Investigation of Epidemiology and Clinical Characteristics of Patients with Enterocutaneous Fistula in China
Purpose: To investigate the epidemiology and characteristics of patients with enterocutaneous fistulas in our hospital. Methods: A single-center study was conducted in our hospital to collect data on patients with ECFs from November 27, 2013 to December 31, 2019. These data included patients’ general information, common diseases and conditions, characteristics, treatments, and outcomes. Results: Patients (N = 218) with enterocutaneous fistulas were enrolled in the study, including 152 males and 66 females (median age: 52 years). Changsha city had the largest number of patients (39.9%), 79.8% of cases had a single enterocutaneous fistula and 92.2% were related to surgeries. Gastrointestinal tumor (25.7%) was the most common primary disease, and small intestine fistula (44.0%) was the most common enterocutaneous fistula. Approximately 51.8% of patients visited tertiary hospitals first and only 22.5% received definitive surgery. However, only 57.3% of patients were cured, which was related to their first-visited hospital (p = 0.039) and undergoing definitive surgery (p = 0.024). The time from the operation to the enterocutaneous fistula diagnosis for 40.0% of patients was within 1 week after the initial operation, and the length of stay for the first hospitalization of 90.8% was one week to half a year. Some patients had complications, such as diabetes (10.1%). Our analysis showed a significant association of malnutrition with cure rate (p = 0.013). Conclusion: The cure rates of enterocutaneous fistulas were associated with the first visited hospital, definitive surgical treatment, and malnutrition.
Key Summary Points
Why Carry out This Study?
Enterocutaneous fistula (ECF) is a serious complication of gastrointestinal surgery. The purpose of this study was to understand the clinical characteristics and treatment of ECFs in our hospital, and to identify high-risk factors influencing the prognosis of patients with ECFs.
What was learned from This Study?
Firstly, we can understand the epidemiological characteristics of enterocutaneous fistula (ECF). Secondly, we can learn some treatment methods to deal with ECFs.
Introduction
A fistula is an abnormal communication between two epithelial surfaces. It often starts from an offending side and makes its way to an adjacent surface. A digestive tract fistula can originate anywhere in the digestive tract, such as the mouth, esophagus, stomach, duodenum, small intestine, colon, rectum, or anal canal [1]. Digestive tract fistulas include external and internal fistulas. External fistulas penetrate the abdominal wall and communicate with the outside world, and internal fistulas connect with other cavity organs. However, internal and external fistulas can also co- exist [2].
An enterocutaneous fistula (ECF) is one of the most common and serious fistulas. It refers to an abnormal passage between the gastrointestinal tract and other hollow organs, body cavities, or outside the body, through which gastrointestinal contents enter other organs, body cavities, or outside the body, causing a series of pathophysiological changes, such as infection, fluid loss, malnutrition, and organ dysfunction. Enterocutaneous, enterenteric, enterovesical, enterocolic, enteroatmospheric, and rectovaginal fistulas are the most frequent fistulas [3, 4, 5]. ECFs are usually caused by underlying diseases and surgical procedures [6]. Therefore, they are considered a complication rather than a distinct disease [7, 8, 9]. Surgical complications are the most common cause of intestinal fistula formation [10, 11]. Except for surgical events, the common causes of ECFs are diverticular disease, Crohn’s disease, malignancy, radiation, non-surgical injuries, and foreign bodies [10, 12, 13, 14, 15, 16, 17]. A fistula’s etiology should be confirmed before planning treatment. It is important to define the cause of an ECF to develop a treatment plan for it. Treatment of an ECF involves treatment of the fistula itself and its underlying disease. Although the outcomes of therapeutic treatments have improved significantly, in general, the mortality of patients with ECFs remains high. The purpose of this study was to understand the clinical characteristics and treatment of ECFs in our hospital and to identify high-risk factors influencing the prognosis of patients with ECFs, to improve their treatment outcomes.
Methods
Patients
This was a retrospective study performed at Hunan Provincial People’s Hospital. Patients diagnosed with ECFs, who were admitted to the Department of Gastrointestinal Surgery of our hospital from November 27, 2013 to December 31, 2019, were screened for potential recruitment. We only evaluated the data from the patients’ first admission. The Hunan Provincial People’s Hospital Institutional Ethical Board approved the use of clinical materials for research purposes (IRB number: 2020-11), and we obtained written informed consent from all the patients.
Content of the Data Collected
We collected data on all of the patients diagnosed with ECFs in our hospital’s department of gastroenterology. Based on clinical manifestations, laboratory examination, imaging data, and intraoperative exploration, the diagnosis of ECF was determined. The doctor in charge was responsible for collecting, recording, and sorting the relevant data of patients with an ECF. Gender, age, common diseases and conditions, primary diseases, causes, length of stay, location and type of the fistula, complications, treatment measures, outcomes, and other information on the patients was recorded. After the data entry was completed, more than three physicians reviewed all of the recorded data.
Statistical Analysis
The statistical software package SPSS (version 20.0; IBM, Armonk, NY, USA) was used for all analyses. The association between the ECF cure rate and the first visited hospital, definitive operation, malnutrition, and other clinical characteristics was analyzed using the Chi-square test. Student’s t-test was used to evaluate significant differences between two groups of data in all of the relevant analyses. The level of statistical significance was set to p < 0.05.
Results
Patients’ General Information
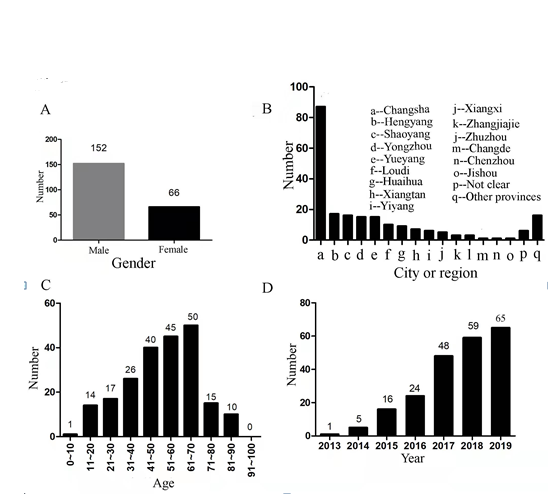
We included 218 patients in the study - 66 females (30.3%) and 152 males (69.7%), with a 1:2.3 ratio of females to males (Figure 1A). Figure 1B shows the regional distribution of the 218 patients with ECF, 84.4% were referred from other hospitals throughout the country. As shown in Figure1B, 39.9% of patients with ECFs came from Changsha, which was the city with the largest number of patients with ECF, followed by Hengyang, Shaoyang, Yongzhou, and other cities or regions. Moreover, 7.3% of patients with ECF came from other provinces, such as Guangdong, Guangxi, and Jiangxi. The age of the patients ranged from 7 to 86 years old, with a median age of 52 years (Figure 1C). Figure 1D shows the patients with ECFs admitted to the hospital each year. Since the first patient was admitted to our hospital for an ECF in 2013, the number of patients admitted with ECFs has increased yearly, and reached 65 cases in 2019. However, it should be noted that we only recorded the data collected on the first hospital admission for patients with ECF, even those with repeated admissions.
Characteristics of the Fistulas
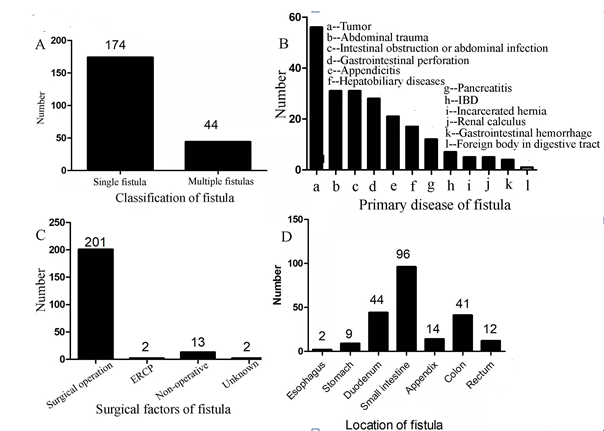
Among the 218 patients with ECFs, 79.8% had single ECFs and 20.2% had multiple ECFs (Figure 2A). The top three primary diseases responsible for ECFs were gastrointestinal tumors (25.7%), abdominal trauma (14.2%), and intestinal obstruction and abdominal infection (14.2%) (Figure 2B). The direct causes of ECFs were mainly surgical procedures (92.2%), followed by non-surgical causes or unknown reasons (6.9%), and endoscopic retrograde cannulation of the pancreas (ERCP) (0.9%) (Figure 2C). Among the patients with ECF, 44.0% had small intestine fistulas, followed by duodenum fistulas (20.2%), colon fistulas (18.8%), appendix fistulas (6.4%), rectum fistulas (5.5%), stomach fistulas (4.1%), and esophageal fistulas (0.9%) (Figure 2D).
Treatment of the Fistulas and Outcomes
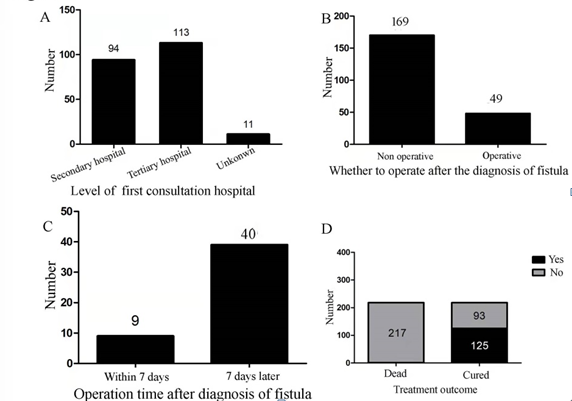
Figure 3A shows the selection of all enrolled patients and the level of hospital for their first visit. Approximately 43.1% of patients visited a secondary care hospital first, and 51.8% visited a tertiary care hospital first. During their hospitalization, 77.5% patients did not receive surgical treatment after being diagnosed with a fistula, while 22.5% of patients received surgical treatment. Moreover, of the 22.5% of patients who received surgical treatment, 18.4% received it within one week after the diagnosis of the fistula, and 81.6% of patients received surgical treatment one week after the diagnosis of the fistula (Figures 3B,3C). Among the 218 patients, 57.3% were cured, 42.2% were not cured, and one (0.5%) died (Figure 3D). The cure rate had a significant association with the level of care of the hospital that the patients visited first (p = 0.039), and the definitive surgical treatment they received after the diagnosis of the fistula (p = 0.024) (Table 1).
Characteristics N Cured Not cured χ2 p Gender
Female 66 44(66.7%) 22(33.3%)
Age (years)
41-70 135 80(59.3%) 55(40.7%)
71-100 25 11(44.0%) 14(56.0%) Classification of fistula(s) Multiple 44 27(61.4%) 17(38.6%) Male 152 81 (53.3%) 71 (46.7%) 3.367 0.067
0-40 58 34(58.6%) 24(41.4%) 2.061 0.357
Single 174 98(56.3%) 76(43.7%) 0.365 0.546
| Hospital’s level of care | |||||
|---|---|---|---|---|---|
| Secondary care | 94 | 60(63.8%) | 34(36.2%) | 4.243 | *0.039 |
| Tertiary care | 113 | 56(49.6%) | 57(50.4%) | ||
| Definitive surgery | |||||
| Yes | 49 | 35(71.4%) | 14(28.6%) | 5.129 | *0.024 |
| No | 169 | 90(53.3%) | 79(46.7%) | ||
| Primary disease | |||||
| Tumor | 56 | 34(60.7%) | 22(39.3%) | 3.781 | 0.151 |
| Trauma | 31 | 22(71.0%) | 9(29.0%) | ||
| Other | 131 | 69(52.7%) | 62(47.3%) | ||
| Location of the fistula | |||||
| Above the intestine | 55 | 26(47.3%) | 29(52.7%) | 3.057 | 0.217 |
| Intestine | 96 | 58(60.4%) | 38(39.6%) | ||
| Below the intestine | 67 | 41(61.2%) | 26(38.8%) | ||
| Diabetes | |||||
| Yes | 22 | 13(59.1%) | 9(40.9%) | 0.022 | 0.882 |
| No | 195 | 112(57.4%) | 83(42.6%) | ||
| Hypertension | |||||
| Yes | 25 | 12(48.0%) | 13(52.0%) | 1.04 | 0.308 |
| No | 189 | 111(58.7%) | 78(41.3%) | ||
| Hypoproteinemia | |||||
| Yes | 24 | 14(58.3%) | 10(41.7%) | 0.012 | 0.912 |
| No | 189 | 108(57.1%) | 81(42.9%) | ||
| Anemia | |||||
| Yes | 27 | 15(55.6%) | 12(44.4%) | 0.082 | 0.774 |
| No | 183 | 107(58.5%) | 76(41.5%) | ||
| Malnutrition | |||||
| Yes | 26 | 9(34.6%) | 17(65.4%) | 6.232 | *0.013 |
| No | 192 | 116(60.4%) | 76(39.6%) | ||
| Crohn’s disease | |||||
| Yes | 8 | 3(37.5%) | 5(62.5%) | 1.336 | 0.248 |
| No | 210 | 122(58.1%) | 88(41.9%) |
Table 1: Relationship between the cure rate and clinical characteristics of patients with enterocutaneous fistulas * p < 0.05.
Amount of Time for the Treatment of the Fistulas
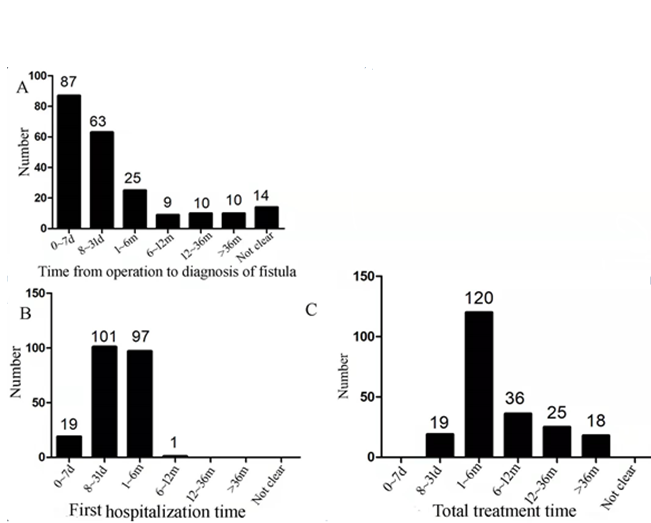
Figure 4A shows the time from the operation to the diagnosis of ECF. Of the 218 patients, 40.0% were diagnosed within 1 week after the initial operation, and 28.9% were diagnosed 8 to 31 days after the initial operation. Therefore, approximately 68.9% of patients with ECFs received a clear- cut diagnosis within 31 days after the initial operation. The length of stay of the first hospitalization for 46.3% of the patients was 8 to 31 days, for 44.5% the length of stay was 1 to 6 months. Therefore, length of stay for the first hospitalization of 90.8% of the patients’ was one week to half a year (Figure 4B). However, the total length of stay for 55.0% of patients was 1-6 months (Figure 4C).
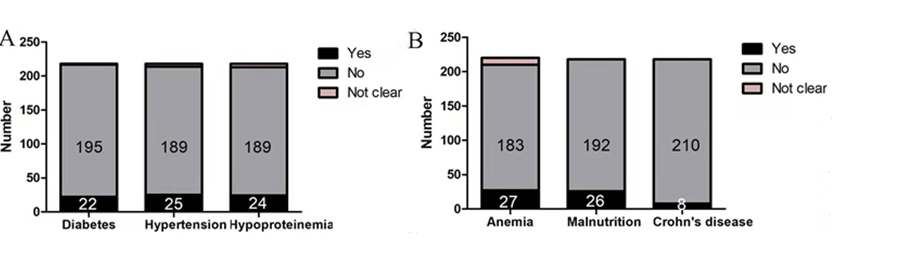
Common Diseases and Conditions of Patients with ECFs
Among the 218 cases with ECFs, there were complications of diabetes (10.1%), hypertension (11.5%), hypoproteinemia (11.0%), anemia (12.4%), malnutrition (11.9%), and other common diseases. Furthermore, 3.7% of patients were found to have Crohn’s disease (Figure 5), and malnutrition was found to be associated with the cure rate of ECFs (p = 0.013) (Table 1).
Discussion
This study analyzed the general demographic characteristics of patients with ECFs. Studies have found that the proportion of male patients among all patients with ECFs is 48.1-72.3% [2, 18, 19, 20, 21]. In this study, approximately 69.7% of the patients with ECFs were male. No significant differences were found in comparisons with the female patients. The median age in this study was 52 years (range: 7-86 years), which was similar to results of other studies [19, 20, 21]. However, we included a 7-year-old ECF patient in our study, which shows that ECF can also occur in children. Approximately 40% of the patients in this study were from Changsha, and the rest were from other cities or regions in China. At the same time, 84.4% of patients were referred from other hospitals throughout the country. More importantly, since the first case of ECF was admitted to our department in 2013, the number of admitted patients has increased annually, reaching 65 cases in 2019.
Our study showed that 79.8% of the patients had a single ECF, which is between the percentages reported in other studies [2, 20]. Moreover, our results showed the main direct cause of ECF was surgical treatment (92.2%), which was higher than other causes [2, 21]. Previous research reported the most common causes of ECFs were malignant tumors (41.2%), gastroenteric ulcers and perforations (13.3%), and trauma (10.3%) [2]. However, our research found that the most common causes were gastroenteric tumors (25.7%), internal obstruction and abdominal infection (14.2%), and abdominal trauma (14.2%). So, it is clear that abdominal tumors and trauma are the main causes of ECFs. Furthermore, a study by Zheng found that the most common types of ECFs were the jejuno-ileal fistula (28.8%), colon fistula (20.6%), and rectal fistula (11.2%) [2]. However, the most common types found in our study were small intestine fistula (44.0%), duodenum fistula (20.2%), and colon fistula (18.8%). There are two reasons for this difference: First, there are different standards for classification of ECFs. In this study, we recorded fistulas between the stomach and the small intestine as gastric fistulas, fistulas between the small intestine and colon as intestinal fistulas, and fistulas between the colon and rectum as colon fistulas. Second, the study’s sample size was small.
As reported in this study, 84.4% of patients were referred from other hospitals throughout the country, 43.1% had visited a secondary care hospital first, and 51.8% had visited a tertiary care hospital first. There were no significant differences between the two groups selected. However, we found that the level of care of the hospital that patients visited first was associated with the cure rate (p = 0.039). This finding can be attributed to two reasons: (1) the patients who had visited a tertiary care hospital first might have done so because their conditions were more serious than those of the other patients; and (2), it is possible that the lymphadenectomies performed in the tertiary care hospitals were more extensive and prone to serious and fatal complications, than those performed in the secondary care hospitals.
In our study, 22.5% of patients received a definitive operation, which was lower than other studies (23.4- 53.2%) [2, 21]. Moreover, 81.6% of patients had received the operation one week after the diagnosis of the fistula, which is consistent with the results of Visschers and Zheng [18, 19]. More importantly, the healing rate was 57.3% for the patients in this study, which is consistent with the results of Quinn (53.8%) [21]. We found that the cure rate was related to having the definitive surgery after the diagnosis of the fistula (p = 0.024) (Table 1). However, surgery is no longer the first choice for patients with intestinal fistulas, given the widespread use of somatostatin, growth hormone, enteral and parenteral nutrition, and negative pressure suction. In addition, proximal enterostomy has improved the healing rate of patients with ECF. Though studies have reported an in-hospital mortality rate of 19.1% and an operative mortality from definitive surgery of 9.8-15.1%, [19, 21] we were unable to assess the mortality rate of patients with ECFs in the present study. First, some patients were discharged or transferred to another hospital before the fistula healed. Second, because of the long treatment period and high costs, it was difficult to conduct outpatient follow-up care. However, one year after treatment for an appendiceal stump fistula in December 2019, a 16-year-old girl suffered from severe abdominal infection, which resulted in rupture of the splenic artery and bleeding, leading to her death. Wu L found that some patients had intra-abdominal bleeding events during hospitalization, and the incidence of intra-abdominal bleeding was 10.6% [22].
Figure 4A shows the time from the operation to the diagnosis of ECF. The time for 40.0% of the patients was within 1 week after the initial operation, and that the time for 28.9% of patients was 8 to 31 days after the initial operation. Martinez and Visschers reported that the median time from the initial surgery to fistula recurrence was 6-21 days (range: 1-494 days) [19, 20]. In our study, approximately 68.9% of patients with ECF received a clear-cut diagnosis within 31 days after the first operation. However, due to inconsistencies in stratification standards, we could not compare our results with the results of Martinez and Visschers [19, 20]. Our study found that the length of stay for the first hospitalization of 90.8% of the patients was one week to half a year. Visschers found that the median period of treatment was 70 days (range: 6-497 days) [19]. However, it was not possible for us to measure the precise length of total treatment for those patients with ECF because some of them received treatment at home.
This study identified patients with complications of diabetes (10.1%), hypertension (11.5%), hypoproteinemia (11.0%), and other common diseases. More importantly, we found a strong relationship between preoperative albumin levels and the cure rate, which is consistent with the results of Visschers [19]. However, no relationship was found between the cure rate and diabetes, hypertension, hypoproteinemia, or anemia. Furthermore, in our study, only 3.2% of the patients had Crohn’s disease, whereas 6-8% of patients in other studies had Crohn’s disease [2, 21, 22].
Conclusion
In our study, we had investigated the epidemiology and clinical characteristics of 218 patients with enterocutaneous fistulas. We found that the cure rates of enterocutaneous fistulas were associated with the first visited hospital, definitive surgical treatment, and malnutrition.
References
-
Farooqi N, Tuma F (2022) Intestinal Fistula. StatPearls Publishing, Treasure Island (FL).
-
Zheng T, Xie HH, Wu XW, Chi Q, Wang F, et al. (2019) Investigation of treatment and analysis of prognostic risk on enterocutaneous fistula in China: a multicenter prospective study. Zhonghua Wei Chang Wai Ke Za Zhi 22(11): 1041-1050.
-
Coccolini F, Ceresoli M, Kluger Y, Kirkpatrick A, Montori G, et al. (2019) Open abdomen and entero-atmospheric fistulae: An interim analysis from the International Register of Open Abdomen (IROA). Injury 50(1): 160- 166.
-
Bhama AR, Schlussel AT (2018) Evaluation and Management of Rectovaginal Fistulas. Dis Colon Rectum 61(1): 21-24.
-
Bensouda A, El Hader K, Sbihi L, Benkabbou A, Karmouni T, et al. (2010) Entero-urinary fistula. Tunis Med 88(11): 814-819.
-
Wadhwani N, Diwakar DK (2018) Localised perforation of locally advanced transverse colon cancer with spontaneous colocutaneous fistula formation: a clinical challenge. BMJ Case Rep 2018: bcr2018224668.
-
Li G, Cheng K, Zhao Z, Wang J, Zhu W, et al. (2018) Treatment of 21 cases of chronic radiation intestinal injury by staging ileostomy and closure operation. Chinese journal of gastrointestinal surgery 21(7): 772- 778.
-
Hamzaoui L, Medhioub M, Ghannei O, Sassi S, Bouzaidi K, et al. (2017) Choledocoduodenal fistula complicating a Crohn’s disease. Presse Med 46(7-8): 782-784.
-
Badic B, Leroux G, Thereaux J, Joumond A, Gancel CH, et al. (2017) Colovesical Fistula Complicating Diverticular Disease: A 14-Year Experience. Surg Laparosc Endosc Percutan Tech 27(2): 94-97.
-
Bakopoulos A, Tsilimigras DI, Syriga M, Koliakos N, Ntomi V, et al. (2018) Diverticulitis of the transverse colon manifesting as colocutaneous fistula. Ann R Coll Surg Engl 100(8): e1-e3.
-
Martinolich J, Croasdale DR, Bhakta AS, Ata A, Chismark AD, et al. (2019) Laparoscopic Surgery for Diverticular Fistulas: Outcomes of 111 Consecutive Cases at a Single Institution. J Gastrointest Surg 23(5): 1015-1021.
-
Shaydakov ME, Pastorino A, Tuma F (2022) Enterovesical Fistula. StatPearls Publishing, Treasure Island (FL).
-
Bessi G, Siproudhis L, Merlini l’Héritier A, Wallenhorst T, Le Balc’h E, et al. (2019) Advancement flap procedure in Crohn and non-Crohn perineal fistulas: a simple surgical approach. Colorectal Dis 21(1): 66-72.
-
Huttenhuis JM, Kouwenhoven EA, van Zanten RA, Veneman TF (2015) Malignant Gastrocolic Fistula: Review of the Literature and Report of a Case. Acta Chir Belg 115(6): 423-425.
-
Iwamuro M, Hasegawa K, Hanayama Y, Kataoka H, Tanaka T, et al. (2018) Enterovaginal and colovesical fistulas as late complications of pelvic radiotherapy. J Gen Fam Med 19(5): 166-169.
-
Yanai K, Ueda Y, Minato S, Kaneko S, Mutsuyoshi Y, et al. (2018) Delayed peritoneal dialysis catheter-intestinal fistula. Nephrology (Carlton) 23(9): 890-891.
-
Barat M, Hoeffel C, Bouquot M, Jannot AS, Dautry R, et al. (2019) Preoperative evaluation of small bowel complications in Crohn’s disease: comparison of diffusion-weighted and contrast-enhanced MR imaging. Eur Radiol 29(4): 2034-2044.
-
Yao Z, Tian W, Xu X, Zhao R, Huang M, et al. (2021) The Double-Lumen Irrigation-Suction Tube in The Management of Incisional Surgical Site Infection After Enterocutaneous Fistula Excisions: An Observational Study. J Invest Surg 34(7): 791-797.
-
Visschers RG, Olde Damink SW, Winkens B, Soeters PB, van Gemert WG et al. (2008) Treatment strategies in 135 consecutive patients with enterocutaneous fistulas. World J Surg 32(3): 445-453.
-
Martinez JL, Bosco-Garate I, Souza-Gallardo LM, Méndez JD, Juárez-Oropeza MA, et al. (2020) Effect of Preoperative Administration of Oral Arginine and Glutamine in Patients with Enterocutaneous Fistula Submitted to Definitive Surgery: a Prospective Randomized Trial. J Gastrointest Surg 24(2): 426-434.
-
Quinn M, Falconer S, McKee RF (2017) Management of Enterocutaneous Fistula: Outcomes in 276 Patients. World J Surg 41(10): 2502-2511.
-
Wu L, Ren J, Liu Q, Wang G, Wu X, et al. (2016) Risk factor and outcome for intra-abdominal bleeding in patients with enterocutaneous fistula. Medicine 95(47): e5369.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia