Covid-Induced Dystonia and Opsoclonus: A Case Report
Intro: New onset movement disorders are being reported following infection with the SARS-CoV-2 virus. These include myoclonus, tremor, oculomotor disorders, ataxia, akinetic rigid syndrome, catatonia, dystonia, and chorea. IVIG and steroids are shown to improve these neurological manifestations. Narrative: We present a case of a 74-year-old female with multiple comorbidities who developed opsoclonus, upper extremity dystonia, and encephalopathy following infection with COVID-19. Discussion: Currently, no cases have been reported on the combination of dystonia, opsoclonus, and encephalopathy in the presence of COVID-19. Due to the patient's minimal improvement following treatment, more research will need to be done on this topic to tailor pharmacotherapy for the neurological manifestations of this virus. Conclusion: Diagnosing movement disorders following infection with COVID-19 remains controversial. This case highlights the complexity of ruling out other etiologies that could lead to these neurological symptoms and the importance of comprehensive patient care and symptom management.
Introduction
SARS-CoV-2 virus (COVID-19) predominantly affects the respiratory system, however, there has been an increase in the spectrum of neurological manifestations of the disease. New onset movement disorders are being reported both during the disease course and post- infection. These include but are not limited to myoclonus, tremor, oculomotor disorders, ataxia, akinetic rigid syndrome, catatonia, dystonia, and chorea [1]. Dystonia, the involuntary repetitive contraction of a muscle, is one of the rarest movement disorders reported during infection with COVID-19, making up only 1-3% of all cases [2, 3].
Myoclonus, rhythmic jerking movements, is one of the most common movement disorders associated with the virus and can coincide with opsoclonus, ataxia and occasionally altered mental status (OMAS) [1, 2]. Opsoclonus is defined as conjugate saccades in all directions and has been seen in COVID-19 patients with more severe disease, often affecting those in the intensive care unit [1, 4]. Currently, immunotherapy and steroids show benefits early in the disease course in immune-mediated movement disorders like OMAS and dystonia [5, 6].
We report a patient presenting with opsoclonus, dystonia, and encephalopathy secondary to COVID-19 infection.
Narrative
The patient is a 74-year-old Caucasian female with a past medical history of hypertension, hyperlipidemia, hypothyroidism, obstructive sleep apnea, coronary artery disease, and a right frontal ischemic stroke due to cardioembolism leading to residual aphasia 2012.
She presented to the emergency department via emergency medical services with a chief complaint of generalized weakness and decreased appetite. The patient was unable to stand up from the toilet due to her leg weakness and therefore called the paramedics. She noted that she recently stopped semaglutide injections due to intolerance. In addition to low appetite the patient endorsed sore throat and cough for the past two weeks. The patient had no other symptoms or concerns upon admission.
An initial exam showed 5/5 strength in her bilateral upper and lower extremities. Coordination and cranial nerves were intact. She was alert and oriented to person and place but not time or situation. She recalled 1/3 items on short- term memory evaluation. In conversation, her responses were delayed. The family reported her presentation was significantly reduced from baseline.
In the following days, the patient developed acute onset opsoclonus and bilateral hand dystonia. Her cognition continued to wax and wane. On day nine, she began to experience visual and auditory hallucinations.
| Patient Value | Reference Range | |
|---|---|---|
| Sodium | 137 | 135 - 145 mmol/L |
| Potassium | 2.6 | 3.5 - 5.0 mmol/L |
| Chloride | 94 | 98 - 111 mmol/L |
| WBC Count | 4.9 | 3.8 - 10.6 K/uL |
| CO2 | 26 | 21 - 35 mmol/L |
| TSH | 2.3 | 0.40 - 7.50 uIU/mL |
| Vitamin B-12 | 769 | 180 - 810 pg/mL |
| Ammonia | 25 | 18 - 50 umol/L |
| CPK | 35 | <178 IU/L |
| SARS-CoV-2 RT-PCR | Detected | Not Detected |
Table 1: ** Initial laboratory tests upon admission.
WBC, white blood cell count; CO2, carbon dioxide; TSH, thyroid stimulating hormone; CPK, creatine phosphokinase. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; RT-PCR, reverse transcription-polymerase chain reaction. Table 1: Initial laboratory tests upon admission.
The diagnostic workup for the patient was comprehensive. The patient had a positive COVID-19 PCR on admission. Her initial CMP demonstrated some electrolyte abnormalities, including hypokalemia and hypochloremia. TSH, B12, Ammonia, and CPK were all within normal limits (Table 1). Arterial blood gas (ABG) showed a pO2 of 72.2, a pCO2 of 27.7, and a pH of 7.54. She was placed on 8L high- flow nasal cannula. Repeat ABG demonstrated improvement with pO2 of 141, pCO2 of 30.4, and pH of 7.51. The patient was weaned down to room air throughout her admission. The patient had no other significant lab abnormalities during her workup that explained her symptoms.
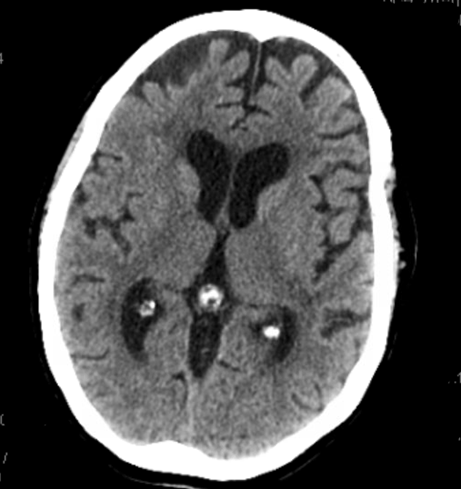
Additionally, the patient underwent multiple imaging studies, including CT without contrast and an MRI with and without contrast, all of which revealed no significant pathology of note besides her chronic frontal lobe infarct from 2002 (Figure 1). The patient received an EEG demonstrating mild diffuse slowing but no other focal epileptiform features. A decision was made to defer lumbar puncture at this time, as it was unlikely to change the patient’s management, and the patient was also concurrently taking clopidogrel.
The initial treatment focused on addressing the patient’s metabolic derangements. IV potassium and nutritional support were administered. Hospital acquired delirium was suspected and sleep was optimized with melatonin (6 mg oral nightly) and Seroquel (25 mg oral nightly). However, Seroquel and Melatonin were discontinued and replaced with Valium (10 mg oral nightly) and Benadryl (25 mg oral nightly) to ensure that Seroquel did not exacerbate the patient’s symptoms. Additionally, Trihexyphenidyl (2 mg oral, TID) was initiated to manage dystonia, but the patient reported no improvement with this treatment. After reviewing the literature, it was suggested that the symptoms might be SARS-CoV-2 induced. Consequently, the patient commenced IVIG therapy at a dose of 400 mg/kg for five days, as some literature suggested this could be an effective treatment for patients with novel COVID-induced movement disorders.
Despite these interventions, the patient’s dystonia and opsoclonus showed no response. A 5-day course of intravenous immunoglobulin (IVIG) yielded no improvement, and two weeks later, there was no change in cognition, dystonia, or opsoclonus. Considering the unresponsive symptoms, the decision was made to transfer the patient to a larger academic facility for further exploration of treatment options unavailable at the current community facility.
Discussion
At this time, dystonia remains one of the rarest reported movement disorders associated with the corona virus [7]. It is currently a diagnosis of exclusion, and we had to consider her medical history, medications, and multiple comorbidities as an underlying cause. The etiology of dystonia can be vast, and most of the time an exact cause cannot be identified [8]. Risk factors include smoking and a history of partaking in regularly skillful, precise movements [9]. Due to her late symptom onset, and absent family history of the movement disorder, it was hypothesized her dystonia was acquired. Acquired causes include neoplastic, brain injury, metabolic, toxic, vascular, infectious, and drug-induced dystonia [10]. It is important to note that although the patient’s case was complicated by semaglutide induced metabolic disturbances, hypoxemia, and hospital acquired delirium, these issues were all corrected for throughout her hospital stay and despite these corrections the patient did not improve. This, combined with the patients’ unremarkable, comprehensive blood work, absence of medications that could lead to dystonia, and lack of improvement with nutritional supplementation made neoplastic, metabolic, toxic, and drug-induced dystonia less likely the cause of her symptoms. The literature suggested that trihexyphenidyl is the most effective pharmacotherapy to treat dystonia. However, our patient showed no improvement following administration of the drug. This led us to expand our work-up and consider other treatment options.
Stroke was also considered as an acquired etiology. This was due to the patient’s acute onset of symptoms, cardiac risk factors, and prior cerebrovascular history. Recent literature proposed that the COVID-19 virus could lead to ischemic stroke through multiple mechanisms. These mechanisms include COVID-induced hypercoagulability, decreased activation of the renin-angiotensin system, cardiac embolism, and endothelial cell dysfunction [11]. The sars-CoV-2 virus binds to the ACE-2 receptor which plays a key role in vasoregulation. This could potentially cause cerebrovascular dysfunction resulting in decreased tissue perfusion [12]. Also, patients with COVID-19 have been found to have elevated D-dimer, and Von Willebrand factor. When combined with endothelial dysfunction this may result in a hypercoagulable state increasing the risk for stoke [13]. Lastly, severe COVID-19 can lead to hypoxemia through respiratory distress. Diminished oxygen to the brain can lead to increased oxidative stress, which in turn can produce vascular changes [14]. While our patient did experience hypoxemia, her bilateral dystonia symptoms and negative MRI made this etiology less likely.
After ruling out all other etiologies, infection was thought to be the primary cause of our patients’ symptoms. Franke, et aldescribed a patient similar to our case, where a 78-year-old experienced upper extremity dystonia along with delirium after a diagnosis of COVID-19. However, this is one of the only other cases we have found. Direct neural invasion could be a proposed mechanism for the development of dystonia. Surprisingly, angiotensin-converting enzyme 2 receptors (ACE-2) have been found in the basal ganglia [15]. This would allow the virus a direct pathway to bind to the brain structure that controls and modulates movement. There are reports of antibodies against the virus being found in cerebral spinal fluid, supporting direct neural invasion as a mechanism [16, 17]. The temporal relationship between the onset of COVID-19 and the emergence of opsoclonus and dystonia supports the association between the viral infection and the neurological manifestations.
To expand on the patients opsoclonus, this movement disorder is typically due to paraneoplastic syndromes, but in the presence of COVID-19, opsoclonus usually manifests with ataxia and myoclonus [1, 18, 19]. This patient was unique in the sense that her opsoclonus presented at the same time as her dystonia in the absence of myoclonus. Due to the patient’s weakness and bilateral hand dystonia, it was difficult to assess this patient for ataxia. Opsoclonus typically results from immune-mediated damage to the cerebellum and is another proposed mechanism of COVID- 19-induced neurological manifestations [4]. It is important to note that opsoclonus can be a side effect of medications and hypoxia [19]. After reviewing the patient’s medications and correcting her hypoxia her opsoclonus remained. So, it was proposed that along with dystonia her opsoclonus was caused by the virus.
Considering this patient’s lack of improvement during her stay, the decision was made to treat with IVIG. While there is no current best practice for managing these symptoms, intravenous immunoglobulin is considered a safe option with benefits previously observed in patients of similar presentation [2]. Two weeks following treatment, the patient did not show any significant improvement. Therefore, the question currently remains what the true etiology and pathophysiology is behind this patient’s neurological symptoms. A case series following several patients with neurological manifestations of COVID-19 did not show complete improvement following the administration of IVIG [20]. Therefore, IVIG may not be the best treatment for all patients with neurological manifestations, but at this time, it is one of the only available options. Due to the lack of literature on this topic, the patient needs continued observation and appropriate adjustment to medical management based on treatment response.
The rapid decline and fluctuating symptoms of this patient highlight the complexity of COVID-19 associated neurological manifestations. While severe, these complications remain rare; thus, proper recognition and treatment are challenging.
Conclusion
De novo movement disorders due to COVID-19 continue to be a rare manifestation of the disease, and there is limited literature on the topic. Currently, they remain a diagnosis of exclusion, and there is still controversy as to whether COVID-19 is the culprit or if other etiologies are being missed. This case highlights the complexity of diagnosing movement disorders in a patient with multiple comorbidities in the presence of COVID-19 and the need for a comprehensive approach when managing these patients.
References
-
Fung WKW, Fasano A, Fearon C (2023) Movement Disorders and SARS-CoV-2. Mov Disord Clin Pract 10(2): S9-S17.
-
Brandao PRP, Grippe TC, Pereira DC, Munhoz RP, Cardoso F (2021) New-onset movement disorders associated with covid-19. Tremor Other Hyperkinet Mov 11(1): 26.
-
Jinnah HA, Factor SA (2015) Diagnosis and Treatment of Dystonia. Neurol Clin 33(1): 77-100.
-
Oh SY, Kim JS, Dieterich M (2019) Update on opsoclonus- myoclonus syndrome in adults. J Neurol 266(6): 1541- 1548.
-
Foucard C, San-Galli A, Tarrano C, Chaumont H, Lannuzel A, et al. (2021) Acute cerebellar ataxia and myoclonus with or without opsoclonus: a para-infectious syndrome associated with COVID-19. Eur J Neurol 28(10): 3533- 3536.
-
Mohammad SS, Dale RC (2018) Principles and approaches to the treatment of immune-mediated movement disorders. Eur J Paediatr Neurol 22(2): 292- 300.
-
Thiel MF, Jost WH (2023) Incidence of dystonia related to COVID-19 infection. Neurol Neurochir Pol 57(1): 140- 141.
-
Mohamed AA, Faragalla S, Khan A, Flynn G, Rainone G, et al. (2024) Neurosurgical and pharmacological management of dystonia. World J Psychiatry 14(5): 624- 634.
-
Vidailhet M, Grabli D, Roze E (2009) Pathophysiology of dystonia. Curr Opin Neurol 22(4): 406-413.
-
Grutz K, Klein C (2021) Dystonia updates: definition, nomenclature, clinical classification, and etiology. J Neural Transm (Vienna) 128(4): 395-404.
-
Sagris D, Papanikolaou A, Kvernland A, Korompoki E, Frontera JA, et al. (2021) COVID-19 and ischemic stroke. Eur J Neurol 28(11): 3826-3836.
-
Fatehi P, Hesam-Shariati N, Abouzaripour M, Fathi F, Hesam Shariati MB (2020) Acute Ischemic and Hemorrhagic Stroke and COVID-19: Case Series. SN Compr Clin Med 2(11): 2396-2401.
-
Small C, Mehkri Y, Panther E, Felisma P, Lucke-Wold B (2023) Coronavirus Disease-2019 and Stroke: Pathophysiology and Management. Can J Neurol Sci 50(4): 495-502.
-
Yang Y, Rosenberg GA (2011) Blood-brain barrier breakdown in acute and chronic cerebrovascular disease. Stroke 42(11): 3323-3328.
-
Franke C, Ferse C, Kreye J, Reincke SM, Sanchez-Sendin E, et al. (2021) High frequency of cerebrospinal fluid autoantibodies in COVID-19 patients with neurological symptoms. Brain Behav Immun 93: 415-419.
-
Rodriguez-Perez AI, Garrido-Gil P, Pedrosa MA, Garcia- Garrote M, Valenzuela R, et al. (2020) Angiotensin type 2 receptors: Role in aging and neuroinflammation in the substantia nigra. Brain Behav Immun 87: 256-271.
-
Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-Leon J, et al. (2021) Neurological and Neuropsychiatric Impacts of COVID-19 Pandemic. Can J Neurol Sci 48(1): 9-24.
-
Pillai KS, et al. (2023) De Novo Movement Disorders Associated with COVID-19- A Systematic Review of Individual Patients. Ann Indian Acad Neurol 26(5): 702- 707.
-
Przytuła F, Slawek J (2023) Hyperkinetic movement disorders following SARS-CoV-2 infection and vaccination - an update. Neurol Neurochir Pol 57(1): 63- 76.
-
Paterson RW, Brown RL, Benjamin L, Nortley R, Wiethoff S, et al. (2020) The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain 143(10): 3104-3120.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury
- Seepage and Swelling-Neuroendocrine Tumour Testis