Bilateral Synchronous Paget's Breast Disease: A Case Report with Review
Paget's breast disease (PBD) is a rare disease with an unusual presentation, so early diagnosis is quite difficult. It is an eczematous eruption on the nipple and areola with or without underlying breast cancer. It is often misconstrued as chronic dermatitis or psoriasis and results in a delayed diagnosis. Bilateral synchronous Paget's breast disease is exceptionally rare, and only a few cases have been reported in the literature. Radiology is a supportive tool for diagnosis as it is the only histopathology that can give a definitive diagnosis. The treatment depends upon the histological findings as well as associated underlying carcinoma in the breast. Simple lumpectomy, mastectomy, or radical mastectomy depends on the lump (cancer) underneath the diseased breast. Now, we present a case of bilateral synchronous PBD without a lump in both breasts.
Introduction
Sir Paget first described Paget’s disease of the nipple in 1874. It is a malignant disease that presents itself as eroding and bleeding ulcer of the nipple and areola. Paget’s breast disease (PBD) is a diagnostic dilemma. If the skin lesions do not heal with topical therapy, a biopsy has to be performed to exclude PBD. Almost all cases are single-sided. Microscopically, typical large clear cells (Paget’s cells) with pale and abundant cytoplasm and hyperchromatic nuclei with prominent nucleoli are seen in the epidermal layer. Paget’s disease is mostly accompanied by primary invasive or in situ carcinoma of the breast. PDB presents most commonly in postmenopausal women between 50 and 60 years old, with a median age of 56–57 years [1]. PDB involving the nipple has been commonly associated with IDC and is thought to be because of epidermal extension of underlying ductal breast carcinoma [2, 3]. Ultrasounds, mammography, and magnetic resonance imaging can search for underlying cancer and guide surgical management [3, 4, 5, 6]. A biopsy is mandatory to confirm the diagnosis, particularly in cases without an associated lump. The surgical treatment of Paget’s disease is not clear, whether radical or conservative. Palpable mass and the invasiveness of cancer predict and decide about prognosis [7]. Our case is a classic case of bilateral synchronous PDB without any lumps underneath.
The 55-year-old females with no family history of cancer presented with eczema and eroded right nipple for the last two years. The disease started as dermatitis around the nipple. She consulted an Ayurveda Veda doctor and who gave her black color ointment to apply on the nipples, which caused complete necrosis of both nipples. Dermatitis and itching persisted. The examination revealed an eczematous aspect of both breasts with an eroded and absence of nipples suggesting Paget’s disease (Figure 1). There was no lymphadenopathy. Clinical examination of breasts did not reveal any palpable masses. An ultrasound and mammograms of breasts did not show any lump. Biopsy concluded PDB (Figure 2). Tissue tested positive for Estrogen and Progesterone receptors but negative for HER2 receptors (Figure 3). Mastectomy was performed without complications. Final histology concluded DCIS associated
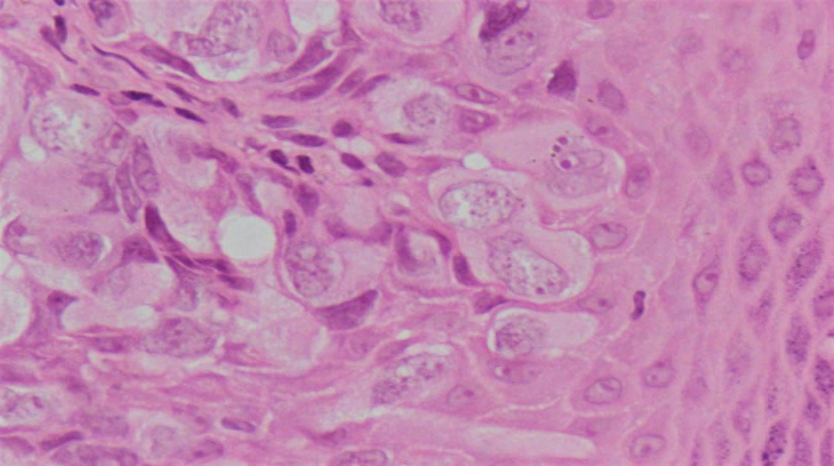
with Paget’s disease. The Sentinel lymph node was negative. There was no distance spread in the body. The patient was put on systemic chemotherapy. The patient is symptom-free after six months follow up.

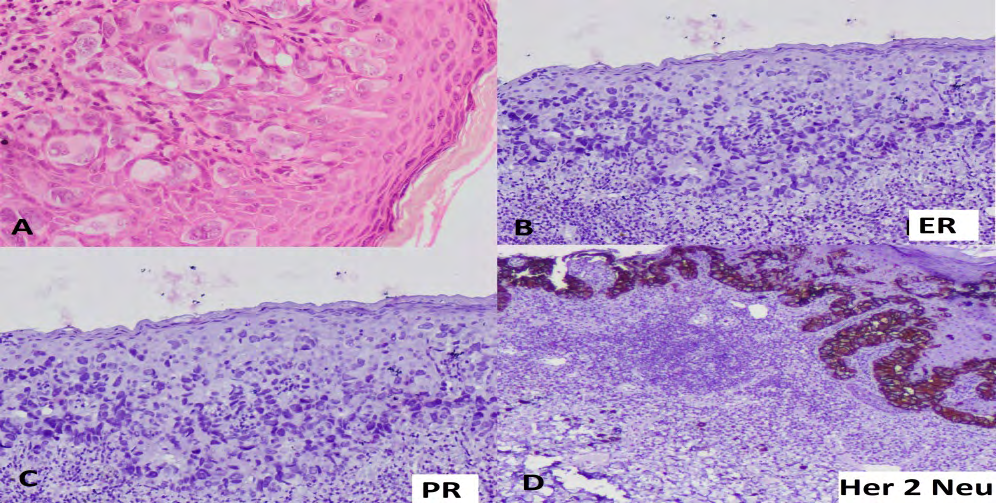
Figure 3A: tumors cells infilterating skin, 3B: Immunostaining -tumors cells -Ve for estrogen receptors, 3C: Tumors celss -Ve for progesterone receptors, 3D: Positive for Her 2 Neu.
Discussion
PBD is expressed as a “syndrome in which ulceration of the nipple is invariably associated with underlying cancer.” Paget’s disease of the nipple develops slowly without any early symptom. Mostly it starts as an eczematous erythema oozing patch of one side nipple first and then slowly start involving and spread centrifugally to invade the areola and the adjacent skin. The colour of the skin changes from pink to red. Retraction, ulceration, or bleeding or complete erosion of the nipple occurs as disease progression as in our case. Lumps or masses in the same breast occur in more than 50% of the patients. The symptoms are bizarre and may wax and wane along with redness, oozing, crusting, a nonhealing nipple sore with complete erosion and destruction of nipples. PBD is a disease of single breast. Incidence is between 1 and 4% of all breast cancers. Synchronous bilateral PBD (as in our case) is quiet rare and incidence is about 1% of all breasts cancer [8]. Other name is mammary Paget disease (MPD) [9]. A similar disease process can occur in female and male external genitalia (extramammary Paget’s disease) with similar histilogical features but with different pattthogenesis. So far, there are about thirteen reported casesss of synchronous bilateral PBD. PBD is common between 45 to 74 years [10, 11]. PBD has been described twice in men [12, 13]. The disease occurs in three forms: (1) associated with an underlying ductal carcinoma in situ (DCIS), (2) associated with invasive carcinoma, or (3) without any underlying malignancy [14]. Most patients with PD have an underlying DCIS or even invasive carcinoma [15, 16]. Benign inflammatory breast skin lesions which mimic with PBD are summarized in Table 1 [17].
| Clinical Manifestation of PBD | Clinical Manifestation of Inflammatory skin lesions in nipple | |
|---|---|---|
| Eczema | Not itchy or little itchy and is non-responsive to treatment | Itchy |
| Irritant contact Dermatitis | Nipple retraction or deformation | No changes in the nipple limited to the areola region |
| Psoriasis | No vesicles or pustules | Vesicles and pustules |
| Drug Eruption | Sometimes with or without a palpable lump | Always no lump |
Table 1: Benign skin and mammary lesions which mimic with PBD [17].
Delayed diagnosis is associated with many factors like lack of knowledge and awareness, use of traditional therapy, financial constraints, and embarrassment of a breast cancer diagnosis [18]. Classification [19] Mammary Paget disease can be divided into 3 categories: (1)Paget disease of the Nipple without DCI (2) Paget disease of the nipple with associated DCIS in the underlying lactiferous ducts of the nipple-areolar complex (3) Paget disease of the nipple with associated DCIS in the underlying lactiferous ducts of the nipple-areolar complex and associated DCIS or invasive breast cancer elsewhere in the breast, at least 2 cm from the nipple-areolar complex.
For bilateral PBD, the limited data are unclear. Sahoo, et al., correlated the PBD of its patient to an underlying lobular CIS because of the immunohistochemical report; Xie et al., did not found any underlying tumour [11, 20]. Anderson and Franceschini et al., patients suffered from underlying ductal carcinomas [21, 22]. It is still unclear whether the disease is the cause or an effect of an underlying breast carcinoma. The epidermotropism of cancerous ductal gland cells into the epidermis is most accepted theory. Other theory is the migration of malignant keratinocytes from the epidermis into deeper breast tissues as in up to 50% of the cases, there is no underlying tumour [23]. There is reduced risk of ductal, lobular, tubular, and mucinous breast cancers and high risk of medullary breast cancers in multiparous patients [24]. If similar findings are obvious for PBD, then one justification is that after lactation, there could be the inflammatory progression and restructuring of the ductal network [25]. The reason for the bilateral form of PD is unclear and this disease maybe a coincidence as the reported patients are having different age gender & ethnicity shown in Table 2 [26].
| Age In Yrs | Gender M/F | Associated cancer Right/ left breast | Country | Author | Reference | |
|---|---|---|---|---|---|---|
| 53 | F | L-Intraductal carcinoma | USA | Anderson 1979 [21] | 21 | |
| F | ? | Netherlands | Knol & Voorhuis 1981 [27] | 28 | ||
| F | ? | India | Sinha & Parshad 1983 [28] | 29 | ||
| M | ? | India | Nagar 1983 [12] | 12 | ||
| 74 | F | ? | Portugal | Fernandes et al. 1990 [10] | 10 | |
| F | ? | Greece | Markopoulos et al. 1997 [29] | 30 | ||
| 53 | F | Rt-LCIS of the Nipple, DCIS+ Microinvasive Ductal carcinoma Left-LCIS of Nipple, DCIS | USA | Sahoo et al. 2002 [11] | 11 | |
| 73 | F | Rt-High grade intraductal Carcinoma Lt-Micro papillary invasive carcinoma | Italy | Franceschini et al. 2005 [22] | 22 | |
| 74 | M | Rt-infiltrative ductal carcinoma | Turkey | Ucar et al. 2008 [13] | 13 | |
| 45 | F | China | Xie et al. 2012 [20] | 20 | ||
| 72 | F | Rt-Low grade DCIS Lt-intermediate DCIS, Invasive ductal carcinoma | Germany | Barth 2014 [30] | 27 | |
| 27 | F | Nipple Discharge B/L Lump in the left breast | India | Babu et al. 2018 [19] | 19 | |
| 54 | F | Rt & Lt Ductal Carcinoma | Java | Lina Coridah 2020 [17] | 17 | |
| 55 | F | B/L completely Eroded Nipples without any Mass | India | Sunder Goyal et al. 2021 |
Table 2: Summary of bilateral Paget’s disease [30].
(DCIS means ductal carcinoma in situ and LCIS means lobular carcinoma in situ) Table 2: Summary of bilateral Paget’s disease [30].
Diagnosis
A nipple biopsy is essential for the diagnosis of PBD. There are several types of nipple biopsy as below: Nipple discharge samples may show the presence of the Paget cells.
- Surface biopsy: A glass slide is gently used to scrape cells from the surface of the eczematous skin.
- Shave biopsy: The top layer of eczematous skin is taken with a razor-like sharp tool.
- Punch biopsy: A punch is used to remove a disk-shaped piece of the nipple and eczematous skin.
- Wedge biopsy: A blade is used to remove a small wedge of the nipple and eczematous skin. This is most informative as a good amount of tissue is available.
Most people who have PBD also have one or more tumours inside the same breast. In addition to a nipple biopsy, a clinical breast exam breast is carried out to check for lumps or other breast changes. About 50 per cent of patients with PBDs have an associated breast lump that can be felt in a clinical breast exam. An ultrasound exam, or mammogram, or magnetic resonance imaging scan is mandatory in cases with a palpable lump in the breast [15].
The mammogram is normal in PBD without papable lump as in our case [3, 6, 31]. The immunohistochemistry is essential to distinguish Paget cells from other cell types like Toker cells normally present, which are quiet similar to Paget’s disease. CD138 and p53 are positive in Paget’s disease and negative in normally present Toker cells [15]. Also, Paget cells stain positive for CK7 in >90% of the cases. Likewise, GATA3 and HER-2 are expressed in around 90% of the cases and are used for confirmation, including CK7 negative Paget disease [32].
Our case study highlights the importance of histologic examination via incisional or deep punch biopsy to confirm PDB diagnosis, regardless of a prior normal mammogram or breast ultrasound. Most patients with PBD without a palpable mass will have a normal mammogram as in our case [3, 6, 31]. The mammography is useful and sensitive to detect underlying carcinoma associated with PDB [2, 31]. Magnetic resonance imaging (MRI) is highly sensitive for detecting breast cancer, especially in patients with a normal mammogram [2]. However, negative or normal radiological studies alone cannot rule out PDB in patients presenting with cutaneous breast changes. They should be correlated with biopsy and clinical findings to establish a PDB diagnosis. A punch or wedge biopsy of the nipple should be performed to get a full-thickness biopsy of the nipple and areola to confirm the diagnosis. It is important to consider that a shave biopsy of the nipple will often not include the entire epidermis and may yield an inadequate sample. If the first biopsy does not contain adequate tissue, a repeat wedge biopsy or excision of the nipple may be necessary for patients without mass to confirm the diagnosis [2].
Treatment
Till recently, mastectomy with or without the removal of axillary lymph nodes on the same side was looked upon as the standard surgery for PBD. Most patients were associated with tumours inside the same breast [32, 33, 34]. Even if only one tumour was present, that tumour could be located several centimetres away from the nipple and areola. It would not be removed by surgery on the nipple and areola alone [33, 34]. However, in patients with PBD without a lump with negative mammograms, the breast-conservative followed by whole breast radiation therapy may be the treatment of choice. Breast conservative surgery (lumpectomy with a sentinel lymph node biopsy) is a harmless substitute for mastectomy. Its necessity is clear surgical margins and postoperative adjuvant radiotherapy. When BCS is considered, it is mandatory to exclude underlying breast cancer preoperatively by clinical, radiological and histopathological examination [8, 33, 34]. There are reports of positive lymph nodes even without any underlying malignancies [15, 16].
In patients with PBD with a breast tumour- a mastectomy with sentinel lymph node biopsy should be done to find spread in axillary lymph nodes. Axillary clearance is done if the sentinel node is positive [35, 36]. Adjuvant therapy, consisting of chemotherapy and/or hormonal therapy, may also be advocated depending upon the stage, positive lymph nodes, and estrogen and progesterone receptors in tissue and HER2 protein expression in the tumour cells. In inoperable patients, radiotherapy, laser therapy, photodynamic therapy, or chemotherapy, for example, with trastuzumab or imiquimod, can offer a therapeutic alternative [30].
Prognosis
The prognosis of PBD depends upon the following factors:
- Whether or not a tumour is present in the affected breast
- If one or more tumours are present in the affected breast, whether those tumours are DIC in situ or invasive breast cancer
- The stage of that cancer is the case of invasive breast carcinoma.
Conclusion
Diagnosis of PBD in the early stage is a diagnostic dilemma. It is uncommon breast cancer which is mostly accompanied by breast cancer. In PBD cases with normal ultrasound and mammogram, a wedge biopsy of the nipple is essential to establish the diagnosis. The presence or absence of an underneath lump decide treatment. Patients with Paget’s disease are candidates for breast conservation with appropriate preoperative investigations. Surgical consequences are equal to those of mastectomy if free surgical margins are achieved and postoperative adjuvant radiotherapy.
References
-
Dubar S, Boukrid M, Bouquetde Joliniere J, Guillou L, Vo QD, et al. (2017) Paget’s Breast Disease: A Case Report and Review of the Literature. Front Surg 4: 51.
-
Karakas C (2011) Paget’s disease of the breast. Journal of Carcinogenesis 10: 31.
-
Wong G, Drost L, Yee C, Lam E, McKenzie E, et al. (2019) Are we properly diagnosing and treating Paget’s disease of the breast? A case series. Journal of Pain Management 12(2): 169-172.
-
Challa VR, Deshmane V (2015) Challenges in diagnosing and managing Paget’s disease of the breast—A retrospective study. Indian Journal of Surgery 77(3): 1083-1087.
-
Ackerman L, Rosai J, Goldblum J, Lamps L, McKenney J, et al. (2018) Rosai and Ackerman’s surgical pathology. 11th (Edn.), Philadelphia, PA: Elsevier.
-
Bolognia J, Schaffer JV, Cerroni L (2018) Dermatology. 4th (Edn.), Elsevier.
-
Sylvana AB, Mary MG (2020) Paget’s Disease of the Breast Presenting as Nipple Ulceration With Normal Mammogram. Journal of the Dermatology Nurses’ Association 12(3): 121-123
-
Marshall JK, Griffith KA, Haffty BG, Solin LJ, Vicini FA, et al. (2003) Conservative management of Paget disease of the breast with radiotherapy: 10- and 15-year results. Cancer 97(9): 2142-2149.
-
Shi YX, Xia Q, Peng RJ, Yuan ZY, Wang SS, et al. (2012) Comparison of clinicopathological characteristics and prognoses between bilateral and unilateral breast cancer. Journal of Cancer Research and Clinical Oncology 138(4): 705-714.
-
Fernandes FJ, Costa MM, Bernardo M (1990) Rarities in breast pathology. Bilateral Paget’s disease of the breast—a case report. European Journal of Surgical Oncology 16(2): 172-174.
-
Sahoo S, Green I, Rosen PP (2002) Bilateral Paget disease of the nipple associated with lobular carcinoma in situ: application of immunohistochemistry to a rare finding. Archives of Pathology & Laboratory Medicine 126(1): 90-92.
-
Nagar RC (1983) Bilateral Paget’s disease of the nipple in a male. Journal of the Indian Medical Association 81(3- 4): 55-56.
-
Ucar AE, Korukluoglu B, Ergul E, Aydin R, Kusdemir A (2008) Bilateral Paget disease of the male nipple: first report. Breast 17(3): 317-318.
-
Chen CY, Sun LM, Anderson BO (2006) Paget disease of the breast: changing patterns of incidence, clinical presentation, and treatment in the U.S. Cancer 107(7): 1448-1458.
-
Caliskan M, Gatti G, Sosnovskikh I, Rotmensz N, Botteri E, et al. (2008) Paget’s disease of the breast: the experience of the European Institute of Oncology and review of the literature. Breast Cancer Research and Treatment 112(3): 513-521.
-
Siponen E, Hukkinen K, Heikkil P, Joensuu H, Leidenius M (2010) Surgical treatment in Paget’s disease of the breast. The American Journal of Surgery 200(2): 241- 246.
-
Choridah L, Kartika Sari W, Dwianingsih E, Widodo I, Anwar SSL (2020) Advanced lesions of synchronous bilateral mammary Paget’s disease: a case report. Journal of Medical Case Reports 14: 119.
-
Maghous A, Rais F, Ahid S, Benhmidou N, Bellahamou K, et al. (2016) Factors influencing diagnosis delay of advanced breast cancer in Moroccan women. BMC Cancer 16: 356.
-
Babu B, Dev B, Mohanapriya T, Sai Shalini CN (2018) Bilateral mammary Paget disease in a young adult female. Radiology Case Reports 13(3): 586-591.
-
Xie B, Zheng H, Lan H, Cui B, Jin K, et al. (2012) Synchronous bilateral Paget’s disease of the breast: a case report. Oncology Letters 4(1): 83-85.
-
Anderson WR (1979) Bilateral Paget’s disease of the nipple: case report. American Journal of Obstetrics &Gynecology 134(8): 877-878.
-
Franceschini G, Masetti R, D’Ugo D, Palumbo F, D’Alba P, et al. (2005) Synchronous bilateral Paget’s disease of the nipple associated with bilateral breast carcinoma. The Breast Journal 11(5): 355-356.
-
Sakorafas GH, Blanchard K, Sarr MG, Farley DR (2001) Paget’s disease of the breast. Cancer Treatment Reviews 27(1): 9-18.
-
Reeves GK, Pirie K, Green J, Bull D, Beral V (2009) Reproductive factors and specific histological types of breast cancer: prospective study and meta-analysis. British Journal of Cancer 100(3): 538-544.
-
Albrektsen G, Heuch I, Thoresen SØ (2010) Histological type and grade of breast cancer tumours by parity, age at birth, and time since birth: a register-based study in Norway. BMC Cancer 10: 226.
-
Schedin P, O’Brien J, Rudolph M, Stein T, Borges V (2007) Microenvironment of the involuting mammary gland mediates mammary cancer progression. Journal of Mammary Gland Biology and Neoplasia 12(1): 71-82.
-
Knol WLR, Voorhuis FJ (1981) Paget’s disease of the breast: a case of bilateral occurrence. Nederlands Tijdschriftvoor Geneeskunde 125(11): 416418.
-
Sinha MR, Prasad SB (1983) Bilateral Paget’s disease of the nipple. Journal of the Indian Medical Association 80(2): 27-28.
-
Markopoulos C, Gogas H, Sampalis F, Kyriakou B (1997) Bilateral Paget’s disease of the breast. European Journal of Gynaecological Oncology 18(6): 495-496.
-
Barth D (2014) Bilateral Paget’s Disease of the Breast— Case Report of Long-Time Misdiagnosed Tumors with Underlying Ductal Carcinomas and Review of the Literature. Case Reports in Dermatological Medicine 2014: 152836.
-
Helme S, Harvey K, Agrawal A (2015) Breast-conserving surgery in patients with Paget’s disease. British Journal of Surgery 102(10): 1167-1174.
-
Arain SA, Arafah M, Said Raddaoui EM, Tulba A, Alkhawaja FH, et al. (2020) Immunohistochemistry of mammary Paget’s disease. Cytokeratin 7, GATA3, and HER2 are sensitive markers. Saudi Medical Journal 41(3): 232-237.
-
Kanitakis J (2007) Mammary and extramammary Paget’s disease. Journal of the European Academy of Dermatology and Venereology 21(5): 581-590.
-
Kawase K, Dimaio DJ, Tucker SL, Buchholz TA, Ross MI, et al. (2005) Paget’s disease of the breast: there is a role for breast-conserving therapy. Annals of Surgical Oncology 12(5): 391-397.
-
Sukumvanich P, Bentrem DJ, Cody HS, Brogi E, Fey JV, et al. (2007) The role of sentinel lymph node biopsy in Paget’s disease of the breast. Annals of Surgical Oncology 14(3): 1020-1023.
-
Laronga C, Hasson D, Hoover S, Cox J, Cantor A, et al. (2006) Paget’s disease in the era of sentinel lymph node biopsy. American Journal of Surgery 192(4): 481-483.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey