocele, Left cerebral hemisphere atrophy, Left ventriculomegaly agenesis of corpus callosum, Retrocerebellar dermoid cyst, Spina bifida, middle cerebral artery aneurysm and intracranial hemorrhage in 1 (1.75%) patient, corpus callosum agenesis in 4 (7.02%) patients, anencephaly in 3 (5.26%) patients and vein of Galen aneurysm in 2 (3.51%) patients. (Table 5) The United States is able to evaluate and diagnose central nervous system malformations in the fetus at any stage of pregnancy. The ultrasound examination also covers the spinal cord and brain. Since the majority of brain development occurs during pregnancy, understanding whether the elements of the central nervous system exhibit complex embryology and architecture is crucial. During pregnancy, there are alterations in the CNS that are correlated with alterations in the US parts of the CNS [9]. The embryology and architecture of the CNS, as well as its ultrasonography properties at different gestational ages, must be understood by all professionals engaged in prenatal examination to prevent misdiagnosis. In addition, knowing the following about the congenital defects that might impact the central nervous system is crucial [9]. Evaluation of the fetal central nervous system during ultrasonography is typically done in the axial, sagittal, and coronal planes using abdominal and vaginal methods in the first trimester. Examination of fetal morphology during 20–24 weeks of gestation is when most attempts to identify CNS abnormalities are made [10]. Since the brain is a three-dimensional organ with a complex anatomy, the midline structures such as the corpus callosum, brain stem, cerebellar vermis, and cerebral cortex are probably not evaluated if the scan of the fetal skull is performed just in the axial planes [6]. Multiplaner study of the embryonic brain regions using sagittal and coronal images of the fetal skull was reported by Tritsch, et al. [11] (Timor- Tritsch and Monteagudo, 1996). The ultrasonographic examination of the brain and spine in fetuses is governed by two sets of recommendations produced by ISUOG, titled “basic CNS assessment” and “neurosonographic evaluation” [10].
The aim of our work was to detect the accuracy of ultrasound to diagnose CNS abnormalities with postnatal confirmation. This was a descriptive cross-sectional study conducted on 567 pregnant women coming for antenatal care at Sohag governorate undergo mid anatomical scan. In our study, the age ranged from 16 to 48 years with a mean value (± SD) of 29.72 (±5.97) years. BMI ranged from 19 to 41 kg/m2 with a mean value (± SD) of 28.92 (±4.06) kg/m2. In our study, maternal medical history was negative in 50 (87.72%) patients and positive 7 (12.28%) patients. Positive maternal medical history was Positive TORCH infection in 5 (8.77%) patients, teratogenic drugs in 1 (1.75%) patient and brain atrophy in 1 (1.75%) patient.
According to Munim, et al. [12] who aimed to describe the trends of congenital abnormalities seen at a tertiary care facility in Karachi. They reported that the mean age of the women in this study was 27.3 years with SD ± 5.3. Among the study subjects 11.6% were women above the age of 35 years. Only 8.8% of them had a previous history of congenital malformations.
Patients visiting the fetomaternal center at Minia University were surveyed to determine the prevalence of central nervous system abnormalities [9]. It was shown that 25% of patients had a history of other congenital fetal abnormalities and 6% had a history of other central nervous system fetal. In our study, antenatal diagnosis showed microcephaly in 8 (14.04%) patients, , hepatosplenomegaly in 2 (3.51%) patients, Dandy-walker syndrome in 7 (12.28%) patients, Joubert syndrome in 2 (3.51%) patients, Hydrocephalus in 16 (28.07%) patients, Hydrocephalous, CHD, Biventricular dilation hydrocephalus, Holoprosencephaly, hydrocephalus, Hydrocephalus aqueductal stenosis, Holoprosencephaly, cleft lip and palate, Intracranial calcification IUGR, Occipital encephalocele meningomyelocele, Left cerebral hemisphere atrophy, Left ventriculomegaly agenesis of corpus callosum, Retrocerebellar dermoid cyst, Spina bifida, middle cerebral artery aneurysm and intracranial hemorrhage in 1 (1.75%) patient, corpus callosum agenesis in 4 (7.02%) patients, anencephaly in 3 (5.26%) patients and vein of Galen aneurysm in 2 (3.51%) patients.
Hassan, et al. [9] we learn that ultrasonography may identify CNS defects in 79 fetuses. Ventriculomegaly was the most often seen abnormality (22%). Due to the continuous process of brain development, modest ventriculomegaly may still be considered a normal variant. The high rate of Ventriculomegaly in our sample (42% of cases) may be explained by the fact that enlargement of the lateral ventricle has been documented in fetuses with aneuploidy during the first trimester. Ultrasound examination is operator dependent and requires thorough and skilled examination since it sometimes involves trial and error. Sixty-four percent of the instances in which a diagnosis of CNS abnormalities was verified after birth, compared with 19 percent of the cases in which therapeutic termination of pregnancy was used. According to a study conducted by Fatma, et al. [13], the identification rate of CNS abnormalities using ultrasonography was 90%. They found that prenatal detection of CNS abnormalities occurred in 90% of patients.
When considering whether or not to terminate a pregnancy, ultrasound diagnosis of prenatal brain anatomic abnormalities is crucial. Patients are more likely to agree to this approach since it is non-invasive. Multiple studies have shown that the United States is able to identify brain abnormalities with a sensitivity of 92% to 99.7% [14]. In our study Diagnostic accuracy of ultrasound in diagnosis of congenital neurological anomalies: 2D&3D US had 100% sensitivity and 100% specificity with positive predictive value 100% and negative predictive value 100% in all parameters.
Ultrasound has been shown to have a 90% detection rate for neural tube abnormalities in a case-control study [15].
For the diagnosis of congenital anomalies, the research team at Gonçalves, et al. [16] found that MRI was more sensitive than 3D -US (MRI, 88.9 percent (16/18) vs. 3DUS, 66.7 percent (12/18) vs. 2D-US, 72.2 percent (13/18)), and that it also provided additional information affecting prognosis. The diagnostic accuracy of 2D-US, 3D-US, and MRI for non- CNS abnormalities was comparable. The sensitivity of MRI was 85.6 percent (77/90) whereas the sensitivity of 3D-US was 94.4 percent (85/90) and the sensitivity of 2D-US was 92.2 percent (83/90). While 2D-US and 3D-US were more reliable than MRI for ruling out CNS disorders before birth, confirmation of these findings after delivery was not possible for MRI.
Conclusion
Based on these findings, we can say that Diagnostic accuracy of ultrasound in diagnosis of congenital neurological anomalies: 2D&3D US had 100% sensitivity and 100% specificity. Our results also imply that imaging tools like CT and MRI scans are effective for confirming diagnoses of neurological and developmental abnormalities in babies, even if clinical assessment is a crucial tool in making the initial diagnosis.
References
-
Gaitanis J, Tarui T (2018) Nervous System Malformations. Continuum (Minneap Minn). Child Neurology 24(1): 72- 95.
-
Dias M, Partington M (2015) Congenital Brain and Spinal Cord Malformations and Their Associated Cutaneous Markers. Pediatrics 136(4): 1105-1119.
-
Petryk A, Graf D, Marcucio R (2007) Holoprosencephaly: signaling interactions between the brain and the face, the environment and the genes, and the phenotypic variability in animal models and humans. Wiley Interdiscip Rev Dev Biol.Sonographic examination of the fetal central nervous system: guidelines for performing the ‘basic examination’ and the ‘fetal neurosonogram’. Ultrasound Obstet Gynecol 29(1): 109-116.
-
Marin-Valencia I, Guerrini R, Gleeson JG (2014) Pathogenetic mechanisms of focal cortical dysplasia. Epilepsia 55(7): 970-978.
-
Cater SW, Boyd BK, Ghate SV (2020) Abnormalities of the Fetal Central Nervous System: Prenatal US Diagnosis with Postnatal Correlation. Radiographics 40(5): 1458- 1472.
-
Malinger G, Lev D, Lerman-Sagie T (2006) Normal and abnormal fetal brain development during the third trimester as demonstrated by neurosonography. Eur J Radiol 57(2): 226-232.
-
Rizzo G, Abuhamad AZ, Benacerraf BR, Chaoui R, Corral E, et al. (2011) Collaborative study on 3-dimensional sonography for the prenatal diagnosis of central nervous system defects. J Ultrasound Med 30(7): 1003-1008.
-
Pang B, Pan JJ, Li Q, Zhang X (2007) Accuracy of ultrasonography in diagnosis of fetal central nervous system malformation. World J Clin ination of the fetal brain UOG 30(7): 1019-1032.
-
Hassan HH, Mohamed MA, Elgibaly FAZR (2022) Proportion of Central Nervous System Fetal Malformations in patients attending Fetomaternal Unit Minia University as an observation study. Minia Journal of Medical Research 33(2): 137-145.
-
ISUOG (2007) Sonographic examination of the fetal central nervous system: guidelines for performing the ‘basic examination’ and the ‘fetal neurosonogram’. Ultrasound Obstet Gynecol 29(1): 109-116.
-
Timor-Tritsch IE, Monteagudo A (1996) Transvaginal fetal neurosonography: standardization of the planes and sections by anatomic landmarks. Ultrasound Obstet Gynecol 8(1): 42-47.
-
Munim S, Nadeem S, Khuwaja NA (2006) The accuracy of ultrasound in the diagnosis of congenital abnormalities. J Pak Med Assoc 56(1): 16-18.
-
El-Dein MFS, Hamid WRA, Elsayed ABB (2019) Role of 3D/4D Ultrasound in Assessment of Fetal CNS Congenital Anomalies. Nat Sci 17(11): 154-157.
-
Abozaid KA, Aborashed AA, Mohamad MT (2022) Role of 3d and 4d dimensional ultrasonography in detection of fetal brain anomalies in second trimester of pregnancy. Al-Azhar International Medical Journal 3(11): 141-147.
-
Gupta SG, Singh H (2001) Prenatal Diagnosis Of Neural Tube Defects. Med J Armed Forces India 57(2): 126-128.
-
Gonçalves LF, Lee W, Mody S, Shetty A, Sangi-Haghpeykar H, et al. (2016) Diagnostic accuracy of ultrasonography and magnetic resonance imaging for the detection of fetal anomalies: a blinded case-control study. Ultrasound Obstet Gynecol 48(2): 185-192.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat