Anatomical Study of the Origin, Course, and Branches of the Anterior Interosseous Nerve
Introduction: The anterior interosseous nerve (AIN) is the main branch originating from the median nerve, responsible for innervating muscles in the anterior compartment of the forearm. It follows a route along the ventral surface of the interosseous membrane, sending branches to the flexor pollicis longus (FPL) and flexor digitorum profundus (FDP) until reaching the pronator quadratus (PQ) muscle. Understanding its origin, path, and ramifications is crucial for clinical and surgical purposes, especially in cases of pronator teres syndrome, AIN compression, carpal tunnel syndrome, and nerve transfers. Objective: This study aims to describe the origin, trajectory, and types of termination of the anterior interosseous nerve up to its arrival at the pronator quadratus muscle. Material and Methods: Dissections were conducted on 52 AINs from 26 human fetuses (13 male and 13 female). Measurements of the AIN were taken using a precision digital caliper, and schematic drawings were used to analyze its trajectory and branches. Results: The length of the AIN varied from 19.05 to 59.83 mm with an average of 39.85 mm and could be classified according to the origin based on the exit face from the MN, exit number, and the relationship with the biepicondylar line. Regarding their path and branching pattern, they were classified into three types: Type I, where the AIN trifurcation occurs into branches for the FPL, PQ, and FDP; Type II, where the branch is emitted to the FDP and a common trunk is formed for the PQ and FPL branches; and Type III, where the branch is emitted to the FPL and a common trunk is formed for the PQ branches and FDP. These types may have extra branches, other branches for different muscles, and branches for joints. Conclusion: The importance of understanding the AIN is evident, based on the recognition of its variant possibilities in the forearm to enhance the clinical and surgical management of the issues associated with this nerve.
Abbreviations
AIN: The Anterior Interosseous Nerve; FPL: Flexor Pollicis Longus; FDP: Flexor Digitorum Profundus PQ: Pronator Quadratus.
Introduction
The main branch of the median nerve in the forearm is the anterior interosseous nerve (AIN), which innervates most of the deep layer muscles of the anterior compartment of the forearm [1, 2]. It is essentially a motor nerve [3] for the flexor pollicis longus (FPL), flexor digitorum profundus (FDP), index, middle, and pronator quadratus (PQ) muscles [4]. Its path is anterior to the interosseous membrane, reaching the posterior surface of the pronator quadratus, perforating it, branching, and innervating this muscle [5]. It has also been suggested that the AIN can provide sensory innervation to the capsules of the radiocarpal, intercarpal, carpometacarpal, and radioulnar joints [6]. From a clinical-surgical point of view, AIN syndrome is a rare form of peripheral neuropathy, with an occurrence of less than 1% among all upper limb nerve syndromes [7]. In general, it presents with a prodrome of pain in the arm and/or forearm lasting hours or days [8], which is followed by paralysis of the muscles innervated by the nerve [9]. Therefore, a good knowledge of the anatomical distribution of the AIN in the region can be of great help in the treatment of this nerve syndrome [10].
Another injury situation may be related to the impact of compressions of the median nerve [11]. AIN injuries commonly appear involved as part of brachial plexus injuries, supracondylar humerus fracture, and Parsonage-Turner syndrome [12, 13, 14]. Other causes are also reported, including trauma, iatrogenesis during surgery, use of slings, and dressings [15]. Furthermore, vigilance is needed regarding the possible development of AIN syndrome in patients with coronavirus disease [16]. The diagnosis of these lesions is established through nerve conduction studies and electromyography of the pronator quadratus muscle. The AIN is also a common donor site for the ulnar nerve or the median nerve, where a good clinical outcome occurs in the practice of nerve transfer with improvement of pathological conditions [17, 18, 19, 20].
Therefore, it is important to anatomically study the topography, the variability of the origin of the AIN, and identify the branching pattern to seek to understand the causes of nerve compression syndromes, for the planning of surgical approach [21], as well as knowing the surgical milestones such as the biepicondylar line, pronator teres, and Gantzer muscle [22]. Our objective was to describe the origin, trajectory, and types of termination of the AIN until its arrival at the pronator quadratus muscle. For this, the intention was to carry out an incremental approach focusing on the analysis of several elements of the origin of the AIN, such as exit position, face, distance in relation to the biepicondylar line, observation of the entire path of the AIN on the forearm, and how it emits its branches. In this way, this work contributes to the existing knowledge in the literature and helps professionals improve management of the region.
Materials and Methods
The anatomical study was conducted through the dissection of 52 AIN in the forearms of 26 human fetuses from the Anatomy Laboratory of the Morphology Department at the Federal University of Sergipe, comprising 13 males and 13 females. Forearms with abnormalities or damage that could affect nerve analysis were excluded from the study, thus only well-preserved forearms were used to prevent nerve damage. Research with fetuses offers advantages such as easier dissection and accessibility of material. Furthermore, the results obtained from fetal studies can be extrapolated to adults.
Dissection was performed until the median nerve and all its articular branches were isolated (Figure 1). AIN was completely dissected and its origin, course, and types of terminations up to the innervation of the pronator quadratus muscle were exposed (Figure 2). Regarding the origin, it was analyzed which branch represented the exit from the AIN, in comparison with the articular branches of the median nerve, the output of this nerve in relation to the median nerve and finally the distance from its exit in relation to the biepicondylar line. The path and branching characteristics of the AIN were illustrated in schematic drawings to enhance visualization and categorize the nerve’s paths and its terminations.
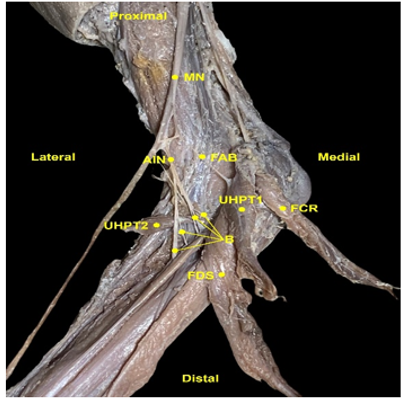
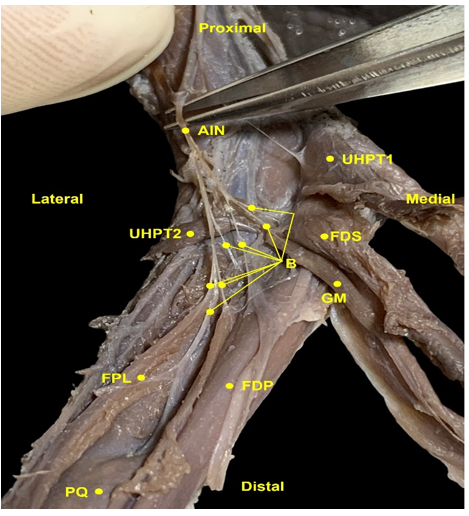
Figure 2: Anterior Interosseous Nerve (AIN) with its branches. AIN - Anterior Interosseous Nerve; UHPT1- Umeral Head of Pronator Teres; UHPT2 - Ulnar Head of Pronator Teres; FDS - Flexor Digitorum Superficialis; B - Branches of the anterior interosseous nerve; GM - Gantzer Muscle; FPL - Flexor Pollicis Longus; FDP - Flexor Digitorum Profundus; PQ - Pronator quadratus.
A digital caliper with an accuracy of 0.01 mm was used to obtain measurements related to the AIN, such as the distance from the origin to the bipicondylar line and nerve length. Additionally, the fetal age was calculated by measuring the hallux-calcaneal length, using the formula derived from studies by Goldstein, Reece, Hobbins [23]. The results indicated a fetal age range between 23.3 and 36.8 weeks, with an average of 30.15 weeks. The fetuses were obtained in compliance with Law No. 8,501 of 1992, which governs the use of unclaimed corpses for studies and research. This study was approved by the Research Ethics Committee of the Federal University of Sergipe under hearing number 5.275.543 and followed the ethical guidelines established by the Declaration of Helsinki.
Results
The AIN was found bilaterally in all dissected fetuses, from the first articular branch of the median nerve to the fifth. The distribution of branches was as follows: 11.5% had the AIN as the first branch (6); 19.2% had it as the second and fourth branch (10); 42.3% had it as the third branch (22), which had the highest incidence; and 7.8% had it as the fifth branch (4). The AIN presented three variations in terms of its exit face from the MN: exit from the posteromedial face in 3.8% of cases (2); exit from the posterolateral surface in 15.4% of cases (8); and exit from the posterior face in 80.8% of cases (42), which was the highest incidence. The point of emergence of the AIN in relation to the biepicondylar line occurred in three ways: above the line in 36.5% of cases (19); at the line level in 9.5% of cases (5); and below the line in 54% of cases (28). The highest frequency of origin was below the biepicondylar line, with the greatest distance above the line being 18.29 mm, and after the line, the greatest distance was 9.17 mm. The AIN had a maximum length of 59.83 mm and a minimum length of 19.05 mm, with an average length of 39.85 mm.
The path and branching pattern of the AIN were classified into three types: Type I, where the trifurcation of the AIN occurred into branches for the FPL, PQ, and FDP (Figure 3); Type II, with the emission of a branch to the FDP and the formation of a common trunk for the PQ and FPL branches (Figure 4); and Type III, with the emission of a branch to the FPL and the formation of a common trunk for the branches of the PQ and FDP (Figure 5). The most lateral branch was the one that went to the FPL, the most medial was the one that reached the FDP, while the PQ branch was in an intermediate position to the other branches.
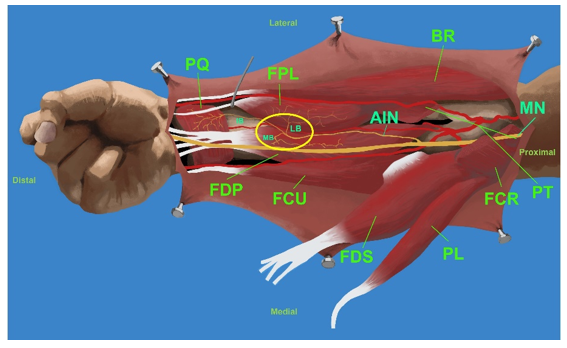
Figure 3: Type I: trifurcation of the AIN into branches for FPL, PQ, and FDP. AIN = Anterior Interosseous Nerve; MN = Median Nerve; MB = Medial Branch to the FDP; IB = Intermediate Branch for PQ; LB = Lateral Branch to the FPL; PQ = Pronator Quadratus; FPL = Flexor Pollicis Longus; FDP = Flexor Digitorum Profundus; FCU = Flexor Carpi Ulnaris; FDS = Flexor Digitorum Superficialis; PL = Palmaris Longus; FCR = Flexor Carpi Radialis; PT = Pronator Teres; BR = Brachioradialis.
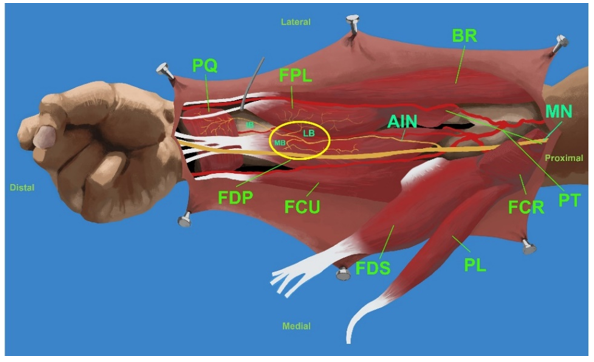
Figure 4: Type II: emission of the branch to the FDP and formation of a common trunk for the PQ and FPL branches. AIN = Anterior Interosseous Nerve; MN = Median Nerve; MB = Medial Branch to the FPD; IB = Intermediate Branch for PQ; LB = Lateral Branch to the FPL; PQ = Pronator Quadratus; FPL = Flexor Pollicis Longus; FDP = Flexor Digitorum Profundus; FCU = Flexor Carpi Ulnaris; FDS = Flexor Digitorum Superficialis; PL = Palmaris Longus; FCR = Flexor Carpi Radialis; PT = Pronator Teres; BR = Brachioradialis.
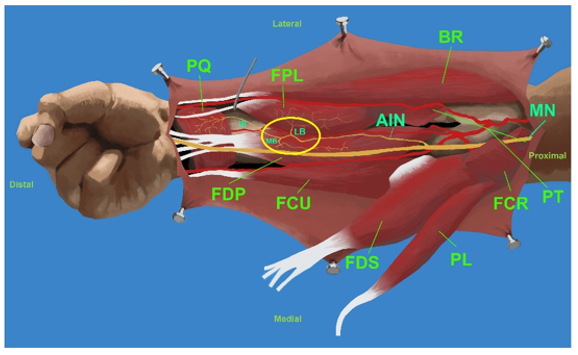
Figure 5. Type III: emission of the branch to the FPL and formation of a common trunk for the PQ and FDP branches. AIN = Anterior Interosseous Nerve; MN = Median Nerve; MB = Medial Branch to the FDP; IB = Intermediate Branch for PQ; LB = Lateral Branch to the FPL; PQ = Pronator Quadratus; FPL = Flexor Pollicis Longus; FDP = Flexor Digitorum Profundus; FCU = Flexor Carpi Ulnaris; FDS = Flexor Digitorum Superficialis; PL = Palmaris Longus; FCR = Flexor Carpi Radialis; PT = Pronator Teres; BR = Brachioradialis.
Discussion
In the present study, it was found that the AIN innervates the FDP, FPL, and PQ muscles in a classical manner. It is also important to highlight the potential contribution of the AIN to the innervation of other muscles in the region, such as the flexor digitorum superficialis muscle, flexor carpi radialis muscle, and Gantzer’s muscle. The literature reports variable presence of Gantzer’s muscle, considered an accessory head of the FPL or FDP [11]. Some authors consider Gantzer’s muscle a vulnerable point of compression for the AIN [24]. In our dissections, its occurrence was approximately 35%. These relationships are important for recognizing AIN injuries and understanding potential branching patterns of this nerve, which could enhance comprehension of compression points.
It was often possible to observe several extra branches for the FPL and FDP muscles. This could indicate that they could be used as a source of graft and nerve transfer in cases of upper extremity nerve palsy [22]. Branches that entered and followed the trajectory of the interosseous membrane were also identified. Some authors suggest that they may be capsular sensory branches for the radioulnar joint regions [6]. There are different descriptions of the point of origin and course of the AIN, as well as the communicating branches of the nerve with other nerves in the forearm [1]. These descriptions were observed, and different possibilities of the origin of the AIN were presented. It was also noted that the different possibilities of origin not only occurred from the emergence of the MN distal to the medial epicondyle after passing deep to the pronator teres and the arch of the flexor digitorum superficialis [8], but also occurred at the level of the biepicondylar line or even more proximally. Additionally, in some cases, communicating branches of the AIN with other branches of the same nerve or with branches of the MN were present.
The anterior interosseous nerve branch to the PQ is increasingly used as a donor nerve for end-to-end and reverse end-to-side nerve transfers. The anatomy of the PQ (and its nervous branch) is generally considered reliable in the absence of previous trauma [17]. This is because this branch has a very constant anatomy. The emission of branches was observed only in its proximal portion, but along the way, it maintains a very invariable characterization, making it an excellent target for these practices. In cases of transfers due to ulnar nerve neuropathy, knowledge of the anatomy of the AIN is of great importance for surgical techniques. However, many inadequate descriptions exist, with inconsistent use of anatomical terms and insufficient detail on the main components of the procedure [25].
Limitations of the study should be acknowledged. The classification relies on various morphological features, and the optimal sample size was not determined. Further research with larger and more diverse samples is necessary to validate the proposed classification system. Moreover, other studies can delve into the classification of branches, including subtypes and variations in innervation of the AIN. Correlations and variations of the AIN based on factors such as sex and side can also be investigated. Nevertheless, this study is unique in its technique approach in human fetuses. No age-related changes were observed in the nerve path.
Conclusion
It is important to understand the anatomy of the AIN, considering the potential variations in the forearm in terms of its origin, trajectory, and ramifications. This understanding can enhance clinical and surgical outcomes, leading to better management of issues related to this nerve, such as AIN syndrome recognition, nerve transfer surgeries, pronator teres syndrome, carpal injuries, traumatic injuries, and the prevention of iatrogenic injuries.
Funding
None.
Research Ethics Committee Approval
The study was approved by the Research Ethics Committee of the Federal University of Sergipe under hearing number 5.275.543 and CAAE: 55188421.2.0000.5546. The study followed the ethical guidelines established by the Declaration of Helsinki.
Acknowledgments
The authors wish to sincerely thank those who donated their bodies to science so that anatomical research could be carried out. The results of this research can potentially im-prove patient care and increase the overall knowledge of humanity. Therefore, these donors and their families deserve our utmost gratitude.
Conflicts of Interest
None.
References
-
Riveros A, Olave E, Sousa-Rodrigues C (2018) Previous Interosseous Nerve: Course, Distribution and Clinical Implications. Int J Morphol 36(3): 1079-1086.
-
Jeon A, Lee M, Kim DW, Kwon OY, Lee JH (2022) Anatomical study of the anterior interosseous nerve. Folia Morphol (Warsz) 81(3): 574-578.
-
Ulrich D, Piatkowski A, Pallua N (2011) Anterior interosseous nerve syndrome: retrospective analysis of 14 patients. Arch Orthop Trauma Surg 131(11): 1561- 1565.
-
Rodner CM, Tinsley BA, O’Malley MP (2013) Pronator syndrome and anterior interosseous nerve syndrome. J Am Acad Orthop Surg 21(5): 268-275.
-
Sakamoto K, Nasu H, Nimura A, Hamada J, Akita K (2015) An anatomic study of the structure and innervation of the pronator quadratus muscle. Anat Sci Int 90(2): 82- 88.
-
Patterson JMJ, Novak CB, Mackinnon SE (2010) Compression Neuropathies. In: Green’s Operative Hand Surgery. Elsevier, Philadelphia, 28: 1085-1126.
-
Li N, Russo K, Rando L, Gulotta-Parrish L, Sherman W, et al. (2022) Anterior Interosseous Nerve Syndrome. Orthop Rev (Pavia) 14(4): 38678.
-
Krishnan KR, Sneag DB, Feinberg JH, Wolfe SW (2020) Anterior Interosseous Nerve Syndrome Reconsidered: A Critical Analysis Review. JBJS Rev 8(9): e2000011.
-
Mills RH, Mukherjee K, Bassett IB (1969) Anterior interosseous nerve palsy. Br Med J 2(5656): 555.
-
Alves N, Cândido PL, Frazão R (2004) Innervation of the pronator quadratus muscle. Int J Morphol 22(4): 253- 256.
-
Caetano EB, Vieira LA, Sprovieri FAA, Petta GC, Nakasone MT, et al. (2017) Anatomical variations of pronator teres muscle: predispositional role for nerve entrapment. Revista Brasileira de Ortopedia 52(2): 169-175.
-
Mauricio EA, Rubin DI (2019) Inclusion Body Myositis Mimicking Bilateral Anterior Interosseous Neuropathies. J Hand Surg Am 44(12): 1100.e1-1100.e4.
-
Shinohara T, Takahashi S, Hirata H (2017) Anterior interosseous nerve palsy mimicking rupture of the index flexor digitorum profundus after volar locking plate fixation of a distal radius fracture. Nagoya J Med Sci 79(3): 421-425.
-
Iyer VG, Shields LB, Zhang YP, Shields CB (2023) Clinical Spectrum of Postsurgical Parsonage-Turner Syndrome: A Perspective From an Electrodiagnostic Laboratory. Cureus 15(6): e41001.
-
Nammour M, Desai B, Warren M, Sisco-Wise L (2021) Anterior Interosseous Nerve Palsy After Shoulder Arthroscopy Treated With Surgical Decompression: A Case Series and Systematic Review of the Literature. Hand (N Y) 16(2): 201-209.
-
Ikumi A, Yoshii Y, Nagashima K, Takeuchi Y, Tatsumura M, et al. (2023) Anterior interosseous nerve syndrome following infection with COVID-19: a case report. J Med Case Rep 17(1): 253.
-
Dy CJ, Brogan DM, Colorado BS (2019) Absence of the Pronator Quadratus Muscle Precluding Distal Nerve Transfer. J Hand Surg Am 44(6): 523.e1-523.e5.
-
Dunn JC, Gonzalez GA, Fernandez I, Orr JD, Polfer EM, et al. (2021) Supercharge End-to-Side Nerve Transfer: Systematic Review. Hand (NY) 16(2): 151-156.
-
Head LK, Zhang ZZ, Hicks K, Wolff G, Boyd KU (2020) Evaluation of Intrinsic Hand Musculature Reinnervation following Supercharge End-to-Side Anterior Interosseous-to-Ulnar Motor Nerve Transfer. Plast Reconstr Surg 146(1): 128-132.
-
Tanure AA, Rezende LGRA, Pazim AC, Ribeiro ML (2022) Supercharged End-to-Side Anterior Interosseous to Ulnar Motor Nerve Transfer for Hirayama Disease: A Case Report. Hand (NY) 17(4): NP12-NP16.
-
Rao YL, Pai MM, Krishnaprasad PR, Murlimanju BV, Mamatha T, et al. (2021) Exploring the Morphology of Anterior Interosseous Nerve and Relating It to Its Clinical Conditions. Turk Neurosurg 31(1): 107-111.
-
Ankolekar VH, Hosapatna M, Dsouza A (2021) Locating the anterior interosseous nerve in relation to the surgically relevant landmarks of the forearm: A cadaveric study. Ann Med Surg (Lond) 71: 102930.
-
Goldstein I, Reece EA, Hobbins JC (1988) Sonographic appearance of the fetal heel ossification centers and foot length measurements provide independent markers for gestational age estimation. Am J Obstet Gynecol 159(4): 923-926.
-
Degreef I, Smet LD (2004) Anterior interosseous nerve paralysis due to Gantzer’s muscle. Acta Orthop Belg 70(5): 482-484.
-
Kulenkampff C, Duraku LS, George S, Power D (2023) Supercharged End-to-Side Nerve Transfer for Ulnar Neuropathy: Redefining Nomenclature and Recommendations for Standardisation of Surgical Technique Description. Cureus 15(11): e48660.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat