Prevalence of Staphylococcus aureus on Noncritical Surfaces of the Laboratories of a Medical Laboratory Training Institution
Staphylococcus aureus is a Gram positive bacterium that is frequently encountered on surfaces such as benches and skin. This organism being a normal flora of the skin is usually nonpathogenic but becomes pathogenic when found outside its normal flora where it can cause varying number of infections such as nosocomial infections and sepsis which may even lead to death if left untreated. This research was therefore carried out to determine the prevalence of Staphylococcus aureus on noncritical surface areas including: Furniture, Doors and Windows of the laboratories of Federal College of Medical Laboratory Science & Technology Jos, Nigeria. Samples were processed, examined and analyzed accordingly. It was observed that out of the 120 samples examined, 8 were gram positive cocci in clusters under Gram staining examination Coagulase and catalase tests were positive indicating specific biochemical tests to identify the organisms in the 8 organisms as Stapylococcus aureus showing a prevalence rate of 6.67%. The 17 working Benches examined, 3(2.50%) were positive. Out of 75 Chairs examined, 5(4.17%) were positive. The 18 Windows examined, 10 Doors examined showed no growth for Staphylococcus aureus. Distribution according to laboratory sections showed that, out of the 95 samples in main laboratory, 6(5.00%) were positive. Out of the 14 samples examined in side laboratory one, 2(1.67%) were positive while none 0(0.0%) was positive out of 11 samples examined in side laboratory two. The isolation of Stapylococcus aureus from these locations stresses the urgent need for public enlightenment campaigns by the appropriate authorities to educate the laboratory workers as well as the masses on the etiological agents, the possible risk factors, routes of transmission and health implication of Stapylococcus aureus infection and ways of preventing these bacteria in the Laboratories especially in Federal College of Medical Laboratory Science and Technology Jos Nigeria.
Introduction
In healthcare certain, noncritical surfaces are the areas that come in contact with hands of patients or healthcare professionals who have been exposed to infected patients. Noncritical surfaces are at the center of continuous transmission and spread of nosocomial pathogens. The knowledge of such issues in healthcare environment informs patients, patients’ relatives and caregivers an ample opportunity to ensure disinfection, sterilization and maintenance of hygiene so as to prevent nosocomial infections [1]. Noncritical areas abound in various health environments ranging from clinics to laboratories. Staphylococcus aureus is a Gram positive cocci and aerobe that has been implicated in most nosocomial infection. Although a normal flora of the skin, Staphylococcus aureus when opportune causes many infections [2]. Microscopic morphology of S. aureus cells are Gram-positive and appear in spherical shape. They are often in clusters resembling bunch of grapes when observed under light microscope after Gram staining. It is versatile human pathogen responsible for nosocomial and community- associated infection and associated with high morbidity and mortality rates [3]. In the developing world, mortality associated with severe Staphylococcus aureus infections far exceeds that in developed countries [4]. Emerging reports revealed that Staphylococcus aureus infections have continued to rise in health care facilities increasing the rate of hospital acquired infections with increased emergence of strains resistant to Methicillin called Methicillin Resistant Staphylococcus aureus (MRSA). MRSA infection has resulted in prolonged hospital stay, increased medical expenses and difficulty in patient treatment and management [4].
The unique characteristic of MRSA strains is the multidrug resistance pattern to β-lactam and other classes, due to acquisition of mecA gene, key genetic determinant located on the Staphylococcal cassette chromosome (SCCmec). The mecA gene, encodes the PBP2a an inducible 75b PBP responsible for low-affinity to β-lactam and other drugs [5]. Recent reports from Nigeria have indicated that the prevalence of hospital-associated MRSA varies in health care institutions. Also, a number of investigations have reported that Staphylococcus aureus is among the most frequently encountered bacterial species in microbiology laboratories in Nigeria [6]. For effective treatment of Staphylococcus aureus infections, adequate information and data on susceptibility patterns and characterization of the organism are of great importance [6]. However, available data are relatively limited in this locality when compared to information from other parts of the world.
The statement of problem leading to this study is that Staphylococcus aureus is one of the leading causes of skin and soft tissue infections such as abscesses (boils), furuncles, and cellulitis. Although most staph infections are not serious, S. aureus can cause serious infections such as bloodstream infections (sepsis), pneumonia, or bone and joint infections.
The study is justified by the fact that many hospitals and laboratories in Nigeria have reported many diseases such as boils, furuncles and cellulitis caused by Staphylococcus aureus [3] and many MRSA bacteria isolated from noncritical surfaces [1]. Notably, limited numbers of studies have been conducted in this area, therefore, the findings of this research will be documented for future reference. The findings of this study may also aid in creating awareness to the Staff, Students and to the general public on the route and danger of this infection.
The findings may also be used by health authorities to better target preventive measures and enhance access to at least basic sanitation and regular disinfection of laboratories including training institutions laboratories. Studies abound in Clinics, Hospitals and diagnostic Laboratories but not noticeable among medical laboratory training institutions especially in Nigeria. This study therefore was aimed at determining the prevalence of Staphylococcus aureus on noncritical surfaces of laboratories in a teaching institution including Benches, chairs, Doors and Windows in Federal College of Medical Laboratory Science & Technology, Jos Nigeria.
Materials and Methods
The study was conducted in Federal College of Medical Laboratory Science & Technology Jos, Nigeria in the training and Research laboratories. The study was carried out between May and July 2022. The sample size was based on the numbers of Benches, Chairs, Windows, and Doors present in the laboratories. Main Laboratory has 8 Benches, 67 Chairs, 12 Windows and 8 Doors, Side laboratory One has 5 Benches, 5 Chairs, 3 Windows and 1 Door, Side laboratory Two has 4 Benches, 3 Chairs, 3 Windows and 1 Door. Therefore, a total of 120 Samples were examined. A verbal consent was obtained from head of the main Laboratory, and the side laboratories respectively before using the laboratories Samples were collected from different locations using sterile swap sticks, and each sample was labeled properly and was transported to the appropriate bench for culturing. The preparation of Blood Agar and Chocolate Agar was done according to the procedures highlighted by Ochie & Kolhatka [7] followed by inoculation and culturing (incubation). After incubation at 37°C for 24 hr, the morphological and appearances examination of cultured plates as described by Cruick, et al. [8] which include: color, shape, size, edge, pigmentation, consistency, opacity and fermentation of lactose and mannitol on the media were noted. Preparation of Smear and Gram Staining Techniques were done in line with Ochie & Kolhatka [7] followed by Biochemical tests were used for the identifications of Staphylococcus aureus based on the differences in the biochemical activities of the bacteria especially with Catalase Test and Coagulase Test according to method described by Ryan, et al. [9]. All data obtained from this research were analyzed statistically using percentage prevalence method.
Results
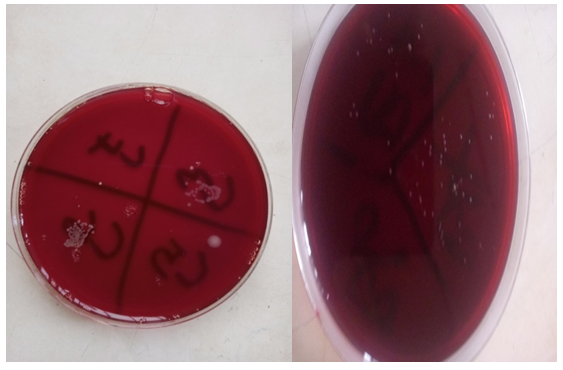
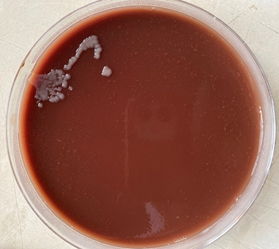
It was observed that out of the 120 samples examined, 8 were gram positive cocci in clusters. Specific biochemical tests were used to identify the organisms, and the 8 organisms were Stapylococcus aureus with a prevalence rate of 6.67%.
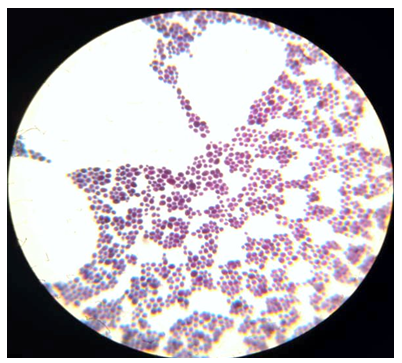
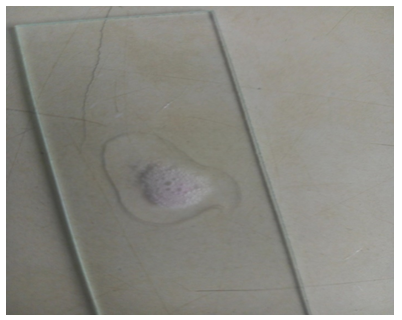
The Tables 1-5 shows the nitty-gritty of the results with the Figures 1-3 showing Growths of Stapylococcus aureus, Gram positive cocci under the microscope (X100) and Coagulase positive results respectively.
| No. Examined | No. Negative | No. Positive | Percentage Positive (%) | |
|---|---|---|---|---|
| Benches | 17 | 14 | 3 | 2.5 |
| Chairs | 75 | 73 | 5 | 4.17 |
| Windows | 18 | 17 | 0 | 0 |
| Doors | 10 | 8 | 0 | 0 |
| Total | 120 | 112 | 8 | 6.67 |
Table 1: Distribution of Staphylococcus aureus in the Laboratories.
| Laboratories | No. Examined | No. Negative | No. Positive | Percentage Positive (%) |
|---|---|---|---|---|
| Main Laboratory | 95 | 69 | 6 | 5 |
| Side Laboratory one | 14 | 12 | 2 | 1.67 |
| Side Laboratory two | 11 | 11 | 0 | 0 |
| Total | 120 | 112 | 8 | 6.67 |
Table 2: Distribution of Staphylococcus aureus in Relation to Laboratory Sections.
| Noncritical Surfaces | No. Examined | No. Negativity | No. Positive | Prevalence (%) | |
|---|---|---|---|---|---|
| Benches | 17 | 14 | 3 | 2.5 | |
| Chairs | 75 | 70 | 5 | 4.17 | |
| windows | 18 | 18 | 0 | 0 | |
| Doors | 10 | 10 | 0 | 0 | |
| Total | 120 | 112 | 8 | 6.67 |
Table 3: Result of the Gram Stain of the Colonies.
| Noncritical Surfaces | No. Examined | No. Negative | No. Positive | Prevalence (%) |
|---|---|---|---|---|
| Benches | 17 | 14 | 3 | 2.5 |
| Chairs | 75 | 70 | 5 | 4.17 |
| windows | 18 | 18 | 0 | 0 |
| Doors | 10 | 10 | 0 | 0 |
| Total | 120 | 112 | 8 | 6.67 |
Table 4: Results of Catalase Test.
| Noncritical Surfaces | No Examined | No. Negative | No. Positive | Prevalence(%) |
|---|---|---|---|---|
| Benches | 17 | 14 | 3 | 2.5 |
| Chairs | 75 | 70 | 5 | 4.17 |
| Windows | 18 | 18 | 0 | 0 |
| Doors | 10 | 10 | 0 | 0 |
| Total | 120 | 112 | 8 | 6.67 |
Table 5: Results of Coagulase Test.
Discussion
Staphylococcus aures being a bacterium that causes germs mostly on noncritical surfaces was isolated from such areas in the laboratories of Federal College of Medical Laboratory Science & Technology Jos, though with a lower prevalence rate of 6.67%. This prevalence obtained from this research is lower when compared to the work of Uzomoh, et al. [10], who documented the prevalence rate of 12.5%. This may be due to different time of study of the researchers. It can equally be attributed to the fact that the hygiene of the laboratory might have increased especially in the training institution under study. Agbo, et al. [1] and Amare, et al. [11] in their studies identified such MRSA from noncritical and inanimate surfaces of hospitals closer to patients and not medical laboratory area.
The isolation Staphylococcus aureus from the laboratory should not be surprised since the laboratory is used frequently by laboratory personnel, lecturers and students, and as a result of this, the bacteria can easily be distributed on Benches, laboratory Doors, Seats and other noncritical areas. Though the laboratory is cleaned and sterilised always, a single table or seat that is left un-cleaned or disinfected can lead to the contamination of others according to Chambers, et al. [12].
It was discovered also that Staphylococcus aureus was isolated from working Chairs (seats) more than the working benches. This though in Laboratory chairs is just like the work of Amare, et al. [11] that showed high prevalence of bacteria in chairs in the hospital studied. This could be attributed to the fact that the Benches are always disinfected and cleaned with less emphasis on the chairs after use. Samples are kept on Benches to be examined always and some of those samples might have been contaminated by Staphylococcus aureus and even other pathogens. According to Joseph [13], the isolation of Staphylococcus aureus from hospital surfaces such as working Benches and Chairs is a clear indication that the professionals needs strict compliance to infections control than allowing only the cleaners to concentrates more in cleaning and disinfecting the floors, giving less attention to the working Benches and Chairs which lead to the build up of Staphylococcus aureus infections on various surfaces. The laboratory personnel and students on the other hand during practicals distribute these bacteria to other places especially on the seats. It is therefore advised that preventive measures such as improved personal hygiene and regular cleaning and disinfection of the Laboratory Chairs and Benches are highly recommended to avoid the tendency for the bacteria to be present in every laboratory noncritical surfaces and laboratory equipment since there are students and Staff using the same laboratory and equipment.Several studies [14, 15, 16, 17] on Staphylococcus aureus infections provides direction towards the epidemiology, infectivity and susceptibility with regards to Staphylococcus aureus therefore more attention should be given to disinfection in medical laboratory surfaces. The study is limited by the fact that Only Stapylococcus aureus was the organism of interest in this study due to logistics and financial challenge.
Conclusion
The isolation of Stapylococcus aureus from the furniture of the laboratory is dangerous to both the Staff and Students as these contaminants have the ability to cause diseases, ranging from food poisoning, to cellulitis, fever, nausea, and diarrhea or to a more dangerous infections. Though the prevalence of 6.67% obtained in this study is low, the safety of the laboratory should not be taken for granted because the isolation of Staphylococcus aurous from these locations shows that the laboratory needs to be cleaned and disinfect regularly to maintain a healthy working environment for both staff and students of the College. This therefore stresses the urgent need for public enlightenment campaigns by the appropriate authorities to educate the laboratory worker as well as the masses on the etiological agents, the possible risk factors, routes of transmission and health implication of Stapylococcus aureus as well as ways of preventing and control of these bacteria in the Laboratories. The authors hereby recommend that:
- Students and Staff involved the Laboratories should be made aware of the possible risk factors associated with Stapylococcus aureus and the health implications.
- The management of the College should intensify efforts to implement the quality of the Laboratories through public enlightenment campaigns and re-training of cleaning personnel in addition to adequate supervision of the cleaning and disinfection of the Laboratory.
- Regular and proper environmental sanitation should be practice in the Laboratory in order to bring back good sanitary condition in the laboratories.
- Disinfection of Benches, chairs, Doors and windows should be done regularly in the College laboratories because bacteria are everywhere, they can easily get into the hands and items touched during daily activities and cause infection.
- Regular cleaning of hands with soap and water or hand sanitizer that contain at least 60% alcohol is one of the most important step to avoid the spread of bacteria in the laboratory.
- Prompt diagnosis and treatment of infected students and staff is highly recommended.
References
-
Agbo EC, Ejinaka OR, Obeta MU, Nwaru IE, Ibanga IE, et al. (2020) Antimicrobial Susceptibility Pattern of Biofilm forming Pseudomonas aeruginosa Isolated from Noncritical Surfaces in a Tertiary Healthcare Facility in South Eastern Nigeria. American Journal of Public Health Research 8(3): 87-92.
-
Bhalakia N, Morris D (2005) Isolation and plasmid analysis of Vancomycin resistant Staphylococcus aureus. Journal of Young Invest 13.
-
Kleven RN, Edwards JR, Tenover FC, McDonald LC, Huran T (2007) Changes in the epidemiology of methicillin- resistant Staphylococcus aurues in intensive care unit in US hospitals. Clin Infect Diseases 42: 389-391.
-
Okon KO, Shittu AO, Usman H, Adamu N, Balogun ST (2013) Epidemiology and antibiotic susceptibility pattern of methicillin-resistant Staphylococcus aureus recovered from tertiary hospitals in Northeastern, Nigeria. Journal of Medicine Med Sci 4: 214-220.
-
Enright MC, Robinson DA, Randle G, Feil EJ, Grundmann H (2002) The evolutionary history of Methicillin- Resistant Staphylococcus aureus (MRSA). Proc Natil Acad Sci 28: 7687-7692**.**
-
Okon KO, Basset P, Uba A, Lin J, Oyawoye B (2009) Co- occurrence of predominant panton valentine leukocidin- positive Sequence Type (ST) 152 and multidrug- resistant ST241 Staphylococcus aureus clones in Nigerian hospitals. Journal of Clin Microbiol 47: 3000-3003.
-
Ochei J, Kalhatkah A (2008) Introduction to Medical Laboratory Science, Theory and Practice. Tata McGraw- Hill publishing company limited, USA.
-
Couick S, Boyle-veura S, Daum RS (2006) Community AcquiredMethicillin-Resistant Staphylococcus aureus. The role of parto-voln tireleakocidin-laboratoryinvent 2: 76-79**.**
-
Blaire EO, Mulcher AC (1958) Medical Microbiology Techniques. Public worthsand cooperation limited, London 8: 341-400.
-
Uzomoh RE, Ohenhen RE, Rojughokan AK (2006) Microbiological and Nutritional Qualities of Dietary Product: Nono and Wara. National and Science 4(3): 37- 40.
-
Amare A, Amare A, Tadesse S (2023) Prevalence of pathogenic Bacteria and Antibiotic Susceptibility Profiles Isolated Medical Equipment and Inanimate Surfaces. Clin Lab 69(6).
-
Chambers EC, Monago EA (2001) Evaluation of nutritional and microbiological quality of Nunu in River State. Nigeria international Journal nutrition 8: 68-69**.**
-
Joseph OAS (2017) Staphylococus aureus Surface Colonization of Medical Equipment and Environment, Implications in Hospital-Community Epidemiology. J Hosp Manage 3: 1.
-
Chambers HF (2001) The Changing of Epidemiology of Staphylococcus aureus. Emerg infect Dis 7(2): 178-182.
-
McDonald J, Huran T, Klevens RK, Edwards (2006) Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care unit in US hospitals. Clin Infect Dis 42(3): 389-391.
-
Ochei J (2000) Enterabacteriacease in Sheri’s Medical Microbiology: An Introduction to Infectious Diseases. 3rd(Edn.), of Appleton and large, pp: 2606-2673.
-
Willey S, Wollveston T (2011) Dairy Microbiology: The Microbiology of staphylococcus 8: 341-400.
- Epidemiological and Clinical Aspects of Intestinal Parasitoses Among Students in the City of Bocaranga, Central African Republic
- Artificial Intelligence Empowers Global Infectious Disease Prevention and Control: Opportunities and Challenges
- Factors that Affect the Incidence of Babesia and Blood Donor Testing in Select States: A Regression Analysis
- Neuro-TB: The Battle between Tuberculosis and the Nervous System
- The Biological and Health Implications of Cat Fleas (Ctenocephalides felis): Assessing Zoonotic Risks and Hygiene Strategies
- Biostatistical Analysis of Medicinal Plants for Treating Schizophrenia