Seepage and Swelling-Neuroendocrine Tumour Testis
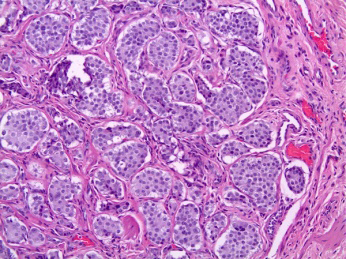
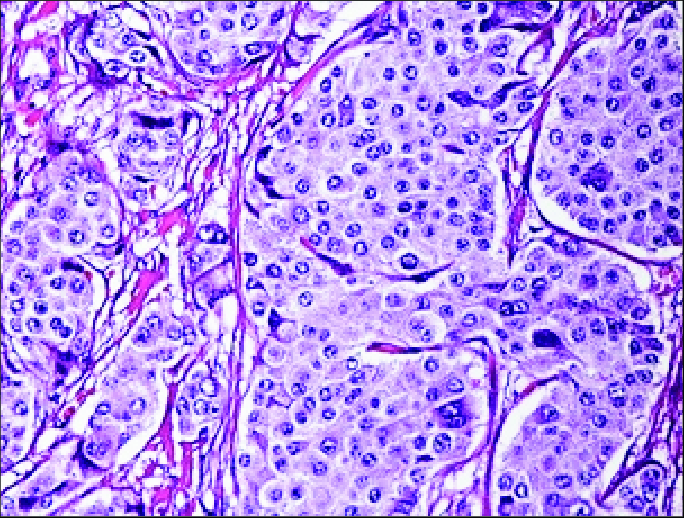
Neuroendocrine tumour of testis configures a well differentiated neuroendocrine tumour or a low grade, epithelial neoplasm demonstrating neuroendocrine differentiation. Testicular neuroendocrine tumour may concur with pre-pubertal teratoma or exceptionally articulate as a post-pubertal subtype. Tumour cells manifest with a near diploid genotype. Tumour cells appear devoid of is chromosome 12p or numerical aberrations confined to X chromosome. Cytological examination exhibits isolated singular cells or sheets of neoplastic cells permeated with granular cytoplasm, uniform, spherical nuclei and evenly distributed, fine nuclear chromatin. Morphologically, tumefaction exhibits cellular nests, glands with intra-luminal mucin, solid sheets, insular, acinar or trabecular pattern of tumour evolution. Monomorphic neoplastic cells are pervaded with abundant, granular, eosinophilic cytoplasm, regular spherical nuclei and fine or salt and pepper nuclear chromatin, encompassed within a delicate, fibrous or hyalinised stroma
Introduction
Neuroendocrine tumour of testis emerges as a well differentiated neuroendocrine tumour or a low grade, epithelial neoplasm demonstrating neuroendocrine differentiation. Additionally designated as pure neuroendocrine tumour, testicular neuroendocrine tumour, pre-pubertal subtype or post-pubertal subtype of neuroendocrine tumour or monodermal teratoma, tumefaction appears devoid of concordance with germ cell neoplasia in situ (GCNIS) and isochromosome 12p. Nevertheless, nomenclature as carcinoid, atypical carcinoid, neuroendocrine carcinoma or neuroendocrine tumour not otherwise specified (NOS) is not recommended.
Primary testicular neuroendocrine tumour predominantly (~75%) manifests as a pure neoplasm or appears associated with teratoma (~25%). Tumefaction expounds a predominantly insular or trabecular neoplastic pattern. Tumour cell nuclei are incorporated with salt and pepper nuclear chromatin. Neuroendocrine tumour (NET) predominantly incriminates renal parenchyma, urinary bladder, prostate, testicles or urethra whereas genitourinary tract is infrequently implicated. Distant metastasis into testis, arising from neuroendocrine tumour confined to sites as pulmonary parenchyma or gastrointestinal tract is documented. The extremely exceptional neoplasm configures an estimated < 1% of testicular neoplasms. Ovaries are frequently incriminated, in contrast to testes with a proportion of 15:1
[1, 2]. Mean age of disease representation is 46 years whereas tumefaction may emerge within 10 years to 83 years. Caucasian population is commonly implicated, in contrast to Asians or Africans [1, 2]. Of obscure aetiology, testicular neuroendocrine tumour may emerge in concurrence with pre-pubertal teratoma and may be designated as testicular neuroendocrine tumour, pre-pubertal subtype. Post- pubertal subtype of testicular neuroendocrine tumour may exceptionally be documented [1, 2]. Majority (~75%) of neoplasms appear as ‘pure’ neuroendocrine tumours whereas ~25% tumours concur with various teratomatous components as dermoid cyst or epidermoid cyst. Preponderantly, testicular neuroendocrine tumour appears non concurrent with germ cell neoplasia in situ (GCNIS) or isochromosome 12p. Assessment of DNA ploidy enunciates tumour cells with near diploid genotype [2, 3]. As testicular neuroendocrine tumour appears non concurrent with germ cell neoplasia in situ, tumour cells appear devoid of isochromosome 12p or numerical aberrations confined to X chromosome, in contrast to germ cell neoplasia in situ associated testicular germ cell tumours. Assessment of isochromosome 12p may be exceptionally adopted within post-pubertal subtype of germ cell tumours [2, 3]. Testicular neuroendocrine tumour commonly represents as a testicular tumefaction or swelling. Testicular pain may or may not ensue. Incrimination of bilateral testis is uncommon. Infrequently, neoplasm appears concordant with cryptorchidism. Nearly 10% lesions concur with conditions such as hydrocele. Up to 12% neoplasms exhibit clinical features of carcinoid syndrome as hot flushes, diarrhoea or palpitation. Distant metastases with haematogenous dissemination may occur into pulmonary parenchyma, hepatic parenchyma, bones, soft tissue, cutaneous surfaces, heart or contralateral testis. Additionally, tumour dissemination through the lymphatic tract may ensue [2, 3]. Cytological examination exhibits isolated singular cells or sheets of neoplastic cells permeated with granular cytoplasm, uniform, spherical nuclei and evenly distributed, fine nuclear chromatin [2, 3]. Grossly, a well circumscribed, solid tumefaction enunciating yellow, tan or brown hue may be discerned. Tumour magnitude varies from 0.5 centimetres to 11 centimetres. Teratomatous component may delineate cystic alterations or focal calcification. Infrequently, extra- testicular tumour progression or incrimination of spermatic cord may ensue [3, 4]. Upon microscopy, tumefaction exhibits cellular nests, glands with intra-luminal mucin or solid sheets. Besides, an insular, acinar or trabecular pattern of tumour evolution may be encountered. An admixture of diverse neoplastic configurations may ensue [3, 4]. Neoplastic cells appear monomorphic and are pervaded with abundant, granular, eosinophilic to pale staining cytoplasm, regular spherical nuclei and fine or salt and pepper nuclear chromatin. Circumscribing stroma is delicate, fibrous or hyalinised [3, 4]. Testicular neuroendocrine tumour appears non concurrent with germ cell neoplasia in situ. Mitotic figures, focal necrosis and vascular invasion may be infrequently exemplified [3, 4]. Atypical neuroendocrine tumour is associated with focal necrosis, nuclear atypia and mitotic activity with > 2 mitoses per 10 high power fields (HPF) [3, 4]. Ultrastructural examination exhibits pleomorphic to regular, spherical or elliptical intracytoplasmic neurosecretory granules in Figures 1 & 2 [5, 6].
TNM Staging of Carcinoma Testis
Primary Tumour
TX: Primary tumour cannot be assessed Tis: Germ cell neoplasia in situ (GCNIS) T0: No evidence of primary tumour within the testis T1: Primary tumour confined to testis and rete testis. Vascular or lymphatic infiltration is absent. Tunica albuginea is invaded. Tumour invasion into tunica vaginalis is absent. Pure seminoma is subdivided as
- T1a: Tumour magnitude < 3 centimetres
- T1b: Tumour magnitude ≥ 3 centimetres T2: Tumour confined to testis, rete testis and extends into ≥ one components of testis as blood vessels, lymphatics, epididymis, adipose tissue confined to hilar soft tissue adjacent to epididymis or tunica vaginalis T3: Tumour extends into spermatic cord T4: Tumour extends into scrotum. Regional lymph nodes Clinical staging of regional lymph nodes is assessed with imaging techniques as computerized tomography (cN).
Pathological staging of regional lymph nodes is assessed with dissection of regional, retroperitoneal, para-aortic, peri-aortic, inter-aortocaval, paracaval, pre-aortic, precaval, retro-aortic and retrocaval lymph nodes (pN).
- NX Regional lymph nodes cannot be assessed
- N0 Regional lymph node metastasis absent
- N1 Regional lymph node metastasis confined to one to five retroperitoneal lymph nodes with magnitude < 2 centimetres
- N2 Regional lymph node metastasis into minimally a singular enlarged lymph node or lymph node mass >2 centimetre and <5 centimetre diameter OR metastasis into >5 regional lymph nodes <5 centimetre diameter OR metastasis into minimally a singular lymph node between 2 centimetre and 5 centimetre diameter
- N3 Regional lymph node metastasis into minimally a singular enlarged retroperitoneal lymph node or lymph node mass > 5 centimetre magnitude OR metastasis into minimally a singular enlarged lymph node or lymph node mass > 5 centimetre diameter
Distant Metastasis
MX: Distant metastasis cannot be assessed M0: Distant metastasis into distant lymph nodes or various organs absent M1: Distant metastasis into
- M1a: Metastasis into pulmonary parenchyma or distant lymph nodes as pelvic, thoracic, supraclavicular or visceral lymph nodes apart from retroperitoneal lymph nodes
- M1b: Distant metastasis into viscera as hepatic parenchyma, skeletal system or brain. Pulmonary parenchyma may or may not be incriminated.
Serum Tumour Markers
SX: Serum tumour marker levels unavailable S0: Serum tumour marker levels appear normal S1: Minimally a singular tumour marker level exceeds normal range as
- lactic dehydrogenase (LDH) <1.5 times upper normal limit (ULN)
- βHCG < 5,000 mIu/mL
- alpha fetoprotein (AFP) <1,000 ng/mL S2: Minimally a singular tumour marker appears substantially above normal range as
- lactic dehydrogenase (LDH) between 1.5 times to 10 times upper normal limit (ULN)
- βHCG between 5,000 to 50,000 mIu/mL
- alpha fetoprotein(AFP) between 1,000 to 10,000 ng/mL S3: Minimally ≥ one or more tumour markers are significantly elevated
- lactic dehydrogenase (LDH) > 10 times upper normal limit(ULN)
- βHCG > 50,000 mIu/mL
- alpha fetoprotein (AFP)> 10,000 ng/mL Testicular neuroendocrine tumour appears immune reactive to cytokeratin, synaptophysin, chromogranin A or CD56. Immune markers as substance P, gastrin, vasoactive intestinal polypeptide (VIP) or neurofilaments are infrequently expounded. Tumour cells appear immune nonreactive to OCT 3/4, CD30, KIT, thyroid transcription factor 1(TTF-1), SF1, SOX2, alpha inhibin or CDX2 [7, 8].
Testicular neuroendocrine tumour requires segregation from neoplasms as Sertoli cell tumour, granulosa cell tumour or neuroendocrine tumour metastatic into testis. Testicular neuroendocrine tumour may be appropriately discerned with cogent histological assessment of surgical resection specimens [7, 8].
Testicular neuroendocrine tumour may suitably be subjected to surgical manoeuvers as orchiectomy. Lesions associated with distant metastasis may benefit with retroperitoneal lymph node dissection. Alternatively, receptor targeted radiotherapy may be employed. Notwithstanding, adoption of chemotherapy or radiotherapy may be associated with minimal therapeutic benefits. Primary testicular neuroendocrine tumour concordant with testicular teratoma demonstrates superior prognostic outcomes, in contrast to singular, pure testicular neuroendocrine tumour. Factors contributing to emergence of distant metastasis appear as atypical morphology, enlarged tumour magnitude > 7 centimetres, elevated mitotic activity or occurrence of carcinoid syndrome [7, 8]. Conclusion Testicular neuroendocrine tumour appears immune reactive to cytokeratin, synaptophysin, chromogranin A or CD56 and infrequently to substance P, gastrin, vasoactive intestinal polypeptide (VIP) or neurofilaments. Tumour cells appear immune non-reactive to OCT 3/4, CD30, KIT, thyroid transcription factor 1(TTF-1), SF1, SOX2, alpha inhibin or CDX2.
Testicular neuroendocrine tumour requires segregation from neoplasms as Sertoli cell tumour, granulosa cell tumour or neuroendocrine tumour metastatic into testis. Neoplasm is appropriately discerned with cogent histological assessment of surgical resection specimens. Testicular neuroendocrine tumour may suitably be managed with surgical manoeuvers as orchiectomy.
References
-
Albalawi AA, Bedaiwi AK, Alotaibi MA, Bedaiwi K (2023) Testicular Neuroendocrine Tumors: A Case Report and Literature Review. Cureus 15(4): e37370.
-
Şahin ÖF, Fenercioğlu ÖE, Beyhan E, Çermik TF, Ergül N (2023) Testicular Metastasis of Jejunal Neuroendocrine Tumor on 68Ga-DOTATATE PET/CT. Mol Imaging Radionucl Ther 32(2): 156-158.
-
Gaddam SJ, Chesnut GT (2023) Testicle Cancer. Stat Pearls International. 2023; Treasure Island, Florida.
-
Torghabeh AE, Dolati M, Gharib M, Saghafi H, Saghafi M (2023) Primary Carcinoid or Sex Cord-Stromal Tumor of the Testis: A Case Report. Caspian J Intern Med 14(1): 147-149.
-
Image 1 Courtesy: Pathology outlines.
-
Image 2 Courtesy: Research gate.
-
Meyts ER, Aksglaede L, Bandak M, Toppari J, Jørgensen N (2000) Testicular Cancer: Pathogenesis, Diagnosis and Management with Focus on Endocrine Aspects. In: Feingold KR, Anawalt B, Blackman MR (EDS.), Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.
-
Amine MM, Mohamed B, Mourad H, Majed H, Slim C, et al. (2017) Neuroendocrine Testicular Tumors: A Systematic Review and Meta-Analysis. Curr Urol 10(1): 15-25.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury