Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
Background: Access to mental health services for children and adolescents has emerged as a critical public health concern. Despite rising rates of depression, anxiety, and suicidality among youth, inpatient psychiatric capacity has not kept pace with demand, particularly for pediatric populations. Limited bed availability, geographic concentration, and inconsistent public reporting create significant barriers to care. Objective: The purpose of this study was to characterize pediatric inpatient psychiatric bed capacity in North Carolina using publicly available regulatory and health system data, evaluate geographic distribution of services, and assess the extent of data gaps across facility types. Study Design: Cross-sectional, descriptive analysis using publicly accessible administrative, regulatory, and health system data. Methods: A tiered data source framework was developed to guide facility identification and data abstraction. Facilities were identified through the North Carolina Division of Health Service Regulation (DHSR) Mental Health Hospital licensing roster and supplemented with Certificate of Need (CON) documents, official health system sources, and secondary public sources. Pediatric inpatient psychiatric bed counts were recorded only when explicitly reported; no estimation or extrapolation was performed. Results: Sixteen facilities and health system entities were identified. Seven freestanding psychiatric hospitals provided verifiable pediatric bed counts totaling 334 beds. Including two hospital-based units with verified capacity, total documented statewide pediatric inpatient psychiatric capacity reached approximately 372 beds, corresponding to 13.9–15.5 beds per 100,000 youth. Capacity was geographically concentrated in a small number of counties, with 92 of 100 North Carolina counties lacking any documented pediatric inpatient psychiatric resources. Conclusion: Pediatric inpatient psychiatric capacity in North Carolina is limited, geographically concentrated, and incompletely characterized due to inconsistent reporting. Improved data transparency and standardized reporting are needed to support effective health system planning and ensure equitable access.
Ashley Parks1*, Keysha Workman1 and Matthew Lazari2
Letter to Editor
Abbreviations
EDs: Emergency Departments; CON: Certificate of Need; DHSR: Division of Health Service Regulation; AHA: American Hospital Association.
Introduction
Access to mental health services for children and adolescents has emerged as a critical public health concern in the United States, with increasing prevalence of depression, anxiety, and behavioral disorders among youth populations [1]. National surveillance data indicates rising rates of persistent feelings of sadness and suicidality among adolescents, alongside increased utilization of emergency departments (EDs) for mental health crises [2, 3]. Inpatient psychiatric care represents a key component of the continuum of behavioral health services, providing stabilization and intensive treatment for acute psychiatric conditions [4]. However, access to inpatient care, especially for children and adolescents, is frequently constrained by limited bed availability, workforce shortages, and systemic barriers to care delivery [5, 6].
A growing body of literature has examined psychiatric bed capacity in the United States, demonstrating that supply has not kept pace with demand, particularly for pediatric populations [7]. National analyses have documented substantial geographic variation in psychiatric bed distribution, with higher concentrations of beds in urban areas and persistent shortages in rural regions [8]. Recent studies focusing specifically on pediatric inpatient psychiatric capacity have found that the number of beds per 100,000 children has remained relatively stable over time, despite increasing need, suggesting a widening gap between demand and available resources [7, 9]. These capacity constraints have been linked to downstream effects such as prolonged ED boarding, delayed admissions, and increased strain on healthcare systems [10].
Despite these insights, much of the existing literature relies on aggregate national datasets or administrative sources that do not provide facility-level granularity. As a result, there is limited understanding of how pediatric inpatient psychiatric capacity is distributed within individual states and across specific healthcare systems [11]. State-level analyses are particularly important because healthcare delivery systems, regulatory environments, and resource allocation mechanisms vary substantially across jurisdictions [12]. In North Carolina, behavioral health services are influenced by a combination of state regulatory oversight, regional managed care organizations (LME/ MCOs), and evolving policy frameworks governing facility development and reporting [13].
A critical challenge in assessing inpatient psychiatric capacity is the lack of standardized, publicly accessible data across different facility types. Freestanding psychiatric hospitals are typically licensed and regulated by state agencies such as the North Carolina Division of Health Service Regulation (DHSR), which maintains facility rosters and documentation of licensed bed capacity [14]. Historically, the development and expansion of inpatient psychiatric services in North Carolina were also subject to Certificate of Need (CON) regulations, requiring facilities to obtain state approval and providing detailed documentation of proposed bed counts, service lines, and population need [15]. These CON documents represent a valuable source of facility-level data for understanding inpatient psychiatric capacity.
However, recent policy changes have altered this regulatory landscape. Legislative reforms, including the removal of psychiatric inpatient services from CON oversight, have reduced the availability of standardized documentation for newly developed or expanded facilities [16]. While these changes may facilitate more rapid expansion of services, they also introduce challenges for monitoring system capacity, as fewer regulatory mechanisms require public reporting of bed counts and service characteristics.
In contrast to freestanding psychiatric hospitals, hospital-based psychiatric units embedded within general acute care hospitals are not consistently subject to the same level of public reporting. Although hospitals report overall bed counts through federal systems such as the Centers for Medicare & Medicaid Services (CMS) cost reports and the American Hospital Association (AHA) Annual Survey, these data sources often lack detailed breakdowns of pediatric psychiatric beds or unit-level capacity [17]. Furthermore, publicly accessible hospital websites frequently confirm the existence of pediatric psychiatric services without specifying the number of available beds. This inconsistency results in a fragmented data environment in which certain components of the inpatient psychiatric system are well-documented, while others remain difficult to quantify [6].
The absence of standardized reporting requirements for pediatric inpatient psychiatric capacity has important implications for health system planning and policy development. Without reliable and comprehensive data, it is challenging for policymakers, healthcare administrators, and researchers to accurately assess system capacity, identify geographic disparities, or evaluate whether existing resources meet population needs [17]. This issue is particularly salient for pediatric populations, where specialized services are often limited and concentrated in a small number of facilities [18].
Given these challenges, there is a need for state-level, facility-specific analyses that integrate multiple data sources to construct a more complete picture of pediatric inpatient psychiatric capacity. Such analyses can provide valuable insights into both the distribution of resources and the limitations of existing data systems.
Purpose of the Study
The purpose of this study was to characterize pediatric inpatient psychiatric bed capacity in North Carolina using publicly available regulatory and health system data, evaluate geographic distribution of services, and assess the extent of data gaps across facility types. By combining facility-level data with population-based measures, this study aims to provide a more detailed and transparent assessment of pediatric inpatient psychiatric capacity and to highlight opportunities for improving data reporting and system planning.
Materials and Methods
Study Design and Objective
This study used a cross-sectional, descriptive design to characterize pediatric inpatient psychiatric bed capacity in North Carolina using publicly accessible administrative, regulatory, and health system data. The primary objective was to construct a facility-level dataset of pediatric inpatient psychiatric bed availability and related facility characteristics utilizing the North Carolina Division of Health Service Regulation (DHSR) Mental Health Hospital licensing roster [19] and other publicly available Certificate of Need (CON) reports. This study endeavored to rigorously distinguish between facilities with publicly verifiable pediatric bed counts and facilities known to provide pediatric inpatient psychiatric services for which bed counts were not publicly available. The analytic focus was on documented pediatric inpatient psychiatric capacity, not real-time bed availability or staffed bed counts.
Setting
The study was conducted in North Carolina and included freestanding psychiatric hospitals, hospital-affiliated psychiatric facilities, and general acute care hospitals with publicly identified pediatric inpatient psychiatric services. The unit of analysis was the individual facility or hospital- based psychiatric unit. In cases where information was reported only at the health-system level and could not be disaggregated to a specific hospital campus, the health- system psychiatric service line was retained as the analytic unit and labeled accordingly.
Conceptual Definitions
To ensure consistent data abstraction and interpretation across facilities, the following operational definitions described below in Table 1 were used. These definitions were applied consistently across all facilities to ensure comparability of capacity estimates and transparency in data abstraction.
| for header rows and for data cells. Use for bold text within cells. Preserve empty cells. Return ONLY the HTML , no other text. | ||
|---|---|---|
| Variable | Definition | Notes / Application |
| Pediatric Inpatient Psychiatric Beds | Inpatient beds explicitly designated for children, adolescents, teens, youth, or child/adolescent psychiatric hospitalization. | Excludes outpatient services, partial hospitalization programs, intensive outpatient programs, emergency department observation, psychiatric residential treatment facilities (PRTFs), and non-psychiatric pediatric hospitalizations unless otherwise specified. Only beds explicitly identified in source materials were included. |
| Total Psychiatric Beds | Total inpatient psychiatric capacity associated with the facility or psychiatric unit, including both adult and pediatric beds when reported. | For freestanding psychiatric hospitals, reflects the full psychiatric bed complement as documented in regulatory or licensing sources. For pediatric-only hospital-based units, total beds equal pediatric beds. Total hospital bed counts were not used to avoid non-comparable estimates. |
| Operational Status | Classification of facility status at the time of data abstraction. | Categories include: Operational, Planned, Under Development, and Unverified. Status was assigned based on language in source documents (e.g., “open,” “approved,” “under construction”). |
| Verification Status | Level of confidence in the reported pediatric bed count based on source type. | Used to distinguish high-confidence data from incomplete or indirect evidence. Categories include: A (Regulatory/CON source), B (Official health system source), C (Secondary source such as press release), and Unverified (service identified but no bed count available). |
Table 1: Key Variable Definitions for Pediatric Inpatient Psychiatric Capacity Analysis.
Data Source Identification
A tiered data source framework was developed a priori to guide facility identification and data abstraction. Sources were categorized based on their level of regulatory authority, reliability, and level of detail provided regarding inpatient psychiatric capacity as shown in Table 2 below.
| Source Type | Description | Examples | Role in Analysis | |
|---|---|---|---|---|
| Tier 1 | Regulatory / Administrative Sources | Official state-level regulatory or licensing documents providing standardized and authoritative information on inpatient psychiatric facilities and bed capacity. | NC DHSR licensing rosters; Certificate of Need (CON) findings and approval documents; State Medical Facilities Plan (SMFP) | Primary source for facility identification and verified pediatric and total psychiatric bed counts |
| Tier 2 | Official Health System Sources | Publicly available information from healthcare systems or hospitals describing services, facilities, and occasionally bed capacity. | Health system websites; hospital facility profiles; service line descriptions | Used to supplement Tier 1 data and identify additional facilities and pediatric bed counts when explicitly stated |
| Tier 3 | Secondary Public Sources | Non-regulatory sources providing information about facilities or planned services, often without standardized reporting. | Press releases; news articles; public announcements | Used to identify planned or emerging facilities and confirm service availability when higher-tier sources were unavailable |
Table 2: Data Source Hierarchy and Classification.
Tier 1 sources consisted of regulatory and administrative documents, including North Carolina DHSR licensing records and CON findings and approval documents. These sources were considered the highest level of evidence due to their standardized structure and requirement for formal documentation of inpatient psychiatric bed capacity. Tier 2 sources included official health system and hospital-level publications, such as facility webpages and service line descriptions. These sources were used to identify hospital- based pediatric psychiatric units and to extract bed counts when explicitly reported. Tier 3 sources consisted of secondary public materials, including press releases and news reports, used to identify planned or recently developed pediatric psychiatric services. This tiered approach allowed for systematic identification of facilities while maintaining transparency regarding data quality and source reliability.
Facility Identification and Inclusion Criteria
To construct a comprehensive dataset of pediatric inpatient psychiatric capacity, a multi-step facility identification process was employed. This process was designed to systematically identify all relevant facilities providing inpatient psychiatric services in North Carolina and to determine their inclusion based on the presence of pediatric inpatient psychiatric care.
Facilities were included if they met at least one of the following criteria: 1. listed as a licensed psychiatric hospital in state regulatory records, or 2. publicly identified as providing inpatient psychiatric services for pediatric populations.
This approach ensured inclusion of both freestanding psychiatric hospitals and hospital-based psychiatric units, while allowing for identification of facilities with incomplete publicly reported capacity data.
State-operated psychiatric hospitals and facilities that exclusively serve adult populations were excluded from the analytic dataset. State psychiatric hospitals in North Carolina primarily provide high-acuity, forensic, and referral-based services and do not function as general-access inpatient psychiatric facilities for pediatric populations.
Identification of Freestanding Psychiatric Hospitals
The initial facility universe was established using the North Carolina DHSR roster of licensed mental health hospitals. For each facility, baseline variables were recorded: facility name, county, city, licensing identifier (when available), and apparent facility type. This step established a standardized and reproducible baseline list of freestanding psychiatric hospitals within the state.
Assessment of Pediatric Service Availability
Each freestanding psychiatric hospital was subsequently evaluated to determine whether it provided inpatient psychiatric services for pediatric populations. This assessment involved targeted searches for facility-specific regulatory documents and official descriptions using pediatric-specific and regulatory keywords including: “child,” “adolescent,” “youth,” “pediatric,” “inpatient psychiatric beds,” “certificate of need,” “findings,” and “approval.” Facilities were classified as providing pediatric inpatient psychiatric services if any source explicitly indicated the presence of child or adolescent psychiatric care.
Identification of Hospital-Based Pediatric Psychiatric Services
Since pediatric inpatient psychiatric services are not limited to freestanding psychiatric hospitals, an additional identification process was conducted to capture hospital- based psychiatric units and hospital-affiliated psychiatric facilities. This process involved a purposive review of major health systems operating in North Carolina, including academic medical centers, regional health systems, and integrated delivery networks. Searches were conducted using behavioral health service terms including: “pediatric psychiatry,” “child and adolescent psychiatry,” “behavioral health children teens,” “inpatient behavioral health,” and “achild psychiatric unit.”
Dataset Assembly and Facility Classification
All identified facilities were compiled into a single master dataset. Each facility was assigned a provisional classification based on its organizational structure and service model: freestanding psychiatric hospital, hospital-affiliated psychiatric facility, general hospital-based psychiatric unit, integrated health system psychiatric service, or planned facility. All facility records were considered provisional and subject to further validation through the data abstraction and verification procedures described below.
Data Abstraction Procedure
A structured data abstraction framework was developed a priori and applied consistently across all identified facilities. For each facility, data were extracted from the highest- priority available source according to the predefined source hierarchy (Table 2). Variables abstracted when available included: facility name, county, facility type, pediatric inpatient psychiatric bed count, total inpatient psychiatric bed count, year associated with the documented capacity, source type, operational status, source link, and notes documenting ambiguity, assumptions, or data limitations.
To ensure consistency and reproducibility, standardized abstraction rules were applied across all facilities. Only explicitly reported pediatric inpatient psychiatric bed counts were recorded as numeric values. No estimates or inferred values were entered. Facilities identified as providing pediatric inpatient psychiatric services but lacking publicly reported bed counts were retained in the dataset with missing numeric values and classified as unverified.
Construction of the Verified Dataset
Facilities were classified as verified when pediatric inpatient psychiatric bed counts could be directly confirmed through high-confidence sources. A facility was considered to have a verified pediatric bed count if at least one of the following conditions was met: (a) a regulatory or administrative document explicitly identified child or adolescent psychiatric bed counts; (b) a state approval or findings document specified the pediatric bed complement; or (c) an official hospital or health system source clearly reported the number of pediatric inpatient psychiatric beds.
Facilities meeting these criteria were assigned a verification status reflecting the strength of the supporting evidence: A (regulatory or administrative source), B (official health system or facility source), or C (secondary public source with explicit bed count). The primary analytic dataset consisted of facilities with verification status A or B.
Manual Validation of Unverified Records
A structured manual validation process was conducted for facilities initially classified as unverified. For each unverified facility, targeted searches were conducted using combinations of facility names and pediatric behavioral health keywords. Cross-source confirmation was sought when pediatric psychiatric services were identified in a single source. Facilities were reclassified as verified only when a numeric pediatric bed count was explicitly reported in an authoritative source. No estimation or extrapolation of capacity was performed.
Variable Construction
All study variables were defined and constructed using standardized criteria to ensure consistency and reproducibility as outlined in Table 3 below. Variable definitions were established prior to final data abstraction and applied uniformly across all facilities.
| for header rows | for data cells | for notes | |
|---|---|---|---|
| Facility | Name of the healthcare facility providing inpatient psychiatric services | Standardized to the most current official name identified in source documents | Alternate or legacy names recorded in notes field |
| County | County in which the facility is located | Assigned based on physical location of the facility | “Multiple” used for system-level records spanning multiple locations |
| Facility Type | Classification based on organizational structure and licensing context | Categories include: Freestanding psychiatric hospital; Hospital-affiliated psychiatric facility; General hospital unit; Integrated health system psychiatric service; Planned facility | Used to stratify analyses and identify structural differences in reporting |
| Pediatric Beds | Number of inpatient psychiatric beds designated for pediatric populations | Only explicitly reported values were recorded; no estimation or extrapolation performed | Excludes outpatient, residential, and non-psychiatric beds |
| Total Psychiatric Beds | Total inpatient psychiatric capacity associated with the facility or unit | Includes both adult and pediatric beds when reported; for pediatric-only units, equals pediatric beds | Total hospital beds were not used |
| Year | Year associated with documented capacity | Defined as the most relevant year available (e.g., approval, opening, expansion) | Used for contextual reference only, not trend analysis |
| Source Type | Highest-level source used to derive facility data | Categories: CON/regulatory; Health system; Press release/media; Unknown | Reflects data provenance |
| Status | Operational status at time of data collection | Categories: Operational; Planned; Under development; Unverified | Based on source language |
| Estimated Youth Population | County-level population under age 18 | Derived from publicly available U.S. Census estimates | Used as denominator for rate calculations |
| Beds per 100,000 Youth | Standardized measure of pediatric bed availability | Calculated as (Pediatric Beds ÷ Estimated Youth Population) × 100,000 | Calculated only when both numerator and denominator were available |
| Unit Scope | Indicates whether facility serves pediatric-only or mixed populations | Categories: Pediatric-only; Mixed adult/pediatric; Unknown | Used to interpret total bed values |
| Source Link | URL or reference supporting data entry | Direct link to regulatory document, website, or publication | Supports reproducibility |
| Notes | Free-text field capturing contextual information | Includes discrepancies, assumptions, alternate names, and “upon completion” language | Supports transparency and auditability |
Table 3: Variable Construction and Coding Rules.
Population Denominator Construction
County-level youth population estimates were assigned to each facility based on its geographic location. These values were derived from publicly available U.S. Census data and represent the population under age 18. Beds per 100,000 youth were interpreted as a localized proxy for access rather than a precise measure of service coverage, as patient catchment areas may extend beyond county boundaries.
Analysis
Data Analysis
The analytic approach was designed to provide a descriptive, facility-level assessment of pediatric inpatient psychiatric bed capacity in North Carolina, with particular emphasis on quantifying documented capacity, examining geographic distribution, and identifying gaps in publicly reported data. Because the primary objective of the study was to characterize the current capacity landscape rather than to test causal hypotheses, the analysis was limited to descriptive statistics and rate-based comparisons. The primary analytic dataset consisted of facilities with verified pediatric inpatient psychiatric bed counts, defined as facilities assigned verification status A or B.
Capacity Summaries
Descriptive analyses were performed to quantify the number of facilities identified, the number of facilities with verified pediatric bed counts, and the number of facilities with confirmed services but missing capacity data. Statewide documented pediatric inpatient psychiatric capacity was calculated as the sum of verified pediatric bed counts across all included facilities. Facility-level variation in pediatric inpatient psychiatric capacity was examined by summarizing the range and distribution of pediatric bed counts across verified facilities, with additional descriptive comparisons conducted by facility type.
Geographic Analysis
Geographic variation in pediatric inpatient psychiatric capacity was assessed using county-level facility location and youth population estimates. For each facility with a verified pediatric bed count, a standardized rate of pediatric inpatient psychiatric beds per 100,000 youth was calculated using the following formula:
Beds per 100,000 Youth = (Pediatric Beds / Estimated Youth Population) × 100,000
These rates were used as localized proxies for pediatric inpatient psychiatric access and were interpreted cautiously, given that facility service areas may extend beyond county boundaries. County-level summaries were used to identify regions with higher documented concentrations of pediatric psychiatric beds as well as counties with no publicly documented inpatient pediatric psychiatric capacity.
Stratified Descriptive Comparisons
To better characterize the structure of the pediatric inpatient psychiatric system, descriptive summaries were stratified by facility type, verification status, and operational status. A secondary descriptive comparison was conducted to distinguish documented current capacity from potential future capacity, with planned facilities retained separately from current operational facilities.
Treatment of Missing Data
Missing data was handled conservatively. Facilities for which pediatric inpatient psychiatric services could be identified but no numeric bed count was publicly available were retained in descriptive tables and narrative summaries but excluded from numeric totals, rate calculations, and other analyses requiring a verified pediatric bed count. No imputation, interpolation, or estimation of missing bed counts was performed. Missingness was interpreted as meaningful and reflective of limitations in publicly accessible reporting systems, rather than as random data absence.
Analytic Tools
Data management and descriptive analyses were conducted using Microsoft Excel and IBM SPSS Statistics 31. Tables and figures were developed to summarize facility characteristics, capacity measures, and reporting completeness, and to illustrate the geographic distribution of pediatric inpatient psychiatric facilities and facility-level variation in pediatric bed counts across the state.
Quality Assurance and Reproducibility
Several procedures were implemented to ensure consistency, transparency, and reproducibility of the data set and analytic approach. All study variables were defined a priori using a structured data dictionary (Table 1), and these definitions were applied uniformly across all facilities. A tiered source hierarchy (Table 2) was established prior to data abstraction. All facilities with incomplete, ambiguous, or conflicting data underwent structured manual review, including cross-source validation where possible. The study intentionally prioritized transparency and reproducibility over completeness. When source evidence was incomplete or ambiguous, no imputation or estimation of pediatric bed counts was performed.
Ethical Considerations
This study used only publicly available, facility-level, non-patient data and did not involve human subjects, patient identifiers, or protected health information. Institutional review board review was therefore not required.
Results
Facility Identification and Dataset Composition
A total of 16 facilities and health system entities were identified as providing or planning to provide inpatient psychiatric services in North Carolina through the multi- phase identification process. Of these, 7 freestanding psychiatric hospitals reported verifiable pediatric inpatient psychiatric bed counts through Tier 1 or Tier 2 sources and formed the core analytic dataset.
Additional pediatric inpatient psychiatric capacity was identified in hospital-affiliated and general hospital-based settings, including integrated health systems and standalone hospital units. Among these, two facilities Atrium Health Behavioral Health (system-level reporting) and the Cape Fear Valley Adolescent Unit (Cumberland County) reported explicit pediatric bed counts and were included in expanded capacity calculations. A separate Cape Fear Valley unit in Harnett County was identified as planned and retained for future capacity analysis.
Several large health systems, including Duke University Hospital, Mission Hospital, and Novant Health, were confirmed to provide pediatric inpatient psychiatric services; however, numeric bed counts were not publicly reported and therefore these facilities were excluded from quantitative capacity estimates but retained in descriptive analyses.
Pediatric Inpatient Psychiatric Bed Capacity
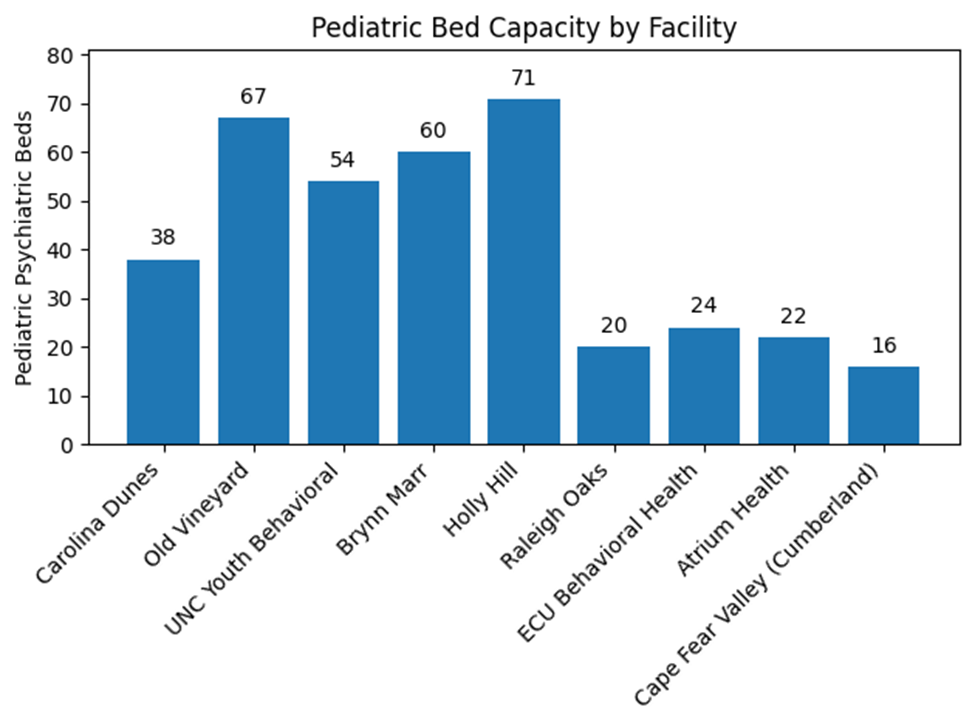
Across the 7 freestanding psychiatric hospitals, a total of 334 pediatric inpatient psychiatric beds were documented. When including hospital-based units with verified pediatric capacity specifically Atrium Health (22 beds) and Cape Fear Valley Cumberland (16 beds) the total documented pediatric inpatient psychiatric capacity increased to approximately 372 beds statewide. Pediatric bed counts varied across facilities, ranging from 16 to 71 beds, with the highest concentrations observed in larger freestanding psychiatric hospitals.
When standardized to population, these values correspond to approximately 13.9 pediatric inpatient psychiatric beds per 100,000 youth based on freestanding facilities alone, and approximately 15.5 beds per 100,000 youth when including hospital-based units with verified capacity, providing a range of conservative to expanded estimates of statewide capacity.
Total Psychiatric Capacity Context
Total inpatient psychiatric bed capacity (adult and pediatric combined) varied widely across facilities, ranging from 54 to 268 beds among freestanding hospitals. Pediatric beds represented a minority proportion of total psychiatric capacity within mixed-use facilities, indicating that pediatric services constitute a limited subset of broader inpatient psychiatric resources. This imbalance was particularly evident in larger facilities, where adult inpatient services dominated overall capacity, reinforcing the structural prioritization of adult psychiatric care within the system (Figure 1).
Geographic Distribution of Capacity
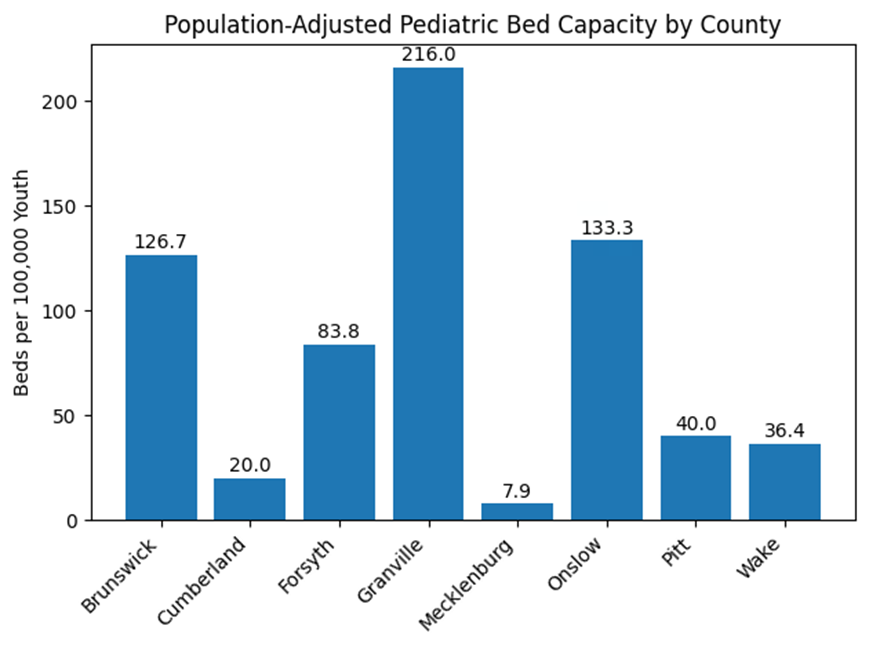
Pediatric inpatient psychiatric capacity was unevenly distributed across North Carolina, with a strong concentration in counties hosting freestanding psychiatric hospitals. Counties such as Brunswick, Onslow, and Granville demonstrated the highest levels of pediatric bed availability, with rates exceeding 120 beds per 100,000 youth in some cases. Granville County, home to a pediatric-dedicated facility, demonstrated the highest observed rate at approximately 216 beds per 100,000 youth.
In contrast, more populous counties without freestanding facilities exhibited significantly lower capacity. Mecklenburg County, despite being one of the largest population centers in the state, demonstrated only 7.9 beds per 100,000 youth based on system-level reporting from Atrium Health. Cumberland County, with a newly established adolescent unit, demonstrated a moderate rate of approximately 20.0 beds per 100,000 youth. Many counties across the state had no publicly documented pediatric inpatient psychiatric capacity, highlighting substantial geographic disparities in access. All other North Carolina counties (92 out of 100) lacked dedicated inpatient pediatric psychiatric resources, representing a large proportion of unserved adolescents and children (Figure 2).
Hospital-Based Capacity and Data Gaps
Hospital-based pediatric psychiatric services contributed additional capacity; however, these facilities were inconsistently represented in publicly available data sources. While some systems reported pediatric bed counts explicitly, others confirmed the existence of services without providing quantitative capacity data. Facilities with confirmed pediatric services but no reported bed counts represented a substantial portion of the overall system. These facilities were excluded from numeric totals but included in descriptive analyses, underscoring a critical limitation in the ability to fully characterize statewide capacity.
Data Completeness and Reporting Gaps
A significant proportion of identified facilities lacked publicly reported pediatric inpatient psychiatric bed counts. This lack of reporting was most pronounced among hospital- based psychiatric units, in contrast to freestanding psychiatric hospitals, which were more consistently documented through regulatory processes. These findings indicate that statewide pediatric inpatient psychiatric capacity cannot be fully quantified using publicly available data, and that existing estimates likely represent a conservative minimum rather than a complete measure of system capacity.
Discussion
Principal Findings
This study provides a comprehensive, facility-level assessment of pediatric inpatient psychiatric capacity in North Carolina and highlights three major findings: (1) limited overall capacity, (2) substantial geographic disparities in access, and (3) significant gaps in publicly available data, particularly for hospital-based services. The total documented pediatric inpatient psychiatric capacity of approximately 372 beds statewide suggests that inpatient resources for children and adolescents are limited relative to population need. Moreover, the concentration of these beds within a small number of facilities indicates that access to care is highly dependent on geographic location.
Comparison to National Benchmarks
When contextualized using population-based benchmarks, pediatric inpatient psychiatric capacity in North Carolina appears constrained. Using approximate population estimates, the state’s capacity equates to roughly 13.9–15.5 beds per 100,000 youth, depending on inclusion criteria. A large cross-sectional study of pediatric inpatient psychiatric capacity in the United States estimated that national capacity is approximately 14–16 beds per 100,000 children, with substantial variation across states and regions [20]. Importantly, that study also found that pediatric psychiatric bed capacity has remained relatively stable over time despite increasing demand, suggesting a widening gap between need and available resources.
Compared to this national estimate, North Carolina’s pediatric inpatient psychiatric capacity falls at the lower end of the national range, even when including hospital-based units with verifiable bed counts. This finding is particularly notable given the uneven geographic distribution of beds within the state. In contrast, broader psychiatric bed benchmarks across all age groups have historically suggested targets of approximately 40–60 beds per 100,000 population, reflecting the level of capacity needed to meet system-wide demand. These benchmarks highlight the relatively small proportion of inpatient psychiatric resources allocated to pediatric populations.
Geographic Access and System Structure
The uneven distribution of pediatric psychiatric beds across the state has important implications for access. Counties with dedicated psychiatric hospitals demonstrate relatively high capacity, while many regions lack any documented inpatient pediatric services. This geographic imbalance likely contributes to known challenges in accessing care, including increased travel distances for families [21], delays in admission, reliance on emergency departments for stabilization [22], and prolonged ED boarding [10, 23]. Hospital-based psychiatric units may partially mitigate these gaps; however, the lack of consistent reporting limits the ability to evaluate their true impact on access [23].
Data Transparency as a Structural Barrier
A central finding of this study is that pediatric inpatient psychiatric capacity is not fully measurable using publicly available data. While regulatory processes such as CON historically provided detailed documentation for freestanding facilities, hospital-based psychiatric units are not subject to equivalent reporting requirements. This inconsistency creates a fragmented data environment in which some facilities are highly visible and well-documented while others are functionally invisible in capacity analyses. As a result, policymakers and researchers lack the information necessary to accurately assess system capacity, identify underserved regions, and evaluate the impact of new facility development.
Policy Implications
The findings of this study have several important policy implications. The limited and uneven distribution of pediatric inpatient psychiatric beds suggests a need for targeted capacity expansion, particularly in underserved regions. However, effective planning requires accurate and complete data, which are currently lacking.
Recent policy changes in North Carolina, including the removal of psychiatric inpatient services from Certificate of Need oversight, may further reduce the availability of standardized data. While these changes may facilitate expansion of services [23], they also reduce regulatory mechanisms that historically generated publicly accessible capacity information. The absence of standardized reporting requirements for hospital-based psychiatric units represents a significant barrier to system-level planning. Policymakers
may consider implementing minimum reporting standards for inpatient psychiatric capacity, particularly for pediatric services, to support transparency and accountability. The observed imbalance between adult and pediatric psychiatric capacity suggests a need to prioritize pediatric-specific services within broader behavioral health planning efforts.
Limitations
This study has several limitations. The analysis relies on publicly available data, which may not capture all operational capacity. Licensed bed counts may overestimate actual availability due to staffing constraints and temporary closures. The county-level population estimates may not reflect actual service catchment areas, as those frequently change based on resources available and can be impacted by geography and preference. Finally, the exclusion of facilities without reported bed counts from quantitative analyses may result in underestimation of total capacity. This study was conducted within the limitations of existing publicly reported data structures.
Conclusion
Pediatric inpatient psychiatric capacity in North Carolina is limited, geographically concentrated, and incompletely characterized due to inconsistent reporting across facility types. The majority of measurable capacity is located within a small number of freestanding psychiatric hospitals, while hospital-based services are not consistently represented in publicly available data. These findings highlight the need for improved data transparency and standardized reporting of pediatric inpatient psychiatric capacity to support effective health system planning and ensure equitable access to care. Without comprehensive and reliable data, it remains difficult to fully assess system capacity or determine whether the needs of pediatric populations are being met.
Conflicts of Interest
The authors declare no conflict of interest. No funding was provided for this faculty-led student-engaged research project.
Acknowledgment
This work reflects a collaborative faculty-student research initiative focused on healthcare access and system capacity. The authors acknowledge student researcher Keysha Workman’s passion for pediatric mental health access. This paper is the first step in supporting the student researcher’s goals of expanding pediatric inpatient psychiatric service access in North Carolina.
References
-
Benton TD, Boyd RC, Njoroge WFM (2021) Addressing the Global Crisis of Child and Adolescent Mental Health. JAMA Pediatr 175(11): 1108-1110.
-
CDC (2026) YRBS Data Summary & Trends Report. Youth Risk Behavior Surveillance System (YRBSS).
-
Verlenden JV, Pampati S, Rasberry CN, Liddon N, Hertz M, et al. (2024) Mental Health and Suicide Risk Among High School Students and Protective Factors — Youth Risk Behavior Survey, United States, 2023. MMWR Suppl 73.
-
Horsfall J, Cleary M, Hunt GE (2010) Acute Inpatient Units in a Comprehensive (Integrated) Mental Health System: A Review of the Literature. Issues Ment Health Nurs 31(4): 273-278.
-
Lindenfeld Z, Cantor JH, McCullough CM, Bather JR, McBain RK (2025) Inpatient psychiatric bed capacity within CMS-certified U.S. hospitals, 2011–2023: A cross- sectional study. PLoS Med 22(7): e1004682.
-
Hazen EP, Prager LM (2017) A Quiet Crisis: Pediatric Patients Waiting for Inpatient Psychiatric Care. J Am Acad Child Adolesc Psychiatry 56(8): 631-633.
-
Cushing AM, Michelson KA, Bucholz EM (2024) Pediatric Inpatient Psychiatric Capacity in the US, 2017 to 2020. JAMA Pediatr 178(10): 1080-1082.
-
Liu MX, McGinty EE, Schpero WL (2025) Regional changes in inpatient psychiatric bed capacity and availability of alternative psychiatric services, 2012–2022. Health Aff Sch 3(11): qxaf204.
-
Michelson KA, Cushing AM, Bucholz EM (2025) National Trends in Pediatric Inpatient Capacity. JAMA Pediatr 179(2): 208-209.
-
Hoffmann JA (2025) Pediatric Mental Health Boarding in US Emergency Departments, 2018–2022. J Am Coll Emerg Physicians Open 6(4): 100180.
-
(2022) mergency Department-Based Psychiatric Services for Children and Adolescents: An In-Depth Investigation of Care in North Carolina. ProQuest Dissertations.
-
McConnell J (2026) Addressing Psychiatric Bed Capacity: Evidence from Medicaid’s Institutions for Mental Disease Waivers for Serious Mental Illness. Health Serv Res.
-
From Idea to Paradigm: The Integrated Primary and Mental Health Care Model in North Carolina.
-
(2026) NC DHSR MHLCS: Licensed Facilities.
-
(2026) NC DHSR HPCON: Overview of Certificate of Need.
-
(2026) Executive Order No. 33: Protecting North Carolinians Through Stronger Behavioral Health and Criminal Justice Systems. NC Governor.
-
Mahmood A, Kedia S, Arshad H, Mou X, Dillon PJ (2024) Disparities in Access to Mental Health Services Among Children Diagnosed with Anxiety and Depression in the United States. Community Ment Health J 60(8): 1532- 1546.
-
North Carolina Department of Health and Human Services, Division of Health Service Regulation (2026) Certificate of Need (CON) Decisions and Findings.
-
Alabi A, Onafowokan OT, Amusa T, Akinpeloye O, Okunola D (2026) Capacity, Financing, and Structural Strain in Mental Health Care in the United States: A Narrative Review. Cureus.
-
(2026) APA Psychiatric Bed Crisis Report. American Psychiatric Association.
-
Savioli G, Ceresa IF, Novelli V, Ricevuti G, Bressan MA, et al. (2022) Emergency Department Overcrowding: Understanding the Factors to Find Corresponding Solutions. J Pers Med 12(2): 279.
-
Mundt AP, Langerfeldt SD, Rozas Serri E, Siebenförcher M, Priebe S (2021) Expert Arguments for Trends of Psychiatric Bed Numbers: A Systematic Review of Qualitative Data. Front Psychiatry 12.
-
(2026) NCDHHS Report Shows Progress in Improving Mental Health Services in North Carolina.
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda
- Health as Consumable Item: The Indian Scenario