Efficacy of Rituximab Therapy for Oculomotor Nerve Palsy and Vision Loss Due to Granulomatous Polyangiitis
Completely reversible oculomotor palsy VI and the vision restoration after only rituximab-corticosteroid therapy in granulomatosis polyangiitis with intraorbital mass presented with CT documentation. Short review of literature about treatment options follows.
Introduction
Sixth nerve palsy is a disorder that affects eye movement. That is due to damage of the sixth cranial nerve (n. abducens). The primary function of the sixth cranial nerve is to send signals to lateral rectus muscle. This small muscle is located on the outer side in our eye. It is responsible for turning your eye away from our nose. When the lateral rectus muscle weakness, your eye crosses inward toward your nose. If inferior oblique ocular muscle (n. III) localized closely to lateral rectus is affected, the eye deviated down inward.
A 67-year-old man with overweight, diabetes mellitus type II, arterial hypertension, congestive heart failure and paroxismal atrial fibrillation developed left ocular nerve pulsy with inward deviation of ocular nucleus and vision loss. Last three years he has treated with corticosteroid pulses and rituximab (RTX) (Anti-CD20) due to granulomatous polyangiitis (GPA) and untill December 2020 was in remission. Because corona pandemic last course postponed and half year after missed RTX for the first time he developed left retro orbital mass with internal inferior rotation of his eye with vision loss (Figure 1). IV Methylprednisolone 1g/ day pulse therapy N3 with further IV 100mg/day was reinstituted and he got infusions of RTX 500mg/week N4.
Oral prednisone continued with tapering to 20mg/day. Three moths later full resolution of ocular palsy followed (Figure 2) and his vision restored. One can see parallel restoration of anterior posterior axis (white lines) of right and left eyes.
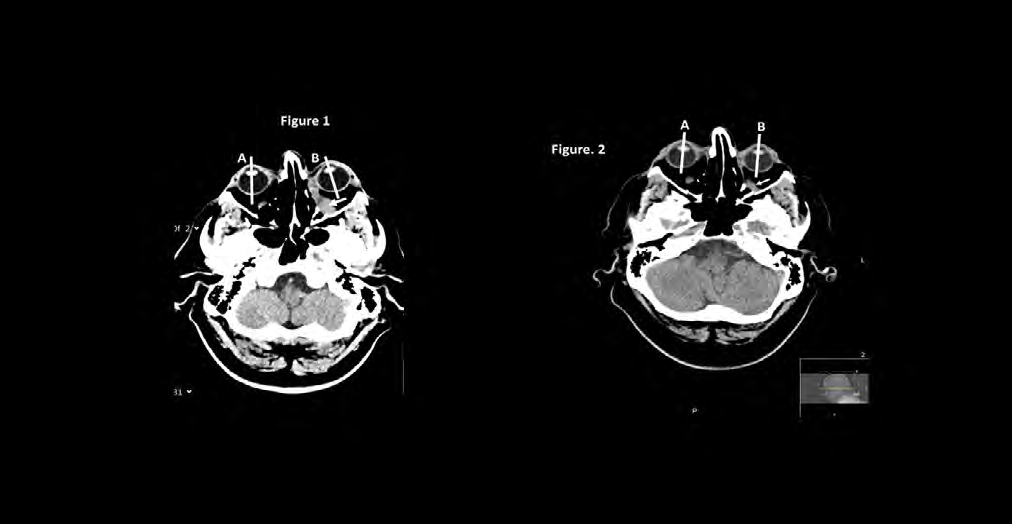
Figure 1: Computer tomography of a head shows left posterior intraorbital mass (GPA infiltrate) (white arrow), obstructing entrance of ocular nerve with internal deviation of left ocular nucleus (white A-B lines). Figure 2: Three months later after rituximab and corticosteroid therapy an angle between axial ocular lines of both eyes vanished and significant reduction of the inflammatory mass (arrow) followed.
Completely reversible oculomotor palsy VI and the vision restoration after only rituximab-corticosteroid therapy in GPA with intraorbital mass have not described. All patients also had immunosuppressive and cytotoxic treatment along with RTX [1, 2, 3, 4, 5]. Fifting years ago a case of abducens nerve palsy resulting from GPA pachymeningitis reported, with response to thirty mg per day of prednison only [6]. Recently, a case with headache and new left-sided hearing loss as relapse of GPA after failure of CS+IV endoxan (CY) reported. The patient got GC and RTX, and a 1-year remission followed [7]. The molecular mechanism of RTX is not fully understood. In this case, RTX was more effective with rapid and strong suppressing B cells than CY. Since the B cells count was proportional to the patients clinical manifestations, B cells represent a suitable target for the treatment of GPA with cranial neuropathies.
Anti-CD20 therapy used successfully in refractory granulomatous disease affecting the CNS: RTX is currently the drug most frequently used for remission induction in refractory orbital granuloma. Whereas an initial series on five patients reported inefficacy of rituximab, further case series composed of five to seven patients reported remission rates of 80–100% [8, 9]. Anti-TNF therapy (infliximab) may be option in refractory GPA [10].
References
-
Sharma A, Kunar S, Wanchu A, Lal V, Singh R, et al. (2010) Successful treatment of hypertrophic pachymeningitis in refractory Wegener’s granulomatosis with rituximab. Clin Rheumatol 29(1): 107-110.
-
Bawa S, Mukthyar C, Edmonds S, Webley M (2007) Refractory Wegener’s meningitis treated with rituximab. J Rheumatol 34(4): 900-901.
-
Julia U, Gross L (2011) Neurological involvement in Wegener’s granulomatosis. Current Opinion in Rheumatology 23(1): 7-11.
-
Peters JE, Gupta V, Saeed IT, Offiah C, Jawad ASM (2018) Severe localised granulomatosis with polyangiitis (Wegener’s granulomatosis) manifesting with extensive cranial nerve palsies and cranial diabetes insipidus: a case report and literature review. BMC Neurology 18(1): 59.
-
Oristrell J, Bejarano G, Jordana R, Monteagudo M, Marí B, et al. (2009) Effectiveness of Rituximab in Severe Wegener’s Granulomatosis: Report of Two Cases and Review of the Literature. Open Respir Med J 3: 94-99.
-
Kamimura T, Shimazaki H, Morita M, Nakano I, Okazaki H, et al. (2006) Limited Wegener’s Granulomatosis Manifested by Abducens Nerve Palsy Resulting From Pachymeningitis. J Clin Rheum 12(5): 259-260.
-
Nakazawa M, Suzuki K, Yasuoka H, Yamaoka K, Takeuchi T (2018) Successful rituximab treatment of granulomatosis with polyangiitis with cranial neuropathies. Inflammation and Regeneration 38: 20.
-
Taylor SR, Salama AD, Joshi L, Pusey CD, Lightman SL (2009) Rituximab is effective in the treatment of refractory ophthalmic Wegener’s granulomatosis. Arthritis Rheum 60(5): 1540-1547.
-
Martinez del Pero M, Chaudry A, Jones RB, Sivasothy P, Jani P, et al. (2009) B-cell depletion with rituximab for refractory head and neck Wegener’s granulomatosis: a cohort study. Clin Otolaryngol 34(4): 328-335.
-
Rozin A (2003) Infliximab efficiency in refractory Wegener’s granulomatosis. Rheumatology 42(9): 1124- 1125.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey