Clinical-Epidemiological Characteristics in Outpatients with Mild to Moderate Covid-19, in the South of Mexico City
Background: Regional information on the characteristics of patients with mild and moderate intensity SARS-CoV-2 “COVID-19” coronavirus disease is needed to better understand the pandemic Objective: The objective of this study was to report the epidemiological clinical characteristics of outpatients with mild to moderate intensity COVID-19 that was carried out by Telemedicine in a first contact clinic, specializing in infectious diseases, in the South from Mexico City from March 10, 2020 to January 31, 2021. Material and Methods: This is a prospective, cross-sectional, observational, single-center study of a series of patients with clinical data of upper and lower respiratory tract infection and a positive CRP for SARS-CoV-2, who requested telemedicine consultation from a first contact clinic with a specialty in infectious diseases, attended from March 10, 2020 to January 31, 2021, The information was analyzed in a statistical package using SPSS 23.0. Results: 66patients who met the established criteria for diagnosis were attended to. In January 2021, the highest number of patients was treated; they requested medical attention, 6.5 days (range from 1 to 12 days) after having started with the disease. The median age was 48 years (range 10 to 80 ) years), 53% were female, 26% had type 2 diabetes mellitus, 23% with arterial hypertension, 7% previous pulmonary disease, 4% suffered from hypothyroidism, 24% positive smoking, 21% positive alcoholism, 39% had obesity , 17% were allergic. The clinical characteristics, the most prevalent was cough in 76%, followed by headache in 73% and myalgia in 71%. Conclusions: Patients with comorbidities, whether they are men or women in the fifth decade of life, are important for the evolution, especially when they are carriers of immunosenescence in the cases of those older than 60 years, or the immune system is immunocompromised as it is the case of patients with DM2 and even more so when they have more than one comorbidity that persists, they have a pro- inflammatory state and attenuation of the innate immune response.
Introduction
In December 2019, an outbreak of pneumonia of unknown cause occurred in the People’s Republic of China in Wuhan, Hubei Province. This led to a thorough investigation by the Wuhan health authorities and reported to the World Health Organization (WHO) the presence of 27 cases of Acute Respiratory Syndrome of unknown etiology [1, 2]. Chinese scientists isolated a new strain of coronavirus and carried out genetic sequencing, which was made available to WHO, facilitating laboratories in different countries to produce specific PCR diagnostic tests to detect the new infection. The isolated virus belongs to the Beta coronaviruses of group 2B with at least 70% similarity in the genetic sequence with SARS-CoV, which was named by the WHO as 2019- nCoV [3]. The World Health Organization (WHO) declares “Outbreak” as a Public Health emergency of international concern, on January 30, 2020. The International Committee on Taxonomy of Viruses (ICTV), a global authority for naming viruses, has referred to it as SARS-CoV -2. In Mexico, the first confirmed case was reported on February 28, 2020, John Hopkins University reports for Mexico City as of April 11, 2021; reports 2,278,420 cases and 209,212 deaths from COVID-19 [4].
In our Country (Mexico City), epidemiological surveillance is carried out with strict case definitions for identification: COVID-19 Case Operational Definitions [1]
Suspicious Case
Person of any age who in the last 10 days has presented at least one of the following signs and symptoms: cough, dyspnea, fever or headache, Accompanied by at least one of the following signs or symptoms:
- Myalgia
- Arthralgia
- Odynophagia
- Chills
- Chest pain
- Rhinorrhea
- Polypnea
- Anosmia
- Dysgeusia
- Conjunctivitis.
Case of Serious Acute Respiratory Infection (SARI)
Any person who meets the definition of a suspected case and the presence of any of the following severity data: dyspnea, chest pain or desaturation.
Laboratory-confirmed case
Person who meets the operational definition of a suspected case and has a laboratory-confirmed diagnosis through RT-PCR.
Case confirmed by rapid antigenic test for SARS- CoV-2
Person who meets the operational definition of a suspected case and has a positive rapid antigenic test for SARS-CoV-2.
Confirmed case by epidemiological association
Person who meets the operational definition of a suspected case and who has been in close contact (living together within 1 meter of distance for 15 continuous or accumulated minutes or more [1]. Clinical information on confirmed COVID-19 cases reported so far suggests a different disease course than that seen in SARS-CoV and MERS-CoV cases. However, with research still ongoing, it is difficult to assess whether there are population groups at higher risk of severe disease [2, 5]. Preliminary information suggests that older adults and people with underlying health conditions may be at increased risk of developing disease serious due to this virus [6]. Because it is a new virus and it evolves rapidly, information is constantly updated throughout the world [3], it is still necessary to have more information given the characteristics of the virus, transmission mechanism, reservoir, specific clinical characteristics and severity of the disease, in order to control the impact of COVID-19
Objective
The objective of this study was to report the epidemiological clinical characteristics of outpatients with mild to moderate intensity COVID-19 that was carried out by Telemedicine in a first contact clinic, specializing in infectious diseases, in the South from Mexico City from March 10, 2020 to January 31, 2021.
Material and Methods
This is a prospective, cross-sectional, observational, single-center study of a series of patients with clinical data of upper and lower respiratory tract infection and a positive CRP for SARS-CoV-2, who requested telemedicine consultation to a first-rate clinic. Contact with a specialty in infectious diseases, attended from March 10, 2020 to January 31, 2021.
A mild to moderate COVID-19 case was considered to be patients who had a positive PCR test for SARS-2 CoV-2
plus the presence of symptoms; fever, dry cough, headache, odynophagia, dyspnoea, arthralgia, myalgia, odynophagia, shortness of breath, hyposmia, dysgeusia, dysphagia, asthenia, diarrhea, conjunctivitis, rash whether they present all the clinical data or incomplete and sign the informed consent Those patients who presented criteria for hospitalization, who did not sign informed consent, and another circumstance that prevented them from making a follow-up video call were excluded.
A pre-coded questionnaire was carried out, designed only for this study, the identification card was taken and the following variables were measured: sociodemographic characteristics date of the first consultation, sex, age in completed years, weight). Non-pathological personal history (probable transmission mechanism, family, public transport, work, unknown). Pathological personal history (comorbidities diabetes mellitus, arterial hypertension, previous pulmonary pathology, cancer, HIV, AIDS, asthma, allergy, obesity, disease cardiovascular disease, smoking, alcoholism) Current Condition Signs and symptoms (date of first symptom and date of first consultation, fever greater than 38°C, cough, headache, dyspnea, arthralgia, myalgia, odynophagia, shortness of breath, hyposmia, Dysgeusia, dysphagia , asthenia, diarrhea, conjunctivitis, rash, anxiety and depression)
Laboratory Studies Were Requested
Complete blood count, glucose, creatinine, ORT, TGP, Erythrocyte sedimentation rate (ESR), C- reactive protein (CRP), Clotting times (PT, PTT), D-Dimer, Ferritin, Gamma interferon, Interleukin 1, (IL 1), IL6, IL8, IL17, NK, CD8, CD4, Cd3, CD8 / CD4, COVID- 19 viral load, AP and lateral chest X-ray and / or Simple chest tomography ) The information was analyzed in a statistical package using SPSS 23.0. The categorical variables presented as percentages were analyzed with chi square or Fisher’s exact tests. Continuous distribution variables were expressed as mode, median and were compared with the Mann Whtney U test. A p <0.05 was considered statistically significant.
Results
We found that during the period from March 10, 2020 to January 31, 2021, 106 patients with a positive PCR test for SARS-2 CoV-2 requested medical attention by telemedicine, of which 12 (11%) had signs and symptoms for entering hospital surveillance and treatment, 34 (30%) did not have laboratory studies, so they were eliminated, leaving 66 patients who met the criteria established for diagnosis, so they were included for the analysis.
In relation to the season, in the month of January 2021 “winter stage” was where more patients requested medical attention 28 (42%), followed by 15 (23%) in the month of December 2020 (see graph 1). From the date the symptoms began to the day they requested a consultation for COVID-19 was 6.5 days (range 1 to 12 days), The average age was 48 years with a range (10-80 years) 35 (53%) Corresponded females, 17 (26%) had type 2 diabetes mellitus, 15 (23%) with hypertension, 5 (7%) had Previous pulmonary disease, 3 (4%) had hypothyroidism, 16 (24%) had positive smoking, 14 (21%) Positive alcoholism, 26 (39%) had obesity, 11 (17%) were allergic (Table 1).
Clinical Characteristics
The respiratory rate at the time of consultation was 20 breaths per minute (BPM) with an average of (14 to 22 BPM), oximetry was 89 range (85 to 96), Fever greater than 38 degrees 35 (53 %), Cough 50 (76%), Headache 48 (73%), Arthralgia18 (27%), Myalgia 47 (71%), Odynophagia 19 (29%), Difficulty breathing 15 (23%), Hyposmia 38 (57 %), Dysgeusia 37 (56%), Dysphagia 19 (29%), Asthenia 41 (71%), Diarrhea 21 (32%), Conjunctivitis 1 (1%), Rash 1 (1%), Anxiety 13 (20%), Depression 7 (11%) Hyporexia 23 (35%) (Table 1).
Laboratory Exams
Hematic biometry, leukocytes with a mean range of 7,040 (1,730 to 15,600), mean hemoglobin 14 (range 11 to 18), mean platelets of 240 thousand (range of 109 to 471 thousand), Neutrophils mean of 68 (range of 49 to 92), mean lymphocytes of 24 with (range 7 to 37), mean monocytes of 6.5 (range 0to 17). Blood chemistry: mean glucose 102 (range 67-263), mean creatinine 0.89 (range 0.5 to 1), mean TGO 38 (range 16 to 77), mean TGP 43 (range 17 to 131) SARS CoV-2 biomarkers: Mean ESR 29 (range 1 to 98), Mean CRP 22 (range 3-165) Mean Dimero D 220 (range 10 to 5159), Mean Ferritin 297 (range 3 to 4253) Coagulation tests: mean PT of 13.34 (range 10 to 15) mean PT of 31 (range 11.5 to 36). 25 Hydroxyl vitamin D mean 20 (range 8 to 35) Imaging tests: Chest X-ray 37 (56%) was reported without alteration, 16 (24%) was reported with pneumonia, Chest CT scan 15 (22%) was performed, the study was compatible with pneumonia.
Immunization
Vaccine history against influenza 14 (21%) had been applied in 2020 Probable transmission mechanisms: The first transmission mechanism was 33 (50%) by a relative followed by 19 (29%) by public transport, 10 (15%) at work and 4 (6%) ignored it Day to day treatment Ivermectin was received by 58 (88%). Pidotimod 63 (95%), Vitamin D3 63 (95%), Vitamin C 60 (90%), Complex B 50 (76%), Prednisone 24 (36%), Dexamethasone 29 (44%) Rivaroxaban 13 (19%) Aspirin 48 (73%), Paracetamol 35 (53%) Ibuprofen 4 (6%), amoxicillin 12 (18%) was prescribed, followed by Ceftriaxone 8 (12%), azithromycin 6 (9%), amoxicillin with sulbactam 2 ( 3%), cefuroxime 2 (3%), and amoxicillin with clavulanic acid and clarithromycin in one patient, Oral antiseptic was prescribed in 44 (67%), Budenosine / formoterol 21 (32%), Budenosine 16 (24%), Melatonin 25 (38%), Supplemental oxygen 32 (47%).
| Characteristics | Number of patients (n = 66) and percentages | Sex of patients and percentages | P value | ||
|---|---|---|---|---|---|
| Female | male | ||||
| Cases | 66 (100%) | 35 | 31 | ||
| Average age | 48 años | 46 años | 49 años | ||
| Smoking history | 16 (24%) | 7 | 9 | ||
| History of positive alcoholism | 14 (21%) | 5 | 9 | ||
| History of chronic degenerative diseases | Diabetes mellitus type 2 | 17 (26%) | 8 | ||
| Arterial hypertension | 15 (23%) | 7 | 8 | ||
| Hypotiroidism | 3 (4%) | 3 | 0 | ||
| Previous pulmonary pathology | Asthma | 5 (7%) | 4 | 1 | |
| Obesity | 26 (39%) | 15 | 11 | ||
| Previous cardiovascular disease | Cardiovascular surgery | 2 (3%) | 2 | ||
| Allergy History | 11 (17%) | 7 | 4 | ||
| Signs and symtoms | Fever | 35 (53%) | 17 | 18 | |
| Dry cough | 50 (76%) | 23 | 27 | P<0.05 | |
| Headache | 48 (73%) | 27 | 21 | ||
| Arthralgia | 18 (27%) | 7 | 11 | ||
| Myalgia | 47 (71%) | 26 | 21 | ||
| Odunophagia | 19 (29%) | 11 | 8 | ||
| Shortness of breath | 15 (23%) | 6 | 9 | ||
| Hyposmia | 38 (58%) | 21 | 17 | ||
| Dysgeusia | 37 (56%) | 19 | 18 | ||
| Dysfagia | 19 (29%) | 11 | 8 | ||
| Asthenia | 47 (71%) | 23 | 24 | ||
| Diarrhea | 21 (32%) | 13 | 8 | ||
| Exanthema | 1 (1%) | 0 | 1 | ||
| Anxiety | 13 (20%) | 6 | 7 | ||
| Depressión | 7 (11%) | 4 | 3 | ||
| Chest x- ray AP and lateral | With pneumonia data | 16 (24%) | 5 | 11 | P<0.05 |
| The anti-influenza vaccine had been applied | 14 (21%) | 8 | 6 | ||
| Probable transmission mechanism | By an infected family member | 33 (50%) | 18 | 15 | |
| At work | 10 (15%) | 5 | 5 | ||
| In public transport | 19 (29%) | 10 | 9 | ||
| Ignore it | 4 (6%) | 2 | 2 |
Table 1: Characteristics of the population studied by sex.
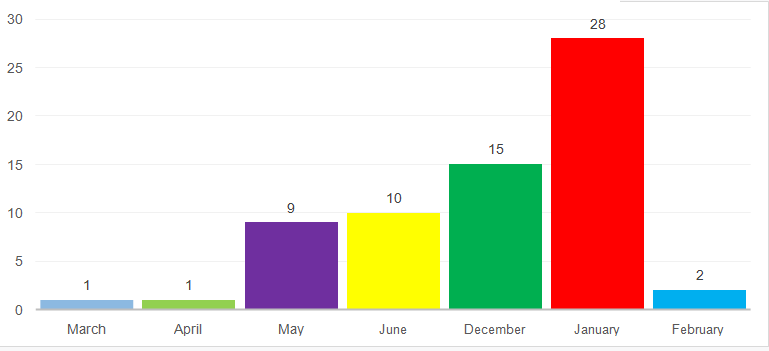
Graph 1: Number of cases consulted per month and year.
Analysis of Results
According to the circulation of viruses in our country, SARS CoV-2 “COVID-19” circulated throughout the year, being the winter months where more cases were reported nationally in our country, in this study the month of January 2021, 66/28 (42%) requested more patients, followed by the month of December 2020. Within the epidemiological characteristics, there was a slight predilection for the female sex with cases 66/35 (53%) with a ratio (1.1: 1), for the mild to moderate presentation of the disease, with an age range within adulthood with a peak within the 5th decade of life. The predominance of subjects in the fifth decade of life can be explained by the high prevalence of overweight, a comorbidity that occurred especially in females with 39%, secondly, it was Diabetes Mellitus type 2 and Hypertension with 26 % and 23% respectively. Of the obese patients, 12 (46%) required oxygen, of these patients, 3 (25%) had comorbidity with DM and HT, and 6 (23%), only had obesity; of patients with DM + HT 66/21 (32%) required oxygen. Within the use of substances, it was found that 24% consumed tobacco and of these, 60% required oxygen support; and 21% alcohol, without having alterations in liver enzymes or clotting times.
The clinical presentation was highly variable, where we have that 76% had a dry cough (Table 2), which was the most prevalent symptom, in second place headache 73% (Table 3) and in third place myalgia (Table 4) and asthenia with 71%; It is striking that only a little more than half (53%) had fever (Table 5) and that the presence of hyposmia (58%) and Dysgeusia (56%) were even slightly more prevalent. The cognitive state also presented in the first place anxiety and depression with 20% and 11% respectively, which were referred to specialists in the field. Within the paraclinics; 66/34 (51%) of the patients presented lymphopenia below 1500, of these 20 (58%) required oxygen and 28 (82%) required steroid for its management; 66/7 (11%) presented plaquetopenia below 150 thousand, of these 6 required oxygen and systemic steroid; 66/9 (14%) with ferritin levels above 500, of which 6 required oxygen and 9 systemic steroid; 66/2 (3%) had kidney disease, of which one had a history of obesity and DM, and the other of hypertension; 66/16 (24%) presented alterations in the radiographs, where only one patient with a history of allergy and obesity presented data of air trapping and the rest with data of pneumonia, of which 76% (13) and 88% required oxygen (15) some type of antibiotic was administered. It is worth mentioning that only 21% had a history of having been vaccinated with an anti-influenza vaccine. The main transmission mechanism was by an infected family member in 50% of the cases, followed by 29% of probable acquisition in public transport. Regarding treatment, 90% required some type of anticoagulation (73% acetylsalicylic acid (ASA) and 13% Rivaroxaban); 80% received some type of systemic steroid (44% dexamethasone, 36% Prednisone); 48% of the patients received inhaled steroid, of these 66/21 (32%) received Budenosine/ formoterol, all with a history of receiving systemic steroid except one. 66/32 (47%) required supplemental oxygen. 66/63 (95%) of the patients were recommended to use an immune regulator of the Pidotimod type, 95% were prescribed Vitamin D3 and other vitamins, 88% received Ivermectin, antibiotics were prescribed for 66/32 (48% ) of the cases (amoxicillin 18%, Ceftriaxone 12%, azithromycin 9%, amoxicillin with sulbactam 3% and others).
| Cough | Total | ||||
|---|---|---|---|---|---|
| Dry Cough | No Cough | ||||
| SEX | female | Count | 23 a | 12 b | 35 |
| % inside sex | 65.70% | 34.30% | 100.00% | ||
| male | Count | 27 a | 4 b | 31 | |
| % inside sex | 87.10% | 12.90% | 100.00% | ||
| Total | Count | 50 | 16 | 66 | |
| % inside sex | 75.80% | 24.20% | 100.00% |
Table 2: Cross Table.
Each letter of the subscript denotes a subset of TOS categories whose column proportions do not differ significantly from each other at the .05 level.
| Headache | Total | ||||
|---|---|---|---|---|---|
| Yes | No | ||||
| SEX | female | Count | 27 a | 8 a | 35 |
| % inside sex | 77.10% | 22.90% | 100.00% | ||
| male | Count | 21 a | 10 a | 31 | |
| % inside sex | 67.70% | 32.30% | 100.00% | ||
| Total | Count | 48 | 18 | 66 | |
| % inside SEX | 72.70% | 27.30% | 100.00% |
Table 3: Cross Table.
Each letter of the subscript denotes a subset of HEADACHE categories whose column proportions do not differ significantly from each other at the .05 level.
| Mialgias | Total | ||||
|---|---|---|---|---|---|
| Yes | No | ||||
| SEX | female | Count | 26 a | 9 a | 35 |
| % inside sex | 74.3% | 25.7% | 100.0% | ||
| male | Count | 21 a | 10 a | 31 | |
| % inside sex | 67.7% | 32.3% | 100.0% | ||
| Total | Count | 47 | 19 | 66 | |
| % inside SEX | 71.2% | 28.8% | 100.0% |
Table 4: Cross Table.
Each letter of the subscript denotes a subset of MIALGIAS categories whose column proportions do not differ significantly from each other at the .05 level
| Fever | Total | ||||
|---|---|---|---|---|---|
| 38 A 39° | No | ||||
| SEX | female | Count | 17 a | 18 a | 35 |
| % inside sex | 48.6% | 51.4% | 100.0% | ||
| male | Count | 18 a | 13 a | 31 | |
| % inside sex | 58.1% | 41.9% | 100.0% | ||
| Total | Count | 35 | 31 | 66 | |
| % inside SEX | 53.0% | 47.0% | 100.0% |
Table 5: Cross Table.
Each letter of the subscript denotes a subset of FEVER categories whose column proportions do not differ significantly from each other at the .05 level
| Pneumonia | |||||||
|---|---|---|---|---|---|---|---|
| Without Alteration | Air Entrapment | Comunity Pneumonia | I Did Not Take | Total | |||
| SEXO | female | Count | 22 a | 1 a | 5 a | 7 a | 35 |
| %inside sex | 62.90% | 2.90% | 14.30% | 20.00% | 100.00% | ||
| male | Count | 15 a | 0 a | 11 a | 5 a | 31 | |
| % inside sex | 48.40% | 0.00% | 35.50% | 16.10% | 100.00% | ||
| Total | Count | 37 | 1 | 16 | 12 | 66 | |
| % inside SEX | 56.10% | 1.50% | 24.20% | 18.20% | 100.00% |
Table 6: Cross table Aspirin 48 (73%), Rivaroxaban 13 (20%), Prednisone 24 (36%), Dexamethasone 29 (44%), Antipyretics and non-st
Table 6: Cross table Aspirin 48 (73%), Rivaroxaban 13 (20%), Prednisone 24 (36%), Dexamethasone 29 (44%), Antipyretics and non-steroidal anti-inflammatory drugs, the most prescribed was paracetamol in 35 (53%). Each letter of the subscript denotes a subset of PNEUMONIA categories whose column proportions do not differ significantly in tri at level 0.5
Discussion
Comparing the results of this study with other investigations was difficult, because there are few studies reported in outpatients with mild to moderate intensity COVID-19 in adult patients. In this study we describe the experience of a first contact clinic with a specialty in infectious diseases, in the south of Mexico City, the results provide the complete description of the clinical and epidemiological characteristics of the first wave of patients diagnosed with SARS- CoV-2 COVID-19, it was possible to identify the clinical, epidemiological, laboratory and imaging differences.
The treatment that was recommended for each subject is also described, individualizing each patient. These findings could be of use to first-contact clinicians According to the circulation of viruses in our country, SARS CoV-2 “COVID-19” circulated throughout the year, prevailing in the winter stage (1) as well as other respiratory viruses such as the influenza virus, virus respiratory syncytial that more cases are observed with the cold. Probably because in the cold season there is less social distance, there is less ventilation to keep heat in homes and workplaces and of course these are factors for more infections [7].
In general, the majority were women in their fifth decade of life, with comorbidities such as obesity, arterial hypertension and DM2, as the most prevalent, it was notorious that age and comorbidities added importance for the evolution of patients, especially when they are carriers of immune senescence in the cases of those over 60 years of age, or the immune system is immune compromised as is the case of patients with DM2 or when you have more than one comorbidity that persists, they have a pro-inflammatory state and attenuation of the innate immune response [8, 9].
Other comorbidities such as a history of smoking and positive alcoholism predominated in males, and are risk factors because they increase the development of a respiratory infection, alcohol affects different levels of the immune response from the cough reflex and epiglottic, which can cause aspiration risk and decrease chemotaxis and microbial activity and tobacco significantly increases gene expression of angiotensin converting enzyme 2, the binding receptor for severe acute respiratory syndrome coronavirus, which could explain the high susceptibility to COVID-19 in smokers. Furthermore, cigarette smoking is the leading cause of chronic obstructive pulmonary disease, which has been identified as an independent risk factor for severe cases of COVID-19 [10].
From the date on which symptoms began to the day they requested a consultation, it was 6.5 days, similar to that reported by Ortiz, et al. [11]. The most frequent symptoms were cough, headache, myalgia, asthenia) which contrasts with that reported by Ortiz, et al. [11]. The clinical manifestations depend on the viremia phase, where the virus passes from the mucous membranes, especially the nasal and larynx, and also enters the lungs through the respiratory tract and if it attacks other organs such as the digestive tract, kidney , heart, brain etc [8, 12, 13].
The dynamic profile of some laboratory tests related to the degree of inflammation were different in each patient, lymphopenia, and biomarkers such as C-reactive protein, ESR, Ferritin, Dimero D, were more frequent in patients with chronic comorbidities. Decreased vitamin D3 was found, and the deficiency is related to a high risk of infections due to the multiple functions in the body [14, 15].
To date, we do not have a targeted, effective and safe treatment to eliminate SARS-CoV-2, so the treatment for the patients in this study was individualized and established according to the different clinical scenarios and patient comorbidities. In general, in the absence of a specific treatment, we emphasize on improving the immune system, knowing that the immune system is a perfect system that combines a whole range of cells and mediators to provide protective immunity against infectious agents. Its intervention in early reactions (innate immunity) and later in (adaptive immunity) both very important for the defense against intracellular germs such as SARS-COV2, Pidotimod was prescribed as an immune modulator, in the acute phase with an 800mg tablet every 12hrs for 2 weeks, followed by a tablet every 24 hours for 4 more weeks, since the population that was treated had comorbidities that made them immune compromised, we favor Pidotimod because it stimulates the immune cells of the innate and adaptive response, studies Like that of Ferrario et al., they highlight it as a molecule capable of improving the response to inflammatory stimuli acting on different immunological pathways [8, 16], Ning Zhao et al, report the effectiveness in respiratory tract infections of viral origin [17]. Esposito S et al, reports it as an immunomodulator that can be given at the same time as an antibiotic with a good response [18], Claudio Ucciferri et al, and n a study in paucisymptomatic patients infected by SARS-CoV2, found and reported a significant reduction in systemic symptoms of the disease [19], other recent studies also recommend it [20, 21, 22]. The use of antibiotics was limited to patients who presented data compatible with community pneumonia with bacterial over aggregation, in which we covered the most frequent germ Streptococcus pneumoniae, the criteria was by laboratory and imaging and associated comorbidity. Initially prescribing amoxicillin as recommended by recent studies [23, 24, 25].
Conclusion
The new coronavirus SARS CoV-2 “COVID-19” has been epidemiologically presented throughout the year, so it is extremely important to be preventive with ourselves and our family environment and with patients, indicating immunization according to age, but in the case of adults and specifically for this disease, the anti-influenza vaccine and the vaccine against Streptococcus pneumoniae and obviously the vaccine for SARS-CoV2 that is being applied throughout the world, plus strengthening the immune system with immune modulars, this strategy should be Recommend especially to frail or elderly subjects due to immune senescence, to prevent the appearance and reduce the duration of viral or bacterial respiratory tract infections and anticipate the appearance of complications plus continue with good personal hygiene practices, use of masks and a tight mask, avoid places with a lot of people and keep a distance of 1.5 meters with other people, to prevent infection in this case by SARS-CoV2 and as physicians to control the source of infection, provide an early diagnosis, inform, isolate, generate supportive treatment and publish.
References
-
Lineamiento estandarizado para la vigilancia epidemiológica y por laboratorio de la enfermedad respiratoria viral. Enero de 2021. Secretaría de Salud. Subsecretaría de Prevención y Promoción de la Salud. Dirección General de Epidemiología.
-
(2020) Risk assessment - pneumonia Wuhan China.
-
David S Hui, Esam I Azhar, Tariq A Madani, Christian Drosten, Alimuddin Zumla, et al. (2020) The continuing COVID-19 epidemic threat of novel coronaviruses to global health-The la-test 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 91: 264-266.
-
Novel Coronavirus 2019, Wuhan, China | CDC.
-
Novel Coronavirus in Hubei Province, China.
-
Noor A, Fiorito T, Krilov L (2019) Cold weather viruses. Pediatrics in Review 40: 10.
-
Gerardo T Lopez Perez et al. (2020) Evaluation of immune Response, Comorbidities and immunomodulation in SARS-CoV2 Pandemic. EC Paediatrics 9.6 872-892
-
Yang J. Ya Zheng, Xi Gou, Ke Pu, Zhaofeng Chen, et al. (2020) Prevalence of comorbidities in the novel Wuahn coronavirus (COVID-19) Infection: a systematic review and meta-analysis. International Journal of Infectious Diseases. 94: 91-95.
-
Cai G (2020) Bulk and single-cell transcriptomics identify tobacco-use disparity in lung gene expression of ACE2, the receptor of 2019- nCov. Medicine Rxiv.
-
Ortiz-Brizuela E, Marco Villanueva-Reza, María F González-Lara, Karla M Tamez-Torres, Carla M Román- Montes, et al. (2020) Clinical and Epidemiological Characteristics of Patients Diagnosed with COVID- 19 in a Tertiary Care Center in Mexico City: A Prospective Cohort Study**.** _Rev. invest. clín._ 72(3): 165-177.
-
Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus- infected pneumonia in Wuhan, China. JAMA 323(11): 1061-1069.
-
Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, et al. (2020) Presenting characteristics, comorbidities and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA 323(20): 2052-2059
-
Ramírez Sanchez, Pedroza MÁ (2019) Vitamina D y su papel en el sistema inmune. Alergia, Asma e Inmunologia Pediatricas. 28(1): 26-34.
-
Dirección General de Epidemiología (2021) Lineamiento estandarizado para la vigilancia epidemiológica y por laboratorio de enfermedad por 2019-nCoV.
-
Ferrario BE, Silvia Garuti, Fulvio Braido, Giorgio W Canonica (2015) Pidotimod: the state of art”. Clinical and Molecular Allergy 13(1): 8.
-
Ning Zhao, Chuanhe Liu, Chunmei Zhu, Xiaoyan Dong, Xiuyun Liu (2019) Pidotimod: a review of its pharmacological Features and Clinical effectiveness in respiratory tract infections. Expert Review of Anti- infective Therapy 17(10): 803-818
-
Esposito S, Micaela Garziano, Veronica Rainone, Daria Trabattoni, Mara Biasin, et al. (2015) Immunomodulatory activity of pidotimod administered with standard antibiotic therapy in children hospitalized for community-acquired pneumonia. Journal of Translational Medicine 13: 288.
-
Ucciferri Claudio, Mirko Barone, Jacopo Vecchiet, Katia Falasca, et al. (2020) Pidotimod in Paucisymptomtic SARS-CoV2 Infected Patients. Mediterranean J Hematology Infect Dis 12(1): e2020048.
-
Pugggioni F, Magna Alves-Correia, Manar-Farouk Mohamed, Niccolò Stomeo, Riccardo Mager, et al. (2019) Immnoestmulantes in respiratory Diseases: focus on Pidotimod. Multidisciplinary Respiratory Medicine 14:31.
-
Fogli M, Caccuri F, Iaria ML, Giagulli C, Corbellini S, et al. (2014) The immunomodulatory molecule pidotimod induces the expression of the NOD- like receptor NLRP12 and attenuates TLR-induced inflammation”. Journal of Biological Regulators and Homeostatic Agents 28(4):753-766.
-
Trabattoni D, M Clerici, S Centanni, M Mantero, M Garziano, et al. (2017) “Immunomodulatory effects of pidotimod in adults with community acquired pneumonia undergoing standard antibiotic therapy”. Pulmonary Pharmacology and Therapeutics 44: 24-29.
-
Baez-Saldaña R, Gómez-Zamora C, López-Elizondo C, Molina-Corona H, Santillán-Martínez A, et al. Neumonía adquirida en la comunidad. Revision y actualización con una pespectiva orientada a la calidad de la atención medica. Neumol Cir Torax 72(1): 6-43.
-
Neumonía adquirida en la comunidad. (2010) Nueva Normativa de la Sociedad Española de Neumología y Cirugía Torácica (SEPAR). Arch Bronconeumol 46: 543- 558.
-
Mandell LA, Wunderink RG, Anzuelo A, John G Bartlett, G. Douglas Campbell, et al. (2007) Infectious Diseases Society of Ameria/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. CID 44(2): S27-S72.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia