Case Report - A Lucky Ending of a Wearable Cardioverter-Defibrillator Failur
The Wearable Cardioverter-Defibrillator (WCD) is crucial for detecting and treating dangerous ventricular arrythmias. However, in a case involving a patient at high risk of sudden cardiac death (SCD) post myocardial infarction, the WCD failed to respond to an early life-threatening rhythm. A quick action by medical staff, fortunately saved the patient's life.
Abbreviations
WCD: Wearable Cardioverter Defibrillator; ICD: Implanted Cardioverter Defibrillator; SCD: Sudden Cardiac Death; VF: Ventricular Fibrillation; VT: Ventricular Tachycardia; CICU: Cardiovascular Intensive Care Unit AArD: Advanced Arrythmia Discriminator.
Introduction
While the implantable cardioverter defibrillator (ICD) is the standard treatment for preventing SCD due to ventricular arrhythmias, certain reversible clinical conditions may temporarily contraindicate its implantation. In such cases, the WCD serves as a valuable tool to protect patients against SCD. These external devices offer continuous monitoring of cardiac rhythm and possess the capability to detect potentially life-threatening arrhythmias and accurately administering electrical shocks when needed [1]. While the WCD exhibits excellent sensitivity and specificity in detecting ventricular tachyarrhythmias [2], the potential consequences of a failure to detect can be life-threatening. In this report, we present an exceptional case where the WCD failed to appropriately identify a ventricular fibrillation (VF) event, fortunately occurring within the confines of the cardiovascular intensive care unit (CICU).
History of Presentation
A 59-year-old patient brought to the hospital for rapidly worsening shortness of breath and orthopnea, starting 24 hours ago, following an episode of retrosternal chest pain. The patient had a medical history that included hypertension, dyslipidemia, type 2 diabetes, chronic obstructive pulmonary disease.
In the emergency department, the physical examination was unremarkable except for oxygen desaturation at 93% and fine bilateral basal crackles on lung auscultation.
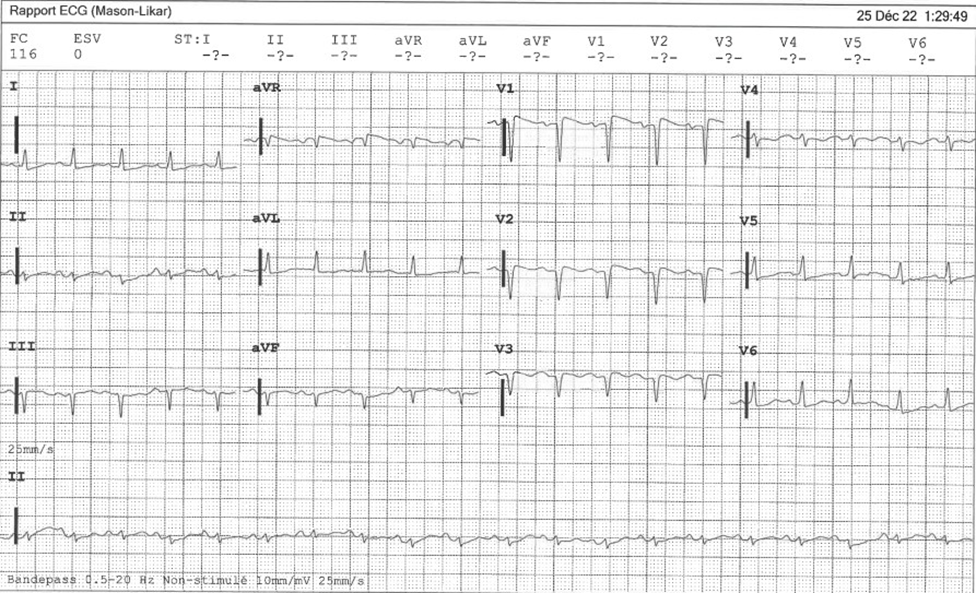
The electrocardiogram demonstrated a sinus tachycardia with normal PR and QRS intervals, as well as normal ST segments. However, pathologic Q waves were observed in the anteroseptal leads (Figure 1). The high sensitivity troponin level was markedly elevated at 22000 ng/L (reference value < 45 ng/L). The bedside cardiac ultrasound revealed a dilated left ventricle that was not hypertrophied, along with an impaired left ventricular ejection fraction at 30%.
Left heart catheterization was then conducted, and the patient was found to have subtotal occlusion in the mid left anterior descending artery and diffuse disease affecting the right coronary artery. Treatment involved a drug-eluting stent for the LAD artery occlusion, resulting in a favorable outcome. Seven days later, the RCA lesion was addressed. However, during this procedure, the patient experienced sustained VF, requiring termination with direct current cardioversion. Due to increased risk of sudden cardiac death and being within 40 days of myocardial infarction with an LVEF < 35%, the patient was provided with a LifeVest 4000, manufactured by ZOLL, following current ESC guidelines [3].
The WCD was programmed to detect ventricular tachycardia (VT) at 150 bpm and VF at 200 bpm. It would initiate therapy within 60 seconds for VT and 25 seconds for VF.
Three days after his first VF, the patient encountered a prolonged episode of sustained VF while still in his CICU bed, lasting approximately 50 seconds. In response to the WCD alert, the medical team promptly entered the patient’s room without making physical contact, adhering to the WCD protocol [4]. As the rhythm further deteriorated, the WCD was removed when the audible alarm ceased after 53 seconds from the onset of ventricular fibrillation (VF). This allowed for a 200 Joules direct current cardioversion using an automated external defibrillator, resulting in the restoration of consciousness and termination of the arrhythmia.
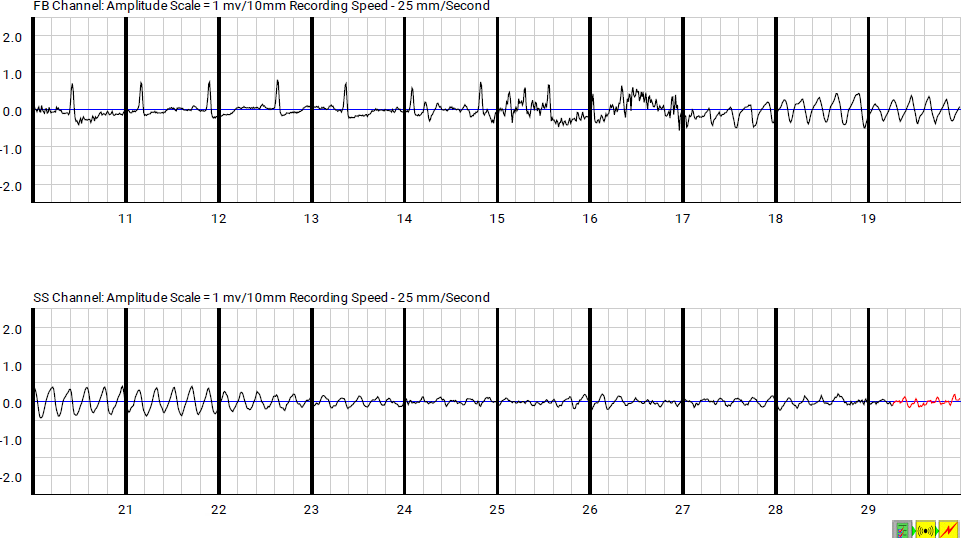
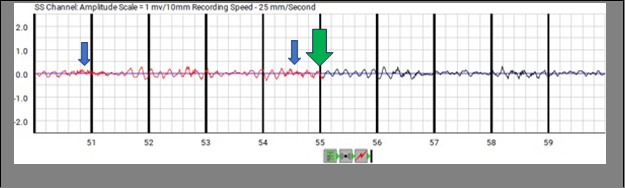
Upon analyzing the rhythm strips recorded by the WCD, it was observed that the patient’s normal sinus rhythm deteriorated into VF around the 17th second (Figure 2). The WCD correctly detected the VF and initiated the alarming system by the 29th second to assess the patient’s responsiveness, but eventually failed to deliver therapy within 25 seconds (Figures 2 & 3).
Following the initial event, the WCD was fully removed. Subsequently, the patient encountered recurrent life- threatening ventricular arrhythmias, necessitating sedation and intubation to end the electrical storm. Despite an extended hospitalization period and challenges with extubation, the patient was ultimately discharged without neurological sequelae.
Discussion
In this report, we present a case where a WCD failed to detect a critical, life-threatening VF and administer the necessary electrical shock.
The LifeVest WCD utilizes an advanced algorithm known as TruVector, which enables accurate analysis and treatment of ventricular tachyarrhythmias by considering both heart rate and rhythm morphology. Furthermore, the LifeVest is equipped with the capability to improve signal quality by detecting and mitigating ECG signal corruption [2]. The TruVector algorithm systematically assesses heart rate in relation to VT/VF thresholds. It categorizes heart rate based on frequency components, compares QRS morphology, and uses advanced arrhythmia discrimination (AArD) to differentiate patterns. Patient responsiveness is evaluated through alerts, and if no response occurs, the device delivers an immediate shock. This unique algorithm significantly reduces the risk of inappropriate shocks, ensuring the effectiveness of treatment [2].
Although the special characteristics of the WCD makes it very interesting to use in the daily practice, studies like VEST trial have demonstrated that patients with recent MI and reduced EF did not benefit from WCD as there was no reduction in the outcome of arrhythmic death compared to controls [5]. Making its indication a class IIb, level of evidence C in the current guidelines [3].
The WCD monitor was sent to ZOLL for analysis. Baseline ECG artifacts were observed in most leads, with a low amplitude, causing the AArD to remain inactive. However, the Tru Vector algorithm mistakenly identified these artifacts as motion artifacts, potentially due to minor patient convulsions. Consequently, the motion artifacts were mistakenly interpreted as signs of patient response to alerts and arousal, leading to a delay in treatment. (Figure 3). In addition to this potential explanation, it is worth considering the possibility of interference from the CICU scope patches, which cannot be completely dismissed. In an out-of-hospital setting, the WCD would likely conduct another analysis and algorithmic evaluation after the event, which would probably result in accurate rhythm detection and treatment, though there might be a few second’s delay. To our knowledge, there have been only a few reported cases of WCD failure, which regrettably have predominantly resulted in fatal outcomes [5, 6]. While the occurrence of SCD in WCD settings is relatively low, it is important to acknowledge that it can still happen due to non-arrhythmic causes or during electrical storms. The WEAR-IT study, for instance, reported a mortality rate of 2.1% among patients using WCDs, with these deaths attributed to factors unrelated to WCD failure [7].
Ethical Committee Approval
This case report has obtained ethical approval from the corresponding committee and adheres to all necessary ethical guidelines and regulations.
Conflict of Interest and Funding
None
Conclusion
WCDs are vital for preventing SCD in certain patients, but there can still be cases of missed ventricular arrythmias detection. There is a need for better arrhythmia detection algorithms to prevent rare yet potentially tragic scenarios.
References
-
Sandhu U, Rajyaguru C, Cheung CC, Morin DP, Lee BK (2019) The wearable cardioverter-defibrillator vest: Indications and ongoing questions. Prog Cardiovasc Dis 62(3): 256-264.
-
Vinas A, Roy D, Saunders C, Badin A, Pamday MM, et al. (2021) A Tragic Case of Wearable Cardioverter- Defibrillator Failure. JACC Case Re 3(2): 322-326.
-
Zeppenfeld K, Tfelt-Hansen J, Riva M de, Winkel BG, Behr ER, et al. (2022) 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 43(40): 3997-4126.
-
Lifevest System Overview (2019) Ohio Association of Physician Assistants.
-
Olgin JE, Pletcher MJ, Vittinghoff E, Wranicz J, Malik R, et al. (2018) Wearable Cardioverter–Defibrillator after Myocardial Infarction. N Engl J Med 379: 1205-1215.
-
Zhang L, Bhonsale A, Jain S (2022) A case of wearable defibrillator failure: How one lifesaving therapy delays another. J Cardiol Cases 25: 323-325.
-
Garcia R, Combes N, Defaye P, Narayanan K, Guedon- Moreau L, et al. (2020) Wearable cardioverter- defibrillator in patients with a transient risk of sudden cardiac death: the WEARIT-France cohort study. Europace 23(1): 73-81.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey