Epidemiology of Serratia Marcescens in the Neonatal ICU of A Tertiary Hospital in Oman over a 10 Years Period
Background: Serratia marcescens has been described as a significant nosocomial organism. Several S. marcescens outbreaks in Neonatal Intensive Care Units (NICUs) were described as causing fatal meningitis, sepsis or pneumonitis in premature or low birth weight neonates with a mortality rate of 44%. The primary objective of this study is to describe the outcome (mortality and length of hospital stay) of S. marcescens infection in NICU at a tertiary care hospital over ten years (2009 -2018). Secondary objectives are to describe the incidence of S. marcescens infection/colonization in NICU, study the risk factors associated with S. marcescens infection/colonization, and the microbiology of this organism. Method: A retrospective, unmatched case-control study was conducted between January 2009 to December 2018. Data were analyzed using IBM SPSS Statistics 28.0. A multivariate binary logistic regression analysis was performed to determine the independent predictors of Serratia marcescens and mortality among Serratia marcescens infected patients. The Odds Ratio (OR) was reported with its 95% CI. A P-value less than 0.05 was considered statistically significant. Result: A total of 93 cases had a positive culture of S. marcescens in neonates hospitalized in the NICU during the study period and 201 controls were included. 50.5% (n=47) of cases were male and 49.5% (n=46) were females. The clinical features of infection by S. marcescens range from asymptomatic colonization (16.1%) to potentially fatal sepsis (38.7%) and meningitis (1.1%). 13 cases (17.3 %) had colonization before infection. Mortality rate among infected neonates was 17%. Multivariate analysis showed that female gender (OR= 1.969, 95% CI= 1.020-3.801, P= 0.044), premature birth ((OR= 2.670, 95% CI= 1.156-6.167, P= 0.021). C-section (OR= 3.238, 95% CI= 1.591-6.591, P= 0.001), type of feeding and surgery (OR= 3.719, 95% CI= 1.546-8.946, P= 0.003) were independent predictors for acquiring S. marcescens. Female gender was an independent factor for mortality from Serratia infection (OR= 6.741, 95% CI= 1.307-34.767, P= 0.023). Conclusion: S. marcescens is an important pathogen that has a propensity to cause difficult-to-control outbreaks in NICUs. Healthcare workers' awareness of this organism and enhancement of infection prevention and control measures is a vital requirement to prevent HAIs among susceptible neonates.
Muna AL Mahrooqi*, Zaina AL Maskari, Sachin Jose and Amal AL Tai
Royal Hospital, Oman *Corresponding author: Zaina Al Maskari, Royal Hospital, Oman, Email: zainamaskri2000@ gmail.com
Introduction
Healthcare-associated infections (HAIs) are among the leading causes of mortalities, morbidities, and prolonged hospital stay, resulting in considerable associated economic patient care costs. Serratia marcescens is a gram-negative bacterium described as a significant nosocomial organism that can rapidly spread, particularly in neonatal intensive care units (NICUs). The third highest number of published outbreaks is due to S. marcescens, after Klebsiella spp. and S. aureus [1]. Several S. marcescens outbreaks in NICUs were described as causing fatal meningitis, sepsis or pneumonitis in premature or low birth weight neonates with a high mortality rate of 44% which is much higher than mortality rate caused by Enterobacter cloacae, another pathogen well- known to cause disease and death in premature neonates [2].
This bacterium can be transmitted to neonates via feeding, contaminated breast pumps and antiseptics, and it can spread through contact with patients [3]. Contaminated baby shampoo was identified as the source of the outbreak in the King Abdulaziz University Hospital in Saudi Arabia. Withdrawal of the shampoo product led to the termination of the outbreak [4].
The primary objectives were to describe the Outcome (30 days mortality & length of hospital stay) of S. marcescens infection in the NICU and the determinants of mortality among infected patients. The secondary objectives were to estimate the incidence of S. marcescens infection/colonization in the NICU at Royal hospital and to study the risk factors for acquisition and the microbiology of S. marcescens strains.
Method
Setting, study designs a retrospective case-control study in the NICU of Royal Hospital, Sultanate of Oman, from 2009 to 2018. The Royal Hospital is a tertiary hospital that provides inpatient and outpatient health care services to the country. The NICU has 35 beds, 16 of which were assigned for critical cases. The unit has no active S. marcescens screening; however, at the time of outbreaks, active screening surveillance is implemented till the outbreak is controlled.
Population Definitions
The target population for the study was neonates admitted to NICU at Royal hospital from 2009-2018. Cases include all neonates with a positive culture for S. marcescens from any sample during the study period. The case was included once if it had repeated cultures, and the infection episode was included if it had colonization before infection. Controls were randomly selected from those neonates who were admitted in the same period and had no positive cultures for S. marcescens from both clinical and screening samples. The sample size was fixed due to the retrospective design. Given the relatively small number of cases, two controls were utilized to improve the precision of the statistical estimate. Each case of S marcescens was compared to two uninfected controls to identify potential risk factors associated with demographics and clinical care variables. Prematurity was defined as delivery before 37 weeks and 0/7 days of gestation [5]. Procedures included echocardiography and ultrasound as they were considered a possible source of transmission of micro-organisms. The acquisition was related to the refereeing hospitals if the cases had a positive culture for S. marcescens within 48 hours of admission, while Royal hospital-acquired infection/ colonization was defined as a positive culture after 48 hours of admission. Colonization is defined as a positive culture for Serratia marcescens in the absence of symptoms or signs of infection, and the neonate was not treated with any antibiotics. Infection was defined as a positive culture for S. marcescens, and signs and or symptoms of infection were present, and the neonate was treated with antibiotics. Mortality was defined as all causes of death within 30 days of a positive S. marcescens culture. Annual incidence proportion was calculated as the total number of positive cases divided by the total number of admitted cases in a year times 100. The annual incidence density was calculated as the total number of positive cases divided by total patient days in a year times 1000.
Statistical Analysis
Collected data were analyzed using IBM SPSS Statistics 28.0. Continuous variables were presented as mean, median, and standard deviation, whereas categorical variables, were presented as frequency and percentage. The comparison of means between the two groups was assessed by using an unpaired t-test. The association between two categorical variables was assessed using a chi-square test (Fisher’s exact/ Likelihood ratio). A multivariate binary logistic regression analysis was performed to determine the independent predictors of Serratia marcescens and mortality among Serratia marcescens infected patients. The Odds Ratio (OR) was reported with its 95% CI. A P-value less than 0.05 were considered statistically significant.
Result
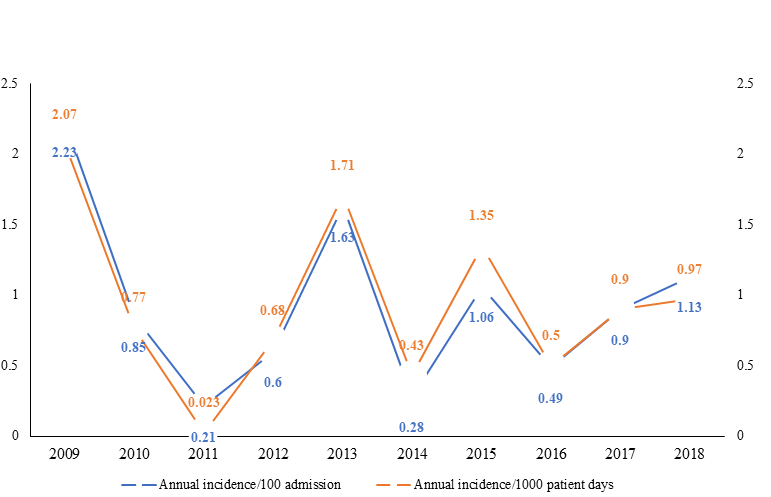
A total of 93 cases had a positive culture of S. marcescens in neonates hospitalized in the NICU during the study period, and 201 controls were included. 50.5% (n=47) of cases were male and 49.5% (n=46) were females. The annual incidence proportion fluctuated from the highest incidence of 2.23 per
100 admissions in 2009 to the lowest incidence of 0.21 per 100 admissions in 2011. The incidence density per 1000 patients’ days ranged between 2.07 and 0.23, as shown in Figure 1.
During the study period, there were a total of 36 neonatal deaths among cases and controls. The overall mortality was higher among infected patients, 17.2% (n=16) vs 10.0% (n=20) in the control group. The median time from detection of S. marcescens to discharge from the hospital is 22 (range 8.25 to 41) days. Regarding predictors of mortality from S. Variable Serratia marcescens p-value Gender Birth weight <1.5 kg 61 (30.5) 42 (46.7) Gestational age marcescens infection, univariate analysis showed that female gender (P=0.030) and mechanical ventilation (P= 0.025) were significant, and in multivariate analysis, only female gender was significant ((OR= 6.741, 95% CI= 1.307-34.767, P= 0.023) as shown in Table 1.
Adjusted Odds Ratio (OR)
$$ \begin{array}{l l l l l l l} \text {Serratia marcescens} & & \text {p - value} & \text {Adjusted Odds Ratio (OR)} & \text {95% CI for OR} & \text {P - value} \\ \text {Negative (n=201)} & \text {Positive (n=93)} & & \text {Lower} & \text {Upper} & \end{array} $$ Male (Reference) 119 (59.5) 47 (50.5) 0.165 1.02 3.801 0.044* Female 81 (40.5) 46 (49.5) 1.969
0.011* 1.498 0.634 3.54 0.357 ≥1.5 kg (Reference) 139 (69.5) 48 (53.3)
| Term birth (Reference) | 94 (46.8) | 25 (27.2) | 0.002* | 1.156 | 6.167 | 0.021* | |
|---|---|---|---|---|---|---|---|
| Premature birth | 107 (53.2) | 67 (72.8) | 2.67 | ||||
| Mode of delivery | |||||||
| Vaginal Delivery (Reference) | 112 (56.9) | 26 (28.9) | 0.0001* | 1.591 | 6.591 | 0.001* | |
| Cesarean-section | 85 (43.1) | 64 (71.1) | 3.238 | ||||
| Catheter | |||||||
| No (Reference) | 153 (76.1) | 79 (84.9) | 0.092 | 0.282 | 1.985 | 0.561 | |
| Yes | 48 (23.9) | 14 (15.1) | 0.749 | ||||
| Central line | |||||||
| Yes (Reference) | 119 (59.5) | 33 (35.5) | 0.0001* | 0.951 | 5.376 | 0.065 | |
| No | 81 (40.5) | 60 (64.5) | 2.261 | ||||
| Procedures | |||||||
| Yes (Reference) | 142 (71.7) | 70 (75.3) | 0.574 | 0.215 | 1.079 | 0.076 | |
| No | 56 (28.3) | 23 (24.7) | 0.482 | ||||
| Mechanical ventilation | |||||||
| Yes (Reference) | 144 (73.5) | 58 (62.4) | 0.074 | 0.606 | 3.495 | 0.401 | |
| No | 52 (26.5) | 35 (37.6) | 1.455 | ||||
| Type of feeding | |||||||
| Total Parenteral Nutrition TPN (Reference) | 60 (30.0) | 18 (19.4) | 0.0001* | ||||
| Enteral | 38 (19.0) | 37 (39.8) | 3.993 | 1.599 | 9.968 | 0.003* | |
| Breast Milk (BM) | 25 (12.5) | 16 (17.2) | 4.73 | 1.512 | 14.799 | 0.008* | |
| Nil Per Os (NPO) | 10 (5.0) | 8 (8.6) | 4.777 | 1.243 | 18.358 | 0.023* | |
| TPN + Enteral | 62 (31.0) | 5 (5.4) | 0.311 | 0.102 | 0.951 | 0.041* | |
| TPN + BM | 5 (2.5) | 9 (9.7) | 9.905 | 2.167 | 45.275 | 0.003* | |
| Surgery | |||||||
| No (Reference) | 122 (61.3) | 61 (65.6) | 0.518 | 1.546 | 8.946 | 0.003* | |
| Yes | 77 (38.7) | 32 (34.4) | 3.719 | ||||
| Antibiotics | |||||||
| Received (Reference) | 175 (87.1) | 90 (96.8) | 0.010* | 0.061 | 1.066 | 0.061 | |
| Not received | 26 (12.9) | 3 (3.2) | 0.255 |
Table 1: Univariate and multivariate analysis to determine the independent predictors of Serratia marcescens infection.
Statistically significant Table 1: Univariate and multivariate analysis to determine the independent predictors of Serratia marcescens infection.
There were significant differences between cases and controls for the acquisition of S. marcescens in birth weight (46.7% of those who had S. marcescens had a birth weight < 1.5 kg (P=0.001), premature births (P= 0.002) and born by cesarean section (P=0.0001) and had a central line (P=0.0001). All types of feeding were significant, and exposure to antibiotics was also significant (P=0.010), as shown in (Table 2). At the time of infection, 28.7% of infants were mechanically ventilated, > 50% received Total parenteral nutrition (TPN) and (21.7%) had a central venous catheter.
<1.5 kg 33 (78.6) 9 (21.4) 0.422 0.761 0.1 5.779 0.791 ≥1.5 kg (Reference) 41 (85.4) 7 (14.6) Gestational age Term birth (Reference) 21 (84.0) 4 (16.0) 1 Premature birth 55 (82.1) 12 (17.9) 0.872 0.083 9.179 0.909 Mode of delivery Vaginal Delivery (Reference) 21 (80.8) 5 (19.2) 0.757 Cesarean-section 54 (84.4) 10 (15.6) 1.156 0.223 6.003 0.863 Catheter No (Reference) 66 (83.5) 13 (16.5) 0.703 Yes 11 (78.6) 3 (21.4) 2.553 0.261 24.921 0.42 Central line Yes (Reference) 26 (78.8) 7 (21.2) 0.567 No 51 (85.0) 9 (15.0) 1.252 0.216 7.266 0.802 Procedures Yes (Reference) 55 (78.6) 15 (21.4) 0.107 No 22 (95.7) 1 (4.3) 0.339 0.029 3.989 0.39 Mechanical ventilation Yes (Reference) 44 (75.9) 14 (24.1) 0.025* No 33 (94.3) 2 (5.7) 0.172 0.024 1.219 0.078 Type of feeding Total Parenteral Nutrition TPN (Reference) 13 (72.2) 5 (27.8) Variable Mortality
p-value Adjusted Odds
$$ \begin{array}{l l l l l l l} \text {Variable} & \text {Mortality} & \text {p - value} & \text {Adjusted Odds Ratio (OR)} & \text {95% CI for OR} & \text {P - value} \\ & \text {No (n= 77)} & \text {Yes (n= 16)} & \text {Lower} & \text {Upper} \\ \text {Gender} & & & & & \\ \text {Male (Reference)} & 4 3 (9 1. 5) & 4 (8. 5) & \text {0.030} ^ {*} & & \\ \text {Female} & 3 4 (7 3. 9) & 1 2 (2 6. 1) & 6. 7 4 1 & 1. 3 0 7 & 3 4. 7 6 7 \\ \text {Birth weight} & & & & & \\ \end{array} $$ Enteral 30 (81.1) 7 (18.9) 1.146 0.159 8.235 0.892 Breast Milk (BM) 15 (93.8) 1 (6.3) 0.28 0.02 3.998 0.348 Nil Per Os (NPO) 7 (87.5) 1 (12.5) 0.391 0.028 5.509 0.486 TPN + Enteral 5 (100) 0 (0) NE TPN + BM 7 (77.8) 2 (22.2) 0.642 0.074 5.595 0.688 Surgery No (Reference) 50 (82.0) 11 (18.0) 1 Yes 27 (84.4) 5 (15.6) 0.389 0.056 2.71 0.341 Antibiotics Received (Reference) 74 (82.2) 16 (17.8) 1 Not received 3 (100) 0 (0) NE
0.394 *Statistically significant, NE - Not estimated due to non-occurrence of event. Table 2: Univariate and multivariate analysis to determine the independent predictors of mortality among Serratia marcescens infected patients.
Multivariate analysis showed that gender (female neonates, OR= 1.969, 95% CI= 1.020-3.801, P= 0.044), premature birth ((OR= 2.670, 95% CI= 1.156-6.167, P= 0.021). C-section (OR= 3.238, 95% CI= 1.591-6.591, P=
0.001); were independent factors for Serratia acquisition. Regarding the type of feeding, Enteral has four times increased risk of getting Serratia marcescens compared to TPN (OR= 3.993, 95% CI= 1.599-9.968, P= 0.003), whereas BM (OR= 4.730, 95% CI= 1.512-14.799, P= 0.008) and NPO (OR= 4.777, 95% CI= 1.243-18.358, P= 0.023) has five times increased risk of getting Serratia marcescens compared to TPN. The combination of TPN and Enteral has 69% reduced risk of getting Serratia marcescens compared to TPN alone (OR= 0.311, 95% CI= 0.102-0.951, P= 0.041). However, the combination of TPN and BM has a ten times higher risk of getting Serratia marcescens than TPN alone (OR= 9.905, 95% CI= 2.167-45.275, P= 0.003). Patients who underwent surgery have a four times higher risk of getting Serratia marcescens than those who did not (OR= 3.719, 95% CI= 1.546-8.946, P= 0.003).
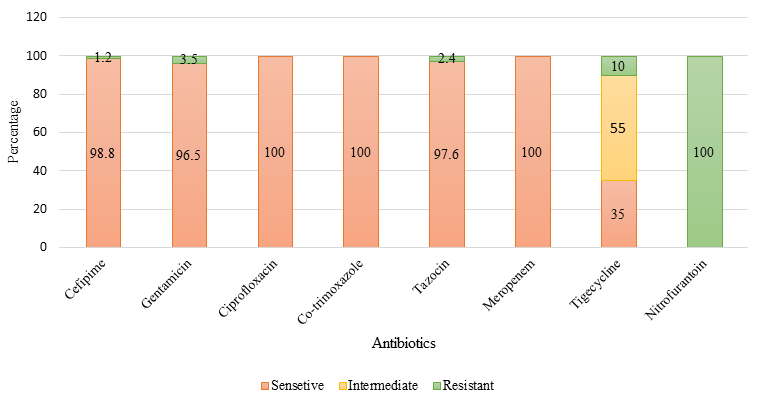
Bacteremia was the commonest infection 38.7% (n=36) followed by conjunctivitis 29.0% (n=27). 15 (16.1%) cases had colonization, and 4 (4.3%) cases had wound infection. Meningitis, pneumonia, and urinary tract infection were 1 (1.1%) each. 87% (n=81) of cases were acquired in our hospital, while 13% (n=12) were acquired in other hospitals. 13 (14%) cases had colonization of S. marcescens before infection as shown in (Table 3). All tested S. marcescens isolates were resistant to ampicillin and amoxicillin/clavulanate, and all were susceptible to ciprofloxacin, co-trimoxazole and meropenem of the tested isolates: 1.2% were resistant to cefepime, 3.5 % were resistant to gentamicin, 2.4 % resistant to tazocin and 10 % resistant to tigecycline. One S. marcescens isolated from urine tested resistant to nitrofurantoin (Figure 2).
| n (%) | ||
|---|---|---|
| Type of positive Sample | blood | 36 (38.7) |
| CSF | 1 (1.1) | |
| ET | 10 (10.8) | |
| eye | 27 (29.0) | |
| Peritoneal fluid | 1 (1.1) | |
| pleural fluid | 1 (1.1) | |
| screen | 5 (5.4) | |
| sputum | 5 (5.4) | |
| urine | 2 (2.2) | |
| wound | 5 (5.4) | |
| Type of Infection | VAP | 8 (8.6) |
| Bacteremia | 36 (38.7) | |
| GU | 1 (1.1) | |
| Eye infection | 27 (29.0) | |
| Wound infection | 4 (4.3) | |
| colonization | 15 (16.1) | |
| Meningitis | 1 (1.1) | |
| pneumonia | 1 (1.1) | |
| colonization before infection | Yes | 13 (14.0) |
| No | 80 (86.0) | |
| Type of Acquisition | Royal Hospital | 81 (87.0) |
| Other hospitals | 12 (13.0) | |
| Detection of S. marcescens from > 1 site | Yes | 18 (19.4) |
| No | 75 (80.6) |
Table 2: Microbiology of _S. marcescens_ cases.
Discussion
Most of the epidemiology of S. marcescens among neonates are described in the literature is from outbreak settings [6, 7, 8, 9, 10, 11]. Our study highlighted the epidemiology for a ten-year period. The annual incidence and incidence proportion were fluctuating over the years due to occurrence of outbreaks throughout the study period that were ultimately controlled. In a recently reported outbreak, no source was identified [6].
The mortality rate in this study was high as reported by M. Luisa and colleagues that mortality due to S. marcescens infections can vary markedly and range from 0 to 45% [10].
In newborns, the main risk factors for the acquisition of Serratia infection are: immaturity of the immune system and low birth weight (<1500 g) in preterm newborns, length of stay, and the use of antibiotics. (10) In our study the significant risk factors were female gender, C-section, all types of feeding including newborn who are NPO and neonates who had surgery. All these might indicate more handling and care is given to those neonates with element of breaches or non-compliance to infection prevention and control practices during care delivery some of which were highlighted previously. (6) S. marcescens colonizes the preterm infant gut within the first days after birth, following a colonization pattern very similar to that observed in other members of the Family Enterobacteriaceae. Moles et al. found 69% of the infants were colonized by S. marcescens at least in a sampling time during the studied period. The colonization rate increased to ~ 75% when only infants born at < 30 gestational weeks and < 1500 g were considered [11]. The most frequent site of infection in our cohort, as reported in other literature, was bloodstream infection however, conjunctivitis was the second most common.
A few limitations were observed in this report including the study was retrospective in nature and was conducted in one center only which might affect the generalizability of the results. The data for rate of colonization might underestimate as our hospital does not a stable active screening for S. marcescens protocol in the NICU. In addition, we could not do sub analysis for bacteremia as we did not study non-S. Marcescens bacteremia among the controls. The strength of this work is that S. marcescens was studied for 10-year periods and the only one of its kind in the country.
Conclusion
S. marcescens is an important nosocomial pathogen, especially in NICUs, that has a propensity to cause difficult- to-control outbreaks. Healthcare workers’ awareness of this organism and enhancement of infection prevention and control measures is a vital requirement to prevent HAIs among susceptible neonates.
References
-
Gastmeier P, Loui A, Stamm-Balderjahn S, Hansen S, Zuschneid I, et al. (2007) Outbreaks in neonatal intensive care units - they are not like others. Am J Infect Control 35(3): 172-176.
-
Polilli E, Parruti G, Fazii P, D’Antonio D, Palmieri D, et al. (2011) Rapidly controlled outbreak of Serratia marcescens infection/colonisations in a neonatal intensive care unit, Pescara General Hospital, Pescara, Italy, April 2011. Euro Surveill 16(24): 19892.
-
Gransden WR, Webster M, French GL, Phillips I (1986) An outbreak of Serratia marcescens transmitted by contaminated breast pumps in a special care baby unit. J Hosp Infect 7(2): 149-154.
-
Madani TA, Alsaedi S, James L, Eldeek BS, Jiman-Fatani AA, et al. (2011) Serratia marcescens-contaminated baby shampoo causing an outbreak among newborns at King Abdulaziz University Hospital, Jeddah, Saudi Arabia. J Hosp Infect 78(1): 16-19.
-
CDC Grand Rounds: Public Health Strategies to Prevent Preterm Birth. MMWR 65(32): 826-830.
-
Al Maskari Z, Al Hinnai M, Al Ghabshi L, Panchatcharam SM, Al Rashdi A, et al. (2022) Rapid Control of Serratia marcescens Outbreak in Neonatal Intensive Care Unit, Oman. Infect Dis Diag Treat 6: 191.
-
Dessì A, Puddu M, Testa M, Marcialis MA, Pintus MC, et al. (2009) Serratia marcescens Infections and Outbreaks in Neonatal Intensive Care Units. J Chemother 21(5): 493- 499.
-
Maltezou HC, Tryfinopoulou K, Katerelos P, Ftika L, Pappa O, et al. (2012) Consecutive Serratia marcescens multiclone outbreaks in a neonatal intensive care unit. Am J Infect Control 40(7): 637-642.
-
Adamson V, Mitt P, Pisarev H, Metsvaht T, Telling K, et al. (2012) Prolonged outbreak of Serratia marcescens in Tartu University Hospital: a case-control study. BMC Infect Dis 12: 281.
-
Cristina ML, Sartini M, Spagnolo AM (2019) Serratia marcescens Infections in Neonatal Intensive Care Units (NICUs). Int J Environ Res Public Health 16(4): 610.
-
Moles L, Gómez M, Moroder E, Jiménez E, Escuder D, et al. (2019) Serratia marcescens colonization in preterm neonates during their neonatal intensive care unit stay. Antimicrob Resist Infect Control 8: 135.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia