Antifungal Susceptibility Pattern of Fungi Associated with Tinea capitis in School Children of Morogoro Municipality, Tanzania
Introduction: Tinea capitis is one of the common skin diseases affecting school-age children in developing countries. However, the susceptibility of fungi associated with this disease against antifungal agents commonly used has not been fully investigated. Aim: The aim of this study was to determine the antifungal susceptibility pattern of fungi associated with tinea capitis amongst children sampled from selected schools in Morogoro Municipality, Tanzania. Methods: A descriptive cross-sectional study was conducted involving 72 school children recruited from 10 primary schools in selected class strata within Morogoro Municipality, Tanzania using a multistage sampling technique. Pure cultures of fungi isolates were obtained from scrappings of head lesions in school children and tested for sensitivity to commonly used antifungal agents using the Kirby Bauer agar disk diffusion method. Results: The identified fungi were Trichoderma longibrachiatum, Cytobasidium minutum, Aspergillus spp, Ectophoma multirostrata, Aureobasidium pullulans, Aspergillus flavus, Cladosporium tenuissimum, Pichia terricola, Penicillium flavigenum and Fusarium solani. Out of 10 fungal isolates, 9 (90%) were sensitive to both amphotericin B and nystatin, 4(40%) sensitive to clotrimazole, 1(10%) sensitive to fluconazole and griseofulvin, 3(30%) sensitive to itraconazole, and no isolate showed sensitivity to ketoconazole. Nystatin and amphotericin B showed best antifungal activity against Trichoderma longibrachiatum, Cytobasidium minutum, Fusarium solani and Aspergillus sp while clotrimazole and ketoconazole had intermediate fungal growth inhibition and best activity against Fusarium solani and Aspergillus sp but were resistant to the other antifungal agents. Fluconazole, griseofulvin, and itraconazole were not effective to any of the isolates. Conclusion: This study revealed that nystatin and amphotericin B were ideal antifungal drugs for the treatment of tinea capitis in the studied population.
Introduction
Tinea capitis is a superficial fungal infection of the scalp, eyebrows and eyelashes, with a propensity for attacking hair shafts and follicles [1]. Tinea capitis is sometimes known as ringworm of the scalp, it is not really a worm but a fungal infection whereby the fungus makes circular marks on the scalp and especially flat centers and raised borders. It is the most common dermatophytosis in children aged between six months, prepubertal age and prevalent in adults whose immunity has been suppressed [2, 3, 4]. The two most common dermatophytes responsible for tinea capitis infection are Trichophyton tonsurans and Microsporum canis [5]. Tinea capitis remains a common childhood infection in many parts of the world [6]. The distribution is attributed by factors such as climate, population migration patterns, lifestyle, primary host range, secondary host immunity, presence of immunodeficiency diseases, and patient’s attitude to prompt treatment following clinical presentation and standard of living [7]. Tinea capitis is quite common in Africa with prevalence among children ranging between 14 and 86% [7]. In developing countries in Eastern Africa, it is categorized as a disease of poverty due to poor socio economic status, high population densities and poor hygienic conditions these factors are responsible for high prevalence of tinea capitis [8, 9]. In Tanzania, large city such as Dar-es-Salaam the prevalence of dermatophytosis was found to be 11% of 420 primary school children [10].
Currently, tinea capitis treatment options include both topical and oral agents including antifungal drugs such as clotrimazole, miconazole, nystatin, terbinafine, itraconazole, griseofulvin and fluconazole [11, 12]. Recently, due to increase in the reports of antifungal drug resistance in dermatophytes, it has been suggested by number of studies to perform the antifungal drug susceptibility testing. Antifungal susceptibility testing will help in understanding the epidemiological pattern of drug resistance in a particular region, choosing the most efficacious antifungal agents for standard treatment and the antifungal susceptibility data will help in effective management. Several studies have been conducted in Tanzania to determine the prevalence and burden of fungal infection [13, 14]. There is paucity of data regarding antifungal susceptibility of fungi associated with tinea capitis or invitro drug resistance to dermatophytes whereas some infections respond well to topical antifungal therapy, others like tinea capitis may require systemic therapy [15]. In some cases, therapy is not effective because of resistance to the drugs by the fungi. Therefore, with the increasing variety of drugs to treat dermatophytes on the market, the need for testing of antifungal susceptibility of dermatophytes has become apparent [16]. To our knowledge, there are few studies on prevalence, antifungal testing and treatment practice of tinea capitis in different parts of Tanzania. There are no reports on epidemiologic studies and antifungal testing on tinea capitis among school children in Morogoro Municipality, Tanzania.
In this study, the agar disk diffusion method which is standardized, simple and reproducible was used to determine the in vitro antifungal susceptibility of denmatophytes associated with tinea capitis [17, 18]. The findings of this study will allow the clinician to apply the appropriate therapy for the management of infections caused by dermatophytes for school children in Tanzania.
Materials and Methods
Study Design and Setting
The present study was a descriptive cross-sectional study involving primary school children with clinical presentation suggestive of fungal infections of the head, including ring scalp, baldness and alopecia. Swabs and scrapings were taken from the head lesions and placed into sterile containers and transported to the laboratory at Sokoine University of Agriculture (SUA) for isolation and identification.
Sample Collection
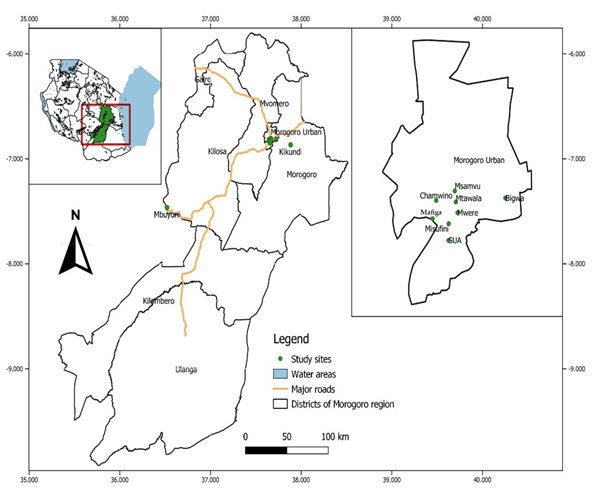
A multistage sampling technique was used to select school children from different primary schools and class strata. A total of 72 school children with clinical signs suggestive of tinea capitis infection were recruited from 10 primary schools; namely Misufini, Mafiga, Msamvu, SUA, Kikundi, Chamwino, Mtawala, Bigwa, Mwere and Mbuyuni (Figure 1). School children aged between 6 and 14 years from classes 1, 3, 5 and 7 were enrolled into the study after obtaining a written consent from parents/guardians. Lesions were physically examined in broad daylight and then skin scrapping’s were taken from the head lesions using a sterile scalpel blade and placed into a sterile container.
Isolation of Tinea capitis
Sabouraud dextrose agar (SDA) (Sigma Aldrich, St. Louis, USA) was prepared according to the instruction of the manufacturer’s. Briefly, cool sterilized medium was mixed with skin scrapping’s and poured into 150 mm sterile cell culture dishes (Corning Incorporated, Corning, NY). The dishes were then allowed to solidify and incubated at room temperature (about 25oC) for three days and the ensuing colonies sub-cultured in in 9 mm diameter SDA Petri dishes (MLS, Menen, Belgium). Fungal colonies were passaged four times to obtain pure cultures.
Antifungal Sensitivity Test
Fungi sensitivity to ketoconazole (15 µg), nystatin (50 µg), fluconazole (25 µg), clotrimazole (10 µg), griseofulvin (25 µg) and amphotericin B (10 µg) (Rosco, Taastrup, Denmark) was performed using the agar diffusion method. A total of 32.5 g SDA powder was mixed with 500 ml of distilled water, allowed to dissolve and then autoclaved at 121°C for
15 minutes. The fungi were suspended in 10 ml of warm agar in sterile tubes, homogenized and then poured into petri dishes and allowed to solidify, before placing the antifungal onto the surface of the agar. The plates were then incubated at room temperature for seven days and the diameter of zone of inhibition measured using a mm ruler to appreciate the sensitivity of each fungal isolate to the antifungal agents. Interpretation of antifungal susceptibility (susceptible S, intermediate I and resistant R) was based on CLSI standards [17, 19, 20] (Table 1).
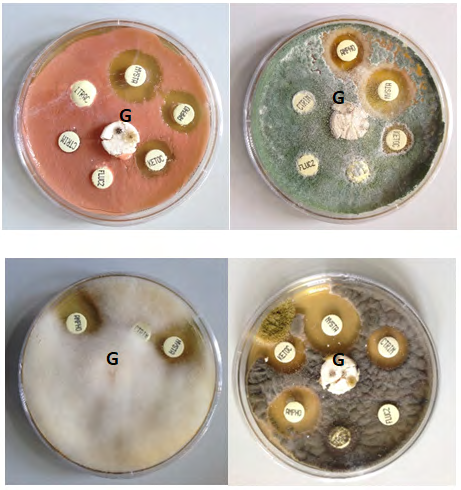
Antifungal susceptibility of isolates associated with tinea capitis in school children after incubation with antifungal agents including amphotericin B (AMPHO), clotrimazole (CTRIM), fluconazole (FLUCZ), itraconazole (ITRAC), griseofulvin (GRISE), ketoconazole (KETOC) and nystatin (NYSTA). The zone of growth inhibition was measured in mm.
Ethical considerations
The purposes and benefits of the study were explained to the school children, parents/guardians and teachers. Informed written consent from the parents/guardians of the study subjects was sought before recruitment into the study. Ethical clearance was obtained from the National Health Research Committee of the Tanzania National Institute for Medical Research, certificate number NIMR/HQ/R.8a/Vol. IX/1943.
Results
Antifungal Susceptibility
A total of 72 school children were recruited as study subjects, 12 (16.67%) had tinea capitis. Identification of fungal isolates by morphological and molecular techniques in related studies by Macha, et al. [21] had indicated the following fungi to be associated with tinea capitis: Trichoderma longibrachiatum, Cytobasidium minutum. Aspergillus spp, Ectophoma multirostrata, Aureobasidium pullulans, Pichia terricola, Aspergillus flavus, Cladosporium tenuissimum, Penicillium flavigenum and Fusarium solani. Interpretation of antifungal susceptibility (susceptible S, intermediate I and resistant R) was based on Clinical Laboratory Standard Institute (CLSI) standards (Table 1) and the antifungal susceptibility of these fungi is shown in Table 2.
| Antifungal drugs | Potency | Zone diameter in mm | ||
|---|---|---|---|---|
| Sensitive | Intermediate | Resistant | ||
| Amphotericin B | 10 µg | >15 | 10-14 | <9 |
| Clotrimazole | 10 µg | ≥20 | 19-12 | ≤11 |
| Fluconazole | 25 µg | ≥19 | 15-18 | ≤14 |
| Griseofulvin | 25 µg | ≥10 | - | No zone |
| Itraconazole | 10 µg | >15 | 10-14 | ≤9 |
| Ketoconazole | 15 µg | ≥30 | 29-23 | ≤22 |
| Nystatin | 50 µg | ≥15 | 10-14 | ≤10 |
Table 1: Criteria of susceptibility and resistance of antifungal disks.
| Antifungal sensitivity (Ø in mm) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Fungal isolate | BLASTn | Accession number | AMPHO | CTRIM | FLUCZ | GRISE | ITRAC | KETOC | NYSTA |
| MSU03 | Aspergillus sp | MN700638 | 21 | 24 | 20 | 0 | 17 | 25 | 32 |
| MSU03 | Ectophoma multirostrata | MN700639 | 17 | 20 | 0 | 0 | 0 | 0 | 15 |
| MSU04 | Fusarium solani | MN700640 | 17 | 16 | 10 | 0 | 12 | 13 | 24 |
| MSU06 | Pichia terricola | MN700642 | 0 | 0 | 0 | 0 | 0 | 14 | 10 |
| KIK02 | Trichoderma longibrachiatum | MN700636 | 16 | 15 | 0 | 0 | 18 | 18 | 28 |
| KIK04 | Cytobasidium minutum | MN700637 | 20 | 10 | 0 | 0 | 0 | 17 | 25 |
| KIK06 | Cladosporium tenuissimum | MN700643 | 18 | 29 | 0 | 20 | 16 | 0 | 20 |
| KIK06 | Aspergillus flavus | MN700645 | 16 | 15 | 0 | 0 | 0 | 12 | 13 |
| CHA 03 | Penicillium flavigenum | MN700644 | 20 | 0 | 0 | 0 | 0 | 0 | 28 |
| SUA 07 | Aureobasidium pullulans | MN700641 | 29 | 20 | 0 | 0 | 0 | 20 | 34 |
Table 2: Antifungal susceptibility of fungi isolates Macha, et al. [21].
Primary schools: KIK= Kikundi, MSU= Msufini, CHA= Chamwino Number 0 representing resistance to the antifungal. Antifungal agents: Amphotericin B (AMPHO), clotrimazole (CTRIM), fluconazole (FLUCZ), itraconazole (ITRAC), griseofulvin (GRISE), ketoconazole (KETOC) and nystatin (NYSTA).
Antifungal Susceptibility of Fungi Isolated from Tinea capitis
Pure cultures of the fungi were tested for sensitivity to different antifungal agents including: amphotericin B, clotrimazole, fluconazole, griseofulvin, itraconazole, ketoconazole and nystatin. The results are shown in Figure 2 and Table 2.
Test results of the susceptibility to antifungal drugs were interpreted as susceptible (S), intermediate (I) or resistant (R) according to CLSI standards (Table 1). Antifungal susceptibility pattern of 10 fungal isolates associated with tinea capitis (Table 3).
| Antifungal | Susceptible (S) n (%) | Intermediate (I) n (%) | Resistant (R) n (%) |
|---|---|---|---|
| Amphotericin B | 9 (90%) | 0 (0%) | 1 (10%) |
| Clotrimazole | 4 (40%) | 4 (40%) | 2 (20%) |
| Fluconazole | 1 (10%) | 0 (0%) | 9 (90%) |
| Griseofulvin | 1 (10%) | 0 (0%) | 9 (90%) |
| Itraconazole | 3 (30%) | 1(10%) | 6 (60%) |
| Ketoconazole | 0 (0%) | 1(10%) | 9 (90%) |
| Nystatin | 9 (90%) | 0 (0%) | 1(10%) |
Table 3: Test results of the susceptibility to antifungal drugs fungal isolates associated with tinea capitis.
Discussion
Tinea capitis is the commonest childhood infection. Given the growing prevalence of tinea capitis in children and immune-compromised adults, it is now regarded as a public health issue worldwide [22]. It is more than a decade since various antifungal drugs with broad effect against the infection have been introduced [23]. These antifungal drugs have been mentioned to have a limited number of cellular targets. This is due to the fact that the mechanisms of action of these drugs overlap one another, hence contributing to the emergence of multidrug resistant phenotypes [24].
In 2008, antifungal susceptibility testing protocol for dermatophytes was approved for the first time by clinical and laboratory standard institute (CLSI), which was further modified in 2010 [25]. The azoles, allylamines, and polyenes represent the most widely used treatments for infection caused by dermatophytes. The azoles are separated into two distinct classes: the imidazoles (eg. clotrimazole, ketoconazole) and triazoles (eg. fluconazole, itraconazole). The triazoles are used as systemic first-line agents for most severe fungal diseases [26]. Different methods can be used to determine the activity of various antifungal drugs against various fungal genera and species. Barry, et al. [27] suggested the standard disk diffusion assay as a good model for antifungal tests in routine laboratory diagnosis and assessment of dermatophyte resistance against antifungal drugs. In this study, the disk diffusion method was used to determine the activities of seven antifungal drugs: Amphotericin B, clotrimazole, fluconazole, griseofulvin, itraconazole, ketoconazole and nystatin against 10 fungi isolates associated with tinea capitis (Trichoderma longibrachiatum, Cytobasidium minutum, Aspergillus spp, Ectophoma multirostrata, Aureobasidium pullulans, Pichia terricola, Aspergillus flavus, Cladosporium tenuissimum, Penicillium flavigenum, and Fusarium solani).
The fungal isolates studied showed 90% sensitivity to amphotericin B and nystatin, 40% sensitivity to clotrimazole, 10% sensitivity to fluconazole and griseofulvin, 30% sensitivity to itraconazole, and all were resistant to ketoconazole. Fungi isolates associated with tinea capitis were found to be sensitive to nystatin and amphotericin B. Nystatin and amphotericin B had large inhibition zones ≥ 15mm around the disks and the best activity against Trichoderma longibrachiatum, Cytobasidium minutum, Aspergillus spp, Ectophoma multirostrata, Aureobasidium pullulans, Pichia terricola Aspergillus flavus, Cladosporium tenuissimum, Penicillium flavigenum, and Fusarium solani.
Few studies have been conducted to determine the antifungal susceptibility pattern of agents of tinea capitis. Some authors have reported a 100% susceptibility of candida species to amphotericin B [20]. This is in agreement with the findings of this study which have shown amphotericin B to be 90% effective against fungal isolates associated with tinea capitis. Interestingly, in this study nystatin which is a polyene antifungal that exerts its effect by targeting the fungal cell membrane via ergosterol binding. Thus causing an increase in cell wall permeability was found to be 90% sensitive to the fungal isolates. This is in agreement with the report of Khan, et al. [19] that it could be used to treat fungal lesions. Our study indicated that most isolates tested were resistant to fluconazole, griseofulvin and ketoconazole (90%), followed by itraconazole (60%), clotrimazole (20%); the least effective was recorded for amphotericin B and nystatin (10%). Clotrimazole and ketoconazole had an intermediate inhibition zone against T. longibrachiatum, F. solani and A. flavus but resistant to C. tenuissimum and others.
Griseofulvin has been reported as an effective and cost-effective drug in the treatment of tinea capitis by a number of studies [17, 28, 29, 30, 31]. According to our study, it was ineffective against 90% of the ten fungal isolates. This is in agreement with Alkeswani, et al. [32] that griseofulvin has been falling out of favor due to significant treatment failure, high cost and long duration of treatment. However, this could be due to species specific differences in response to treatment, mutation, such as missense substitution. This kind of mutation was seen in a dermatophyte T.rubrum which contributes to cross resistance to antifungals [33, 34, 35]. According to a systemic review and a meta-analysis, azoles such as itraconazole and ketoconazole were considered the most effective agents in treating tinea capitis infection caused by Trichophyton spp and Microsporum canis [36, 37, 38]. Despite the fact that they are associated with serious hepatotoxicity and death [39].
They are many studies indicating that fluconazole, itraconazole and ketoconazole has less effect against dermatophytes [31, 40, 41, 42]. Our findings are in agreement with those reports. This could be due to the fact that triazoles have components that can interfere with the test or it could be the culture medium used that is Sabouraud Dextrose Agar components interfere the test [31]. Recently, it was reported that itraconazole should not be considered as a first line agent for cutaneous fungal infections in children, because data on safety and efficacy are lacking [43] and oral ketoconazole has fallen out of favor in many jurisdictions due to risks of hepatotoxicity [39, 44]. Our study, suggests that nystatin and amphotericin B can be used to treating dermatophytosis.
Conclusions and Recommendations
Doctors should be informed on the antifungal drugs that are able to treat dermatophytoses, however optimal regimens for application of antifungal agents need further studies.
Funding
This work was supported by the Government of the United Republic of Tanzania through the Higher Education Student Loan Board (HESLB). The funders had no role in the design of the study, or in the collection, analysis, interpretation of data and writing of the manuscript.
Acknowledgments
This work was supported by the Government of the United Republic of Tanzania through the Higher Education Student Loan Board (HESLB). The authors appreciate the College of Veterinary Medicine and Biomedical Sciences of Sokoine University of Agriculture for granting permission to conduct this research in the Department of Veterinary Microbiology, Parasitology and Biotechnology. The authors are also grateful to individuals who assisted with data collection and critical review of the final drafts of the manuscript.
Author Contributions
M.E.M conceived the study, did the laboratory work, analysed data, and wrote the manuscript. M.R.M helped in laboratory work and G.M supervised M.E.M and critically revised and approved the manuscript.
References
-
Rayala BZ, Morrell DS (2017) Common Skin Conditions in children: Skin Infections. FP Essent 453: 26-32.
-
Mayowa OM, Ana GR, Sridhar MK (2015) Use of Azadirachta indica derived germicidal in the management of tinea capitis among pupils in selected public primary schools in Ibadan, Nigeria. Peak Journal of Medicinal Plant Research 3(1): 9-15.
-
Balci E, Gulgun M, Babacan O, Karaoglu A, Kesik V, _et al_. (2014) Prevalence and risk factors of tinea capitis and tinea pedis in school children in Turkey. J Pak Med Assoc 64(5): 514-518.
-
Hees C, Naafs B, Troderma S (2014) Common Skin Diseases in Africa: An illustrated guide.
-
Shy R, Corporis T, Capitis T (2019) Article skin disorders. 28: 5.
-
Hay RJ (2017) Tinea capitis: Current Status. Mycopathologia 182(1-2): 87-93.
-
Guerrant RL, Walker D, and Peter W (2011) Tropical Infectious Diseases. Principles, Pathogens and Practice, 3rd (edn.), Elsevier Churchill, Livingstone, Philadelphia, Pa, USA.
-
Moto JN, Maingi JM, Nyamache AK (2015) Prevalence of tinea capitis in school-going children from Mathare, informal settlement in Nairobi, Kenya. BMC Res Notes 8: 274.
-
Dinkela A, Ferié J, Mbata M, Grendelmeier MS, Hatz C, _et_ _al_. (2007) Efficacy of triclosan soap against superficial dermatomycoses: a double-blind clinical trial in 224 primary schoolchildren in Kilombero district, Morogoro region, Tanzania. Int J Dermatol 46: 23-28.
-
Komba EV, Mgonda YM (2010) The spectrum of dermatological disorders among primary school children in Dar es Salaam. BMC Public Health 10: 765.
-
Fuller CF, Barton RC, Mustapa MFM, Proudfoot LE, Punjabi SP, _et al_. (2014) British Association of Dermatologists’ guidelines for the management of tinea capitis 2014. Br J Dermatol 171(3): 454-463.
-
Shemer A, Plotnik IB, Davidovici B, Grunwald MH, Magun R, _et al_. (2013) Treatment of tinea capitis - griseofulvin versus fluconazole - a comparative study. J Dtsch Dermatol Ges 11(8): 737-741.
-
Faini D, Maokola W, Furrer H, HatzC, Battegay M, _et al_. (2015) Burden of serious fungal infections in Tanzania. Mycoses 58 (Suppl 5): 70-79.
-
Chikoi R, Nyawale HA, Mghanga FP (2018) Magnitude and Associated Risk Factors of Superficial Skin Fungal Infection Among Primary School Children in Southern Tanzania. Cureus 10(7): 1-12.
-
Esteban A, Abarca ML, Cabanes FJ (2005) Comparison of disk diffusion method and broth microdillution method for antifungal susceptibility testing of dermatophytes. Med Mycol 43(1): 61-66.
-
Augustine SK, Bhavsar SP, Kapadnis BP (2005) Production of a growth dependent metabolite active against dermatophytes by Streptomyces rochei AK 39. Indian J Med Res 121(3): 164-170.
-
Pakshir K, Bahaedinie L, Rezaei Z, Sodaifi M, Zomorodian K (2009) In vitro activity of six antifungal drugs against clinically important dermatophytes. Jundishapur Journal of Microbiology 2(4): 158-163.
-
Torres BF, Carrillo AJ, Martín E, Palacio AD, Moore MK, _et al_. (2001) In vitro activity of ten antifungal drugs against 508 dermatophyte strains. Antimicrob Agents Chemother 45(9): 2524-2528.
-
Khan M, Ahmed J, Gul A, Ikram A, LalaniFK, _et al_. (2018) Antifungal susceptibility testing of vulvovaginal Candida species among women attending antenatal clinic in tertiary care hospitals of Peshawar. Infect Drug Resist 11: 447-456.
-
Seifi Z, Azish M, Salehi Z, Mahmoudabadi AZ, Shamsizadeh A (2013) Candiduria in children and susceptibility patterns of recovered Candida species to antifungal drugs in Ahvaz. J Nephropathol 2(2): 122-128.
-
Macha ME, Makange MR, Misinzo G (2020) Prevalence and identification of fungi associated with tinea capitis in school children of Morogoro municipality, Tanzania. African Journal of Medical and Health Sciences 19(7): 103-109.
-
Gnat S, Łagowski D, Nowakiewicz A (2020) Major challenges and perspectives in the diagnostics and treatment of dermatophyte infections. J Appl Microbiol 129(2): 212-232.
-
Gnat S, Łagowski D, Nowakiewicz A, Dyląg M (2020) Clinically used and potential antimycotics in the context of therapy of dermatomycoses. Postępy Mikrobiol - Adv Microbiol 59: 63-74.
-
Rossi NMM, Bitencourt TA, Peres NTA, Lang EAS, Gomes EV, _et al_. (2018) Dermatophyte resistance to antifungal drugs: Mechanisms and prospectus. Front Microbiol 9: 1108.
-
Thatai P, Sapra B (2016) Critical review on retrospective and prospective changes in antifungal susceptibility testing for dermatophytes. Mycoses 59(10): 615-627.
-
Bondaryk M, Kurztkowski W, Staniszewska M (2013) Antifungal agents commonly used in superficial and mucosal candidiasis treatment: mode of action and resistance development. Postepy Dermatol Allergol 30(5): 293-301.
-
Barry AL, Pfaller MA, Rennie RP, Fuchs PC, Brown SD (2002) Precision and Accuracy of Fluconazole Susceptibility Testing by Broth Microdilution, Etest, and Disk Diffusion Methods. Antimicrob Agents Chemother 46(6): 1781-1784.
-
Gupta AK, Mays RR, Versteeg SG, Piraccini BM, Shear NH, _et al_. (2018) Tinea capitis in children: a systematic review of management. J Eur Acad Dermatol Venereol 32(12): 2264-2274.
-
Mikaeili A, Kavoussi H, Hashemian AH, Gheshtemi MS, Kavoussi R (2019) Clinico-mycological profile of Tinea capitis and its comparative response to griseofulvin versus terbinafine. Curr Med Mycol 5(1): 15-20.
-
Shukla AK, Bhushan B, Mishra DK, Chaudhary SS, Jha MK, _et al_. (2019) Comparative study of oral terbinafine vs. oral griseofulvin in the management of tinea capitis. International Journal of Research in Dermatology 5(3): 629-636.
-
Singh J, Zaman M, Gupta AK (2007) Evaluation of microdilution and disk diffusion methods for antifungal susceptibility testing of dermatophytes. Med Mycol 45(7): 595-602.
-
Alkeswani A, Cantrell W, Elewski B (2019) Treatment of tinea capitis. Skin Appendage Disorders 5: 201-210.
-
Chen BK, Friedlander SF (2001) Tinea capitis update: a continuing conflict with an old adversary. Curr OpinPediatr 13: 331-335.
-
Deng S, Hoog GSD, Verweij PE, Zoll J, Ilkit M, _et al_. (2015) In vitro antifungal susceptibility of Trichophyton violaceum isolated from tinea capitis patients. J Antimicrob Chemother 70(4): 1072-1075.
-
Dogra S, Shaw D, Rudramurthy SM (2019) Antifungal drug susceptibility testing of dermatophytes: Laboratory findings to clinical implications. Indian Dermatology Online Journal 10(3): 225-233.
-
Chen X, Jiang X, Yang M, González U, Lin X, _et al_. (2016) Systemic antifungal therapy for tinea capitis in children. Cochrane Database Sys Rev (5): CD004685.
-
Hanselmayer GG, Smolle J, Gupta A (2004) Itraconazole in the treatment of tinea capitis caused by Microsporum canis: experience in a large cohort. Pediatr Dermatol 21(4): 499-502.
-
Mathioudaki EK, Panagiotidou DD, Rallis E, Athanassopoulou V, Eremondi TK, _et al_. (2005) Is itraconazole the treatment of choice in Microsporum canis tinea capitis? Drugs Exp Clin Res 31: 11-15.
-
Gupta AK, Foley KA, Versteeg SG (2017) New antifungal agents and new formulations against dermatophytes. Mycopathologia 182(1-2): 127-141.
-
Favre B, Hofbauer B, Hildering KS, Ryder NS (2003) Comparison of in vitro activities of 17 antifungal drugs against a panel of 20 dermatophytes by using a microdilution assay. J Clin Microbiol 41(10): 4817-4819.
-
Grover C, Arora P, Manchanda V (2012) Comparative evaluation of griseofulvin, terbinafine and fluconazole in the treatment of tinea capitis. Int J Dermatol 51(4): 455-458.
-
Rubio MC, Gil J, Oca IRD, Benito R, Rezusta A (2003) Comparison of results obtained by testing with three different agar media and by the NCCLS M27-A method for in vitro testing of fluconazole against Candida spp. J Clin Microbiol 41(6): 2665-2668.
-
Kimberlin DW, Brady MT, Jackson MA (2018) Committee on Infectious Diseases, American Academy of Pediatrics. Red Book 2018-2021: Report of the Committee on Infectious Diseases. Itasca, IL: American Academy of Pediatrics.
-
Arenas R, Duran JER, Sigall DA, Vega DC (2019) Tinea capitis: A Practical Approach. OAJMMS 2(2): 1-6.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia