Reproducibility of Isometric Strength in Children with Cerebral Palsy
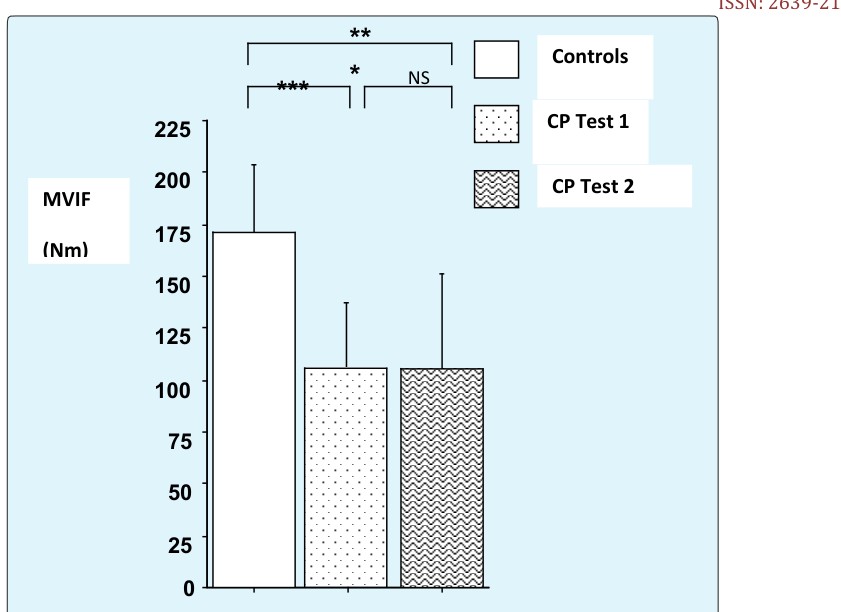
Physical activity is suggested to be beneficial for most children with cerebral palsy, whereas studies based on scientific results from reproducibility remain poorly known in such children. This study then asses the reproducibility of skeletal muscle function in children with spastic hemiplegic cerebral palsy, with a control able-bodied children. 16 children with cerebral palsy (Gross Motor Function Classification System Levels I and II), 10 males and six females, between 10 and 16 years of age) undertook two trial of assessment of skeletal muscle function with one week inter-test interval. 14 ablebodies aged-and sex-matched (10 boys and four girls) served as controls, undertaking only one test at the first trial. Quadriceps maximal voluntary isometric force (MVIF) and isometric endurance time (IET; contraction time to exhaustion at 50% of MVIF) were measured twice one week follow another week. Muscle strength (test1: 115±18.5 vs. Test2: 115±20.9 Nm-1, p=0.458), (and control: 171.1±23.8m-1, p
Introduction
Cerebral Palsy (CP) is a diagnosis based on an insult to the immature brain and resultant observed movement disorders, the maturation or development central nervous system function is often the focus of intervention [1]. Children with cerebral palsy are very weak compared to their able-bodies match controlled [2, 3]. Additionally, muscle weakness can be a major problem for many young people with spastic hemiplegic CP [2, 3, 4, 5]. The term “hemiplegia” refers to weakness and movement in coordination involving one side of the body [2, 6]. The majority of studies assessing muscle strength in children with CP use only functional measures of muscle strength without endurance time. Although functional measures of muscle strength are important indicators of a child’s motor ability, they do not quantify muscle force, lack the ability to detect small incremental changes in strength, and confounded by motor planning and control issues [5]. For another way, the evidence supporting the case for either inclusion or exclusion of strength training is based on sound scientific results from reproducible studies [3]. In general, further research of sufficient methodological quality is required to increase evidence on trainability after a good reproducibility of all fitness parameters and functional ability in children with cerebral palsy [2, 3]. Then, a better knowledge of the innocuity of sports, if correctly practiced, as well as a precise appreciation of the clinical and physiological parameters, should also help and overprotection and, eventually, to delay as long as possible the course towards cerebral palsy. An increasing number of studies have investigated assessment of strength in children with spastic CP [4, 5, 7, 8, 9]. However, most of the relevant literature consists of one trial of isokinetic and/or isometric contractions without reproducibility for almost. Whereas it is the best strategy of the validation of a test before apply the clinical feasibility of the programs [2, 3]. Quantitative measurement instruments have been shown to reliably assess muscle strength in children with and without neuromuscular disorders [9, 10, 11]. Indeed, an assessment tool may not be reliable in all patient populations and/or with all analysis system [12]. However there is a paucity of studies which use our current methodology to assess the reproducibility of muscle strength which assessed the responses to rehabilitation Accordingly, the objectives of this study are two folds: (i) To determine whether the strength and endurance during sustained isometric contraction of quadriceps femoris is reproducible in spastic hemiplegic CP kids, and (ii) To documented the methodology of the evaluation of the strength in children with CP., in the case of the optimization therapy in children with CP.
Methods
Participants
16 children with right hemiplegic CP, 10 boys and six girls classified as Gross Motor Function Classification System Levels I and II (as expanded and revised for children > 12 years [13] and 14 AB control subjects (10 boys and four girls) (ranging in age from 10 to 16 yrs old) participated in this study (Tables 1). Children and parents were informed about all aspects of the study, and written consent was obtained for protocol approved by a local ethic committee, in accordance with the Helsinki Declaration of 1975 and 1983, and in an investigation that met the ethical standards of this journal as detailed by Harris and Atkinson [14]. Children were excluded if they undergone a surgical procedure influencing mobility during the past year, were taking medication that could affect muscular function. A medical examination was performed and anthropometric data were collected on each subject. The clinical characteristics of the children with CP are stated in Table 1. A physician assessed the spasticity of each child, using the method of Ashworth (1964) [15]. All children were independently ambulatory and maturity was assessed by Tanner staging [16, 17]. All children were assigned in an assessment skeletal muscular function on an isokinetic apparatus twice in a separated week on the same day.
| Variable | Able-bodied | Children | ||||
|---|---|---|---|---|---|---|
| Controls | with CP | |||||
| (n=14) | (n=16) | |||||
| Age (years) | 14 ± 0.6 | 13 ± 1.9 | ||||
| Body mass (kg) | 55 ±11 | 44±9 | ||||
| Height (m) | 1.65±0.09 | 1.49 ±0.12** | ||||
| Sex | 10 boys | 10 boys | ||||
| 4 girls | 6 girls | |||||
| Hemiplegia | none | 16 | ||||
| GMFCS | none | Level I: 9, level II:7 | ||||
| Degree of Spasticity | none | I: 12, II: 4 | ||||
| Leg fat (%) | 13.7 ± 6.0 | 12.5±5.8 | ||||
| Leg volume (L) | 11.4 ± 2.6 | 10.3±1.6* | ||||
| Leg muscle volume (L) | 7.9 ± 2.4 | 6.8±1.6* |
Table 1: Clinical and anthropmetric characteristics, and sex of subjects.
CP = cerebral palsy, BMI = body mass index, * p< 0.01, **p< 0.001
Procedure
Anthropometric Measurements
Standing height, body mass, and body mass index were determined by standard anthropometric techniques. Fat mass, limb volume and limb muscles volumes for the legs were estimated from the individual's leg length (L), skin fold thicknesses (S, measured over the midthigh and mid- calf), 5 limb circumferences (C, ankle, mid-calf), knee, mid-thigh and groin), and the skinfold-corrected inter- condylar diameter (D), as detailed else were [18, 19]: Total leg volume = (SC2) L/62,8
Leg fat volume = (SC/5) (SS/4)L Bone volume = (0,235D)2 3,14 L Muscle volume Total leg volume – (fat + bones volumes)
Muscle Function Assessment
Maximal voluntary isometric force and static endurance time at an intensity level of 50% of maximal voluntary isometric force were determined using a Cybex dynamometer (Cybex Norm II; Lumex Inc, Ronkonkoma, NY) [6], Several studies have established the safety of such testing in CP [6, 7]. Chest and knee strapping maintained a consistent position; controls were tested at knee and hip angles of 60° and 120° respectively; angles for children with CP varied slightly, depending on available joint ranges, a practice trial ensured that the child understood procedures before definitive evaluations were made. Three sets of 5 maximal contractions were then performed, Verbal encouragement was provided and child watched the force developed on a computer monitor, A 20-sec recovery interval was allowed for each repetition, and a 1-minute interval for each set of contractions, The maximal force was considered as the average of the highest readings from each of the 3 sets. During the static endurance test, children maintained the contraction at a computer reference mark corresponding to 50% of their personal maximal force, Timing began as soon as the target force was attained, and subjects were informed of the elapse time every 15 seconds. The test was halted when the child could no longer maintain the contraction within 5% of the target value. A final 3 minutes of passive recovery was allowed following such testing, this protocol was undertaken in one week for all children follow another week for children with CP.
Statistical Analysis
Data were expressed as mean values ± standard deviation (SD). Data were analyzed using Stat View Software (SAS Institute Inc, SAS Campus Dr, Cary, North Carolina 27513, USA). Statistical Significance was set at p<0.05 throughout. We used a non parametric test to compare MVIF and SET parameters measured in the 2 repeated isometric tests in children with cerebral palsy and between children with cerebral palsy and control children because that the distribution of data in CP is skewed, with some subjects showing much poorer reproducibility than others. Relationships between the first test and the second test were determined by using a regression analysis. Test-retest reliability was examined using Spearman correlation coefficients (r), intra class correlation coefficients (ICCs) and Bland-Altman plots [1986] [20]; 95% of the data for isometric strength and endurance parameters fell within the limits of the corresponding Bland-Altman plots, as required for an acceptable repeatability of data [1986]. Assuming the mean difference between the first and second measurements to be zero, the COR for the Bland-Altman test is derived as follows Where x1 and x2 are the mean values for the first and second measurements and n is the number of subjects. Bland-Altman plots were generated to show the relationship between inter-measurement differences and their average, together with the limits of agreement (mean difference, ±2SDs) [20].
Results
Participants
18 children with cerebral palsy and 14 AB control children were initially recruited. 2 children with cerebral palsy did not complete the study because there were unwilling to sustain the isometric force due to their extra equinovarum legs. 30 children thus completed the entire study.
Physical and Anthropometric Characteristics
Physical and anthropometric characteristics are showed in Table 1.
Reproducibility of the Maximal Voluntary Isometric Force
Values of the 2 repeated MVIF obtained during isometric contraction of quadriceps and Bland-Altman Plot is shown in figures 1 and 3 respectively. No statistical difference was found between the 2 repeated MVIF (tests 1 and 2, p=0.458). Moreover, high correlation coefficients were obtained between the two repeated tests (r=0.87, p<0.01, ICC=0.84).
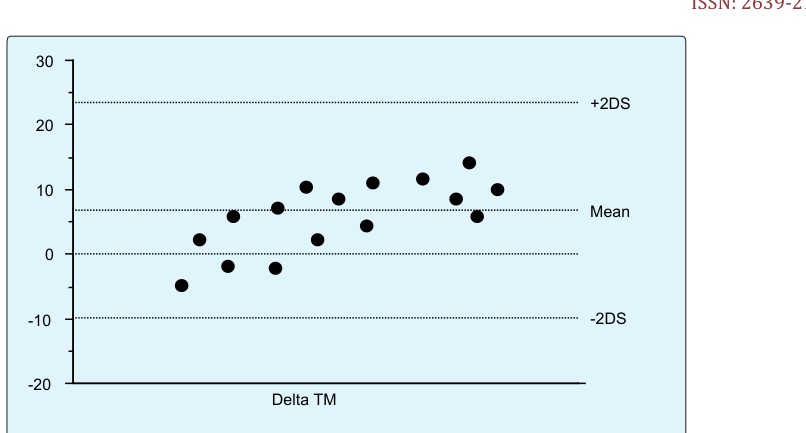
Bland-Altman plot shows a good agreement between the two repeated measures for all variables assessed.
Reproducibility of the Static Endurance Time (SET) parameters
Values of the 2 repeated SET obtained during isometric contraction of quadriceps and Bland-Altman Plot are shown in figures 2 and 4 respectively. No statistical difference was found between the 2 repeated SET (tests 1 and 2, p=0.479). Moreover, high correlation coefficients were obtained between the two repeated tests (r=0.94, p<0.01, ICC=0.89). Bland-Altman plot shows a good agreement between the two repeated measures for all variables assessed.
Discussion
In this study, reliability of skeletal muscle function measured by Cybex Norm II during isometric contraction was examined in a homogeneous group of right hemiplegic children with CP classified to GMFCS-level I and II. In our study, we tested the affected leg because we wanted to validate the protocol in the altered leg. The population of this study was right hemiplegic cerebral palsy, and we compared the results of their isometric strength with the right leg of their able-bodied match children. However must studies of strength in children with cerebral palsy only use the unaffected leg as controlled but do not get healthy controlled children [21, 22]. Moreover those studies do not do Bland and Altman plot. Where as to be more relevant in clinical practice, a tool of evaluation should compared the results of the research between disability population and typically developing. Additionally, for a clinical reproducibility study, Bland and Altman should be plotted to show a good agreement between the repeated measures for all variables assessed, and to clarify and attest the use of interclass correlation coefficient in the evaluation of the agreement [20, 23]. It is obvious that reproducibility is the hallmark of science. Therefore, given that the population of our study was homogeneity, we used ICC. It was assumed that, it is useful to use also SEM and SDD on sample heterogeneity [22]. In their study, Willemse et al 2013 [22] found that hand-held dynamometry is reliable and can be used to detect changes in isometric muscle strength in children with CP when using the mean of at least 2 trials. They also say that to further improve reliability, taking the average of 2 occasions on separated days is recommended, depending on group size and muscle group. Indeed, although the protocol is not quite the same, we agree closely with Willemse et al. (2013) [22]. We reported a reproducibility of isometric strength and endurance in children with cerebral palsy when participants were tested twice at an interval of 1 week. In support of this view, Ayalon et al. (2000) [21] evaluates the reliability of isokinetic testing of Knee flexors and extensors in children with CP. They concluded that the finding indicate that measuring isokinetic strength in the tested population is highly reliable and should be considered in rehabilitation protocols. Unfortunately, their study does not included endurance test and the participants in their study represent heterogeneity sample of children with CP. Our sampling was larger of the participant's capacity and confirmed the higher reliability that was manifested by the ICC. Molnar et al. (1979) [10] also investigated the reliability of isokinetic testing on a variety of muscle groups of the lower and upper extremities in children aged 7 to 15 years. They confirmed that isokinetic testing is simple to conduct and highly reliable for typically developing children with normal intelligence as well a children with minor learning disability. Similarly, Damiano et al. (1999) [9] argued that manuel muscle testing (MMT) and hand-held dynamometry are the most commonly used methods to assess strength both in clinical practice and in research. Our study confirmed those [9]. Most of these studies on reproducibility of isometric strength in children with CP forsake the endurance time during the sustained force. However, the outcome of the endurance time could be a good index of a relevant reproducibility. We can argue that static endurance time at 50% of individual's maximal voluntary torque is a parameter of the isometric strength. This in turn might suggest that static endurance time could enhance the ability of child with CP to sustain isometric concentrations. One important limitation to the interpretation of correlation coefficients is that they are very sensitive to the range of values studied [23], with higher ICCs if the range of values is wide. Moreover, even a high inter-test correlation does not necessary imply that a measurement is reproducible. Most previous investigators have used arbitrary cut-off values to rate the reproducibility of data [24, 25]. Nadler et al. (2000) [24] accepted an ICC >0.75 as indicative of good reliability and Portney and Watkins defined values <0.75 as having poor to moderate reliability; others have required an ICC of 0.80 for an acceptable test. Adopting the 0.75 cut-off, one would conclude that in children with hemiplegic cerebral palsy, the Cybex Norm dynamometer yields several MVIF and SET measurements that have a satisfactory level of reproducibility over a one-week interval. The coefficient of reproducibility (COR) of Bland and Altman (1986) [20] can be more informative than either the ICC or the CV.
Thus, a COR of 115 Nm for strength in children with cerebral palsy implies that 95% of inter-test differences were less than 115 Nm. This is important practical information for the clinician who must decide whether an apparent improvement in gait cycle is due to measurement variability or a response to treatment. The COR value is also helpful in calculating minimum sample sizes when designing a study of group responses to treatment [23, 26]. Testing of the reproducibility of quadriceps femoris isometric strength may therefore be important for treatment planning or for assessing the effectiveness of treatment.
Conclusion
Results of this repeated sustained isometric contraction of quadriceps support the view that home- based on reproducibility test programmes is a prerequisite to validate the feasibility of a protocol before apply it use. Forward, our study showed good reproducibility of isometric voluntary maximal force and static endurance time in children with spastic hemiplegic CP classified at Gross Motor Function Classification level I and II, suggesting the utility of using the sustained isometric test as a valid tool to measure strength in clinical rehabilitation.
Acknowledgement
We acknowledge the cooperation and expert technical assistance of the medical staff of the cerebral palsy center during data collection and processing, and the generous cooperation of the children and parents participating in this study. The authors disclose any potential conflict of interest.
References
-
Bobath K (1969) The motor Deficits in Patients with Cerebral Palsy. Heinimann London.
-
Nsenga AL, Shephard RJ, Ahmaidi S (2013) Aerobic Training in Children with Cerebral Palsy. Int J Sports Med 34: 533-537.
-
Nsenga Leunkeu A, Lelard T, Shephard RJ, Doutrellot PL, Ahmaidi S (2014) Gait cycle and plantar pressure distribution in children with cerebral palsy: Clinically useful outcome measures for a management and rehabilitation. Neuro Rehabil 35(4): 6570-6663.
-
Engsberg JR, Ross SA, Olree KS, Park TS (2000) Ankle spasticity and strength in children with spastic diplegic cerebral palsy. Dev Med Child Neurol 42(1): 42-47.
-
Buckon CE, Thomas SS, Harris GE, Piatt JH, Aiona MD, et al. (2002) Objective measurement of muscle strength in children with spastic diplegia after selective dorsal rhizotomy. Arch Phys Med Rehabil 83(4): 454-460.
-
Leunkeu AN, Keefer JD, Miladi I, Ahmadi S (2010) Electromyographic (EMG) Analysis of quadriceps femoris muscle fatigue in children with cerebral palsy during a sustained isometric contraction. J Child Neurol 25(3): 287-293.
-
Damiano DL, Martellotta TL, Sullivan DJ, Granata KP, Abel MF (2000) Muscle force production and functional performance in spastic cerebral palsy: relationship of cocontraction. Arch Phys Med Rehabil 81(7): 895-900.
-
Elder GC, Kirk J, Stewart G, Cook K, Weir D, et al. (2003) Contributing factors to muscle weakness in children with cerebral palsy. Dev Med Child Neurol 45(8): 542-550.
-
Damiano DL, Abel MF, Panuzzio M, Romano JP (1999) Interrelationships of strength and gait before and after hamstring lenthening. J Pediatr Orthop 19(3): 353-358.
-
Molnar GE, Alexander J, Gutfeld N (1979) Reliability of quantitative strength measurements in children. Arch Phys Med Rehabil 60(5): 218-221.
-
Stackhouse SK, Binder-Macleod SA, Lee SCK (2005) Voluntary muscle activation, contractile properties, and fatigability in children with cerebral palsy. Muscle Nerve 31(5): 594-601.
-
Sorsdahl AB, Moe-Nilssen R, Strand LI (2008) Test- retest reliability of spatio and temporal parameters in children with cerebral palsy measured by and electronic walkway. Gait and Posture 27(1): 43-50.
-
Palisano R, Hana SE, Rosenbaum P, Russell DJ, Walter SD, et al. (2000) Validation of a model of Gross Motor Function for children with Cerebral Palsy. Phys Ther 80(10): 974-985.
-
Harris DJ, Atkinson G (2011) Update – ethical standards in sport and exercise science research. Int J Sports Med 32(11): 819-821.
-
Ashworth B (1964) Preliminary trial of carisoprodol in multiple sclerosis. Practitioner 192:540-542.
-
Worley G, Houlihan CM, Herman-Giddens ME, O'Donnell ME, Conaway M, et al. (2002) Secondary sexual characteristics in children with cerebral palsy and moderate to severe motor impairement: a cross- sectional survey. Pediatrics 110(5): 897-902.
-
Henderson RC, Gilbert SR, Clement ME, Abbas A, Worley G, et al. (2005) skeletal maturation in moderate to severe cerebral palsy. Dev Med Child Neurol 47(4): 229-236.
-
Shephard RJ, Vandewalle H, Boudel E, Monod H (1988) Muscle mass as a factor limiting physical work. J Appl Physiol 64(4): 1472-1479.
-
Samsong-Fang LJ, Stevenson RD (2000) Identification of malnutrition in children with cerebral palsy: poor performance of weight-for-height centiles. Dev Med Child Neurol 42(3): 162-168.
-
Bland JM, Altman DG (1986) Stastical methods for assessing agreement between two methods of clinical measurement. Lancet 8(1): 307-310.
-
Ayalon M, Ben-Sira D, Hutzler Y, Gilad T (2000) Reliability of isokinetic strength measurements of the knee in children with cerebral palsy. Dev Med Child Neurol 42(6): 398-402.
-
Willemse L, Brehm MA, Scholtes VA, Jansen L, Woudenberg-Vos H (2013) Reliability of isometric lower-extremity muscle strength measurements in children with cerebral palsy: implication for measurements design. Phys Ther 93(7): 935-941.
-
Bland JM, Altman DG (1990) A note of the use of intraclass correlation coefficient in the evaluation of agreement between two methods of measurement. Compt Biol Med 20(5): 337-340.
-
Nadler SF, DePrince ML, HauesienN, Malanga GA, Stilik TP, et al. (2000) Portable dynamometer anchoring station for measuring strength of hip extensors and abductors. Arch Phys Med Rehabil 81(8): 1077-1076.
-
Portney LG, Watkins MP, Foundations of clinical research: Application to practice. 2nd (ed.) Upper Saddle River, NJ, Prentice Hall.
-
Van den Linden ML, Aitchison AM, Hazlewood ME, Hillman SJ, Robb JE (2004) Test-retest repeatability dynamometer in children with cerebral palsy. Arch Phys Med Rehabil 85(12): 2058-2063.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury