Moral Judgment and Inferential Reasoning in Patients with Bipolar Disorder and Schizophrenia
Introduction: Previous studies demonstrated that both emotional and cognitive processes are involved in moral judgments. In this study we analyse moral judgment in two psychiatric pathologies to explain the greater use of the utilitarian judgment in moral dilemma, to recognize a selective sense moral disorder or a consequence of Theory of Mind impairment. Methods: We investigated the characteristics of moral judgment in patients with bipolar disorder and schizophrenia using personal dilemma (“Footbridge” Dilemma) and impersonal dilemma (“Trolley” Dilemma). Our study included 19 bipolar patients, 18 schizophrenic patients, and 21 healthy controls. Subjects were instructed to determine whether or not each dilemma was morally acceptable. Results: All subjects performed two Theory of Mind (ToM) tasks: the Eyes Test for emotional components and the Fauxpas Test for cognitive components.Bipolar patients performed lower than controls on all ToM tasks and on two moral dilemmas. Patients with schizophrenia performed lower than controls on all ToM tasks and on the personal moral dilemma. Conclusions: Ourresults provide evidence that inferential reasoning and moral judgments (personal and impersonal) are two different cognitive abilities and in psychiatric people their impairments can coexist and they can be linked when emotional processing is involved.
Introduction
Specific cognitive processes are involved in moral evaluations on others social actions. In traditional moral psychology models, moral judgment is considered as a product of conscious reasoning [1]. Recently, social intuitionist models proposed an important role of emotion in moral judgment and suggested that reasoning follows the emotion reactions [2, 3]. Greene at al. proposed a dual process model of moral judgment, in which two separate psychological processes influence moral judgment: emotional and cognitive aspects are involved in two different processes depending on the type of moral dilemma [4, 5]. In the “trolley” dilemma, a malfunctioning trolley is killing five people. If it is switched to a side track; it will sacrifice just one person. In the “footbridge dilemma, the way to save the five people is by pushing a man off the “footbridge” and down onto the track. For most of people sacrifice one person to save five persons is morally acceptable in the “trolley” dilemma, but not in the “footbridge” dilemma, because the action of pushing a person active emotional processing. For this the “trolley” and “footbridge” dilemmas are considered impersonal and personal moral dilemmas. In a pilot study with fMRI, Greene and colleagues 2001 showed that ventromedial prefrontal lobe and superior temporal sulcus are active in personal moral decision making, whereas the dorsolateral prefrontal cortex and inferior parietal lobe are active in impersonal dilemmas. They suggested that two separate psychological processes (cognition and emotion) influence moral judgment. From the view of utilitarian judgment, it is better the five people survive instead that one, but most people feel strong aversion or disgust when they choose utilitarian judgment because they do not feel that the consequences justify the action [6, 7].
In other researches on social cognition, patients with VMPC lesions exhibit reduced social emotions [8, 9, 10] and defect in emotional regulations [11] but they endorse moral violations in personal dilemmas [12]. These results suggest that some psychiatric patients with impaired Theory of Mind, social emotion or emotional regulations may have different performance on moral judgment. In addition, a study investigated moral judgment in maniac and euthymic patients with bipolar disorder, using moral dilemma task [13]. From results, bipolar patients experiencing manic disorders with impaired emotional regulation and behavioural control, showed a significantly greater utilitarian judgment for personal dilemma. In our opinion it is not clear if these results derived by a specific impairment of moral sense or if it is caused by a Theory of Mind (ToM) impairment, considering some studies one motional and cognitive components of ToMin psychiatric patients [14, 15].
Recently, some researchers found that differential performance on the Moral Judgment Interview by people with schizophrenia and healthy controls was mediated via social-cognitive ability, as theory of mind [16]. A more recent study extends these results, providing no evidence that moral judgment is compromised in schizophrenia [17]. From this data patients with schizophrenia were less influenced by automatic aversive responses to amoral conduct and that association found between poorer perspective-taking and greater disapproval of social transgressions suggests insensitivity to others’ extenuating motives may worse social misunderstandings in schizophrenia.
We think that investigate ToM impairments in two psychiatric pathologies with different moral behaviours and beliefs, we could explain the greater use of the utilitarian judgment in moral dilemma, recognizing a selective sense moral disorder or a consequence of ToM deficit that makes impossible attributing emotions or mental states to others. In this study we investigate: 1) Moral judgment of psychiatric patients in personal and impersonal dilemmas; 2) Cognitive and emotional components of ToM in patients with bipolar disorder and schizophrenia.
Materials and Methods
Participants
Thirty seven psychiatric patients were recruited at Psychiatric Department of University Hospital in Catania (Italy). Inclusion criteria were the following: age between 18 and 65 years old; diagnosis of bipolar disorder type I or schizophrenia according to DSM-IV TR criteria (American Psychiatric Association, 2000) using Structured Clinical Interview for DSM-IV (SCID) First, et al. stable medication intake during the preceding month (as confirmed by the clinical staff and/or a family member).
All patients were in a stable phase of the disorder and able to live in the community with a stable medication regimen provided by the outpatient facilities of the University Mental Health Centre of Catania. All schizophrenia patients (N=18) were on stable antipsychotic drug treatments (risperidone 5, clozapine 4, olanzapine 5, and aripiprazole 4), 3 patients a combination of typical and atypical antipsychotic drugs.
All bipolar patient (N=19) were examined after clinical stabilization. Remission criteria for bipolar disorder patients (euthymia) were defined as a rating of <=9 on the Hamilton Depression Rating Scale (HAM-D); <=9 on the Mania Rating Scale (YMRS); and a self-report by the patient and confirmation by at least one family member that the patient was in remission. All bipolar disorder patients were receiving psychiatric medication, mainly mood stabilizers (seven patients taking lithium, six patients sodium valproate and five patients taking carbamazepine).
Exclusion criteria were: history of substance abuse, history of mental retardation, neurological disease, or any clinical condition that could affect cognitive performance and other psychiatric disorder in comorbidity.
Additionally, twenty-one aged-matched healthy volunteers (HC) served as controls: they had no antecedence of neurological disease, neither history of psychotic or affective disorders in themselves or a first- degree family member, and they were not taking psychotropic medication.
All the subjects provided written informed consent after a complete description of the study, in accordance with the local Institutional Review Board.
Measures
Clinical Assessment
The Positive and Negative Syndrome Scale (PANSS) [18] and the Clinical Global Impressions Scale (CGI) [19], were applied to assess psychopathology in schizophrenic patients. The patient’s symptomatology was assessed with the Positive and Negative Symptoms of Schizophrenia (PANSS) [18]. The Clinical Global Impression-Severity (CGI-S) scale [19] was used to assess patient condition at baseline.
The Hamilton Depression Rating Scale (HDRS), [20] and Mania Rating Scale (YMRS) [21] were applied to assess psychopathology in bipolar patient. Additional clinical information was obtained from clinical charts and direct patients interview. Exposure to antidepressants, mood stabilizers, antipsychotics, and benzodiazepines was assessed. Cognitive Measures To assess logical reasoning and general intelligence we use Colored Progressive Matrices CPM, (Raven, 1984).
Theory of Mind Tasks
Second-order false belief task (cognitive components). Two second-order false belief stories (Pietro’s Birthday story and Ice-cream story, Sullivan, et al.) were presented to the patients. At the end of the story two test questions (second-order ignorance and second-order belief) were presented. Participants received one point for each correct answer (maximum total score for each story=2).
Theory of mind–perception: Eyes Test (emotional components). To test perceptual aspects of ToM competence we used an Italian adaptation of the Eyes Test which is based on the original English version devised by Baron-Cohen, et al. [22]. In order to perform well on this test participants, need to know a number of mental state terms, match them to the ocular region of a face and decide whether the terms describe adequately the face by choosing one adjective among four possible alternatives. Participants were presented 37 black and white photographs showing the ocular regions of male and female adults. On each trial, first a photograph was presented and the participants were asked a control questions about the gender of the person in the photo. Then, four adjectives describing complex emotions or other mental states (e.g. dispirited, bored, embarrassed, flirting) were shown below the picture and participants were asked to choose the word that best described the photograph. Participants were asked to read all four words before making their choice. Then experimenter asked: ‘Which word best describes what this person is feeling or thinking?’ Following the procedure used by Baron-Cohen, et al. participants were encouraged to consult a glossary of all words used in the task whenever they felt they were not sure about their meaning. The maximum score on test and control questions was 36. Two Moral Dilemmas for Moral Judgment Two different and well known moral dilemmas were presented to the participants. In the “Trolley” Dilemma the experimenter tells: “You are standing near train tracks and you see a runaway train carriage (a trolley) heading towards five people – if it hits them it will kill them instantly. You can save those five people by pulling a lever on the tracks next to you that will divert the carriage from the track it’s currently on (heading towards the five people) onto another track. However, there is one person standing on the other track and they will be killed if you pull the lever”. After story he asks: “Is it appropriate to save the five people by pulling the lever and killing one person?” In the “Footbridge” Dilemma the experimenter tells: “You are standing on a footbridge that is going over the train tracks and something similar to the scenario above is happening – a trolley is heading towards five people. You can push someone off the footbridge where you’re standing to hit the carriage and the trolley will stop, saving the five people’s lives but killing the person you pushed.” After story he asks: “Is it appropriate to save the five people by pushing the one person to their death?”
Results
Clinical Cognitive and demographical characteristics of bipolar patients, schizophrenic patient and healthy controls are shown in Table 1. The statistical analyses were conducted with SPSS 19.0.
Schizophrenic
Bipolar
Healthy Controls
patient patient (n=18) (n=19) (n=21) Male 16 5 13 Age 33,83 (10,96) 47,47 (11,03) 37, 24 (14,11) Education 11,89 (3,23) 10,05 (4,17) 12,14 (3,30) Onset of illness 21,50 (4,11) 28,89 (8,04) -- QoL 6,17 (2,00) 7,37 (2,19) -- CGI 3,56 (0,78) 3,32 (0,75) -- PANSS 74,56 (20,74) -- -- HDRS -- 8.05 (6,19) -- MRS -- 5,00 (5,88) -- Raven CPM 29,11 (7,29) 22,63 (7,45) 33,76(1,94) (Values are expressed as mean; standard deviation is
shown in brackets. QOL= QL-Index; CGI= Clinical Global
Impression, PANSS=.Positive and Negative Syndrome
$$ \text{Impression, PANSS} = \text{Positive and Negative Syndrome Scale, HDRS} = \text{Hamilton Depression Rating Scale, MRS} $$
MRS=Mania Rating Scale)
Table1: Clinical and demographical characteristics of
schizophrenic, bipolar patients and healthy controls (HC).
ANOVA analysis founded a significant effect of group factor on Raven (PCM), in which the mean scores of patients with schizophrenia was significantly lower than those of the other two groups (p’s=.01). ANOVA analysis also revealed a significant effect of group factor on all ToM tasks and on two moral dilemmas. Multiple comparison tests were conducted using Bonferroni correction. Results indicated that on Eyes Test the mean scores of patients with schizophrenia and bipolar disorder were significantly lower than those of controls, all p's = .000).
On Second Order False Belief Task, in each story (Pietro’s Birthday story and Ice-cream story)the mean scores of patients with schizophrenia and with bipolar disorder were significantly lower than those of controls (all p’s = .000). On impersonal moral dilemma (“Trolley” Dilemma) the mean scores of patients with bipolar disorder was significantly lower (all p’s = .01) than those of controls. On personal moral dilemma (“Footbridge” Dilemma) the mean scores of patients with schizophrenia was significantly lower (all ps = .000) than those of controls.
Comparing the performance of two clinical groups separately, no significant difference was found on all ToM tasks and on two moral dilemmas. Different patterns of results were founded comparing the performances of each clinical group with those of control group.
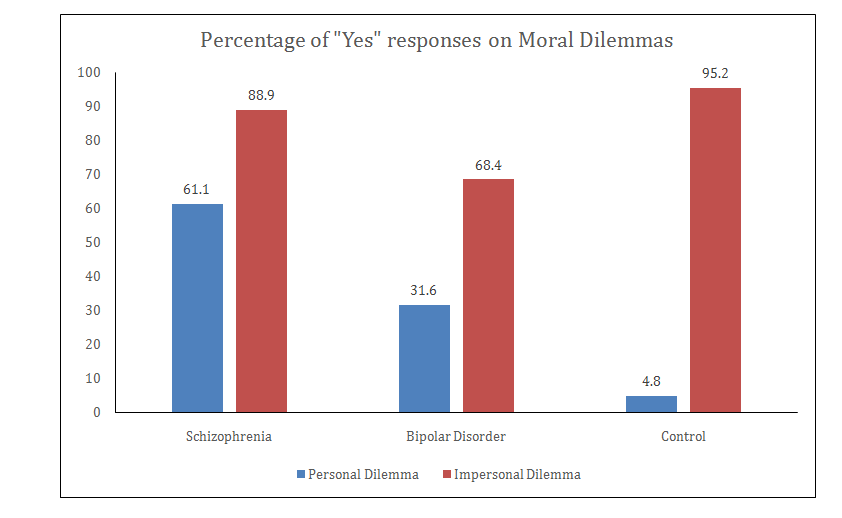
The mean scores of patients with schizophrenia was lower than that of controls on Eyes Test (t (37) = - 7.79, p= .000, equal variance not assumed, and on Second Order False Belief Tasks, Pietro’s Birthday story (t (37) = - 4.44, p = .000) and Ice-cream story (t (37) = - 5.89, p = .000) equal variance assumed in both stories. Nonparametric statistics were used to analyze dichotomic results on moral dilemmas. Schizophrenic patients were more likely to choose “yes” for the proposed action in personal moral dilemma, “Footbridge” Dilemma than controls (p = .000, Fischer exact test). No significant difference was found for impersonal dilemma (p=.20, Fischer exact test). These findings indicate that schizophrenic patients’ response only differed for personal moral dilemma.
The mean scores of patients with bipolar disorder was lower than that of controls on Eyes Test (t (38) = 4.76, p=.001, equal variance assumed, and on Second Order False Belief Tasks, Pietro’s Birthday story (t (38) = - 4.66, p = .000) and Ice-cream story (t (38) = - 6.77, p = .000) equal variance assumed in both stories. Nonparametric statistics were used to analyze dichotomic results on moral dilemmas. Bipolar patients were more likely to choose “yes” than controls for the proposed action in personal moral dilemma, “Footbridge” Dilemma (p =.04) and in impersonal dilemma, “Trolley” Dilemma (p= .007, Fischer exact test).
The between-group differences in endorsement of the proposed action (i.e. “yes” response) for impersonal moral and personal moral dilemmas are show in graphic (see Figure 1).
We also investigated the correlations between CPM Raven, 1984, ToM task and two moral dilemmas in two clinical groups. Patients with schizophrenia exhibited a positive correlation between CPM and Pietro’s Birthday story (Second Order False Belief Task, second order ignorance, r = .528; p=. 02. There was no significant correlation between ToM tasks and the two moral dilemmas. In patients with bipolar disorder there were significant correlations between CPM and Eyes Test (r = .677; p = .001), CPM and Ice-cream story (Second Order False Belief Task, second order belief) (r = .657; p = . 002).
Discussion
In the current study patients with schizophrenia performed lower than controls on CPM (logical reasoning), on all ToM tasks (emotional and cognitive components) and on the personal moral dilemma (“Footbridge” Dilemma). These results suggest: a) a general cognitive impairment of ToM, including emotional and cognitive components; b) a more utilitarian judgment in emotionally salient personal moral dilemma. Taken together, our results provide evidence that inferential reasoning and moral judgment are not linked to the general intelligence (logical reasoning). However, the fact that we only founded a significantly correlation between CPM and Pietro’s Birthday story (Second Order False Belief Task, second order ignorance) cannot attribute to general intelligence all ToM deficits [23]. In our results, there is no correlation between the mean scores of all ToM tasks (emotional and cognitive components) and also there is no correlation between ToM performance and moral dilemmas results (personal and impersonal dilemmas). This data suggests different underlying neurobiological mechanisms. For emotionally salient personal moral dilemma (“Footbridge” Dilemma) schizophrenic patients were more acceptable of moral violations than normal controls. More utilitarian judgment in personal dilemma may be due to the ToM impairment and the altered processing of emotional or cognitive information [9, 10, 14, 15]. According to the Greene’s dual- process view, conflict between utilitarian and deontological judgments happen when patients consider personal moral dilemma [24]. In some recent studies the understanding of moral judgment has focused on the integrated role of cognition and emotion rather than their mutually competing roles [25, 26]. Their conclusions suggested that increased utilitarian judgment of personal dilemmas observed in schizophrenic patients might reflect disrupted synchronization between the prefrontal cortex and subcortical structures, including amygdala. Electrophysiological and imaging studies will be needed to identify the neural mechanisms related to unique moral judgment in psychiatric patients.
Our results extend a recent previous study on patients with bipolar disorder Kim, et al. 2015, in which maniac patients showed significantly greater utilitarian judgment than euthymic patients and normal controls for personal moral dilemmas. In our study, bipolar patients performed than controls on CPM (logical reasoning), on all ToM tasks (emotional and cognitive components) [27] and on two moral dilemmas (“Footbridge” Dilemma and “Trolley” Dilemma). Our patients with bipolar disorder were all selected in euthymic clinical state to exclude maniacal symptoms. We found a significant correlation between Ice-cream story (Second Order False Belief Task, second order belief) and personal moral dilemma (“Footbridge” Dilemma), showing that the greater utilitarian judgment in moral personal dilemma could be associated to impaired understanding of consequences of moral violations or a limited inferential reasoning. On ToM impairments, we found also significant some correlations between CPM and Eyes Test, (emotive components), CPM and Ice-cream story (Second Order False Belief Task, second order belief) (cognitive components). This data suggest that in bipolar patients ToM impairments could be attributing to general intelligence, differently from results that we found on schizophrenic patients. In conclusion, our results in moral judgment assessments may reflect the different underling neurobiological mechanism when more emotional processing is activated in moral personal decision making. Taken together, these conclusions provide evidence that inferential reasoning and moral judgments (personal and impersonal) are two different cognitive abilities and in psychiatric people their impairments can coexist and also they can be linked when emotional processing is involved.
In considering the clinical implications, our results token together promote cognitive behavioural approaches in psychiatric patients to stimulate a better cognitive and emotional control during moral judgments.
This study has several limitations. Our results should be carefully interpreted because of the relatively small sample size and single site recruitment.
References
-
Kohlberg L (1981) The philosophy of moral development moral stages and the idea of justice. Digital Georgetown: 441.
-
Haidt J (2001) The emotional dog and its rational tail: a social intuitionist approach to moral judgment. Psychol Rev 108(4): 814-834.
-
Damasio A (2005) The neurobiological grounding of human values. Neurobiology of human values: 47-56.
-
Greene JD (2007) Why are VMPFC patients more utilitarian? A dual-process theory of moral judgment explains. Trends in Cogn Sci 11(8): 322-323.
-
Greene JD, Sommerville RB, Nystrom LE, Darley JM, Cohen JD (2001) An fMRI investigation of emotional engagement in moral judgment. Science 293(5537): 2105-2108.
-
Chapman HA, Kim DA, Susskind JM, Anderson AK (2009) In bad taste: Evidence for the oral origins of moral disgust. Science 323(5918): 1222-1226.
-
Schnall S, Benton J, Harvey S (2008) With a clean conscience: Cleanliness reduces the severity of moral judgments. Psychological Science 19(12): 1219-1222.
-
Damasio AR, Tranel D, Damasio H (1990) Individuals with sociopathic behavior caused by frontal damage fail to respond autonomically to social stimuli. Behav Brain Res 41(2): 81-94.
-
Frith CD, Frith U (1999) Interacting minds--a biological basis. Science 286(5445): 1692-1695.
-
Geraci A, Surian L, Ferraro M, Cantagallo A (2010) Theory of Mind in patients with ventromedial or dorsolateral prefrontal lesions following traumatic brain injury. Brain Injury 24(7-8): 978-987.
-
Anderson SW, Barrash J, Bechara A, Tranel D (2006) Impairments of emotion and real-world complex behavior following childhood-or adult-onset damage to ventromedial prefrontal cortex. J Int Neuropsychol Soc 12(2): 224-235.
-
Koenigs M, Young L, Adolphs R, Tranel D, Cushman F, et al. (2007) Damage to the prefrontal cortex increases utilitarian moral judgements. Nature 446(7138): 908-911.
-
Kim SH, Kim TY, Ryu V, Ha RY, Lee SJ, et al. (2015) Manic patients exhibit more utilitarian moral judgments in comparison with euthymic bipolar and healthy persons. Compr Psychiatry 58: 37-44.
-
Geraci A, Cantagallo A (2011) Inferential reasoning: Comparison of patients with schizophrenia and patients with traumatic brain injury. Psychiatry Res 188(2): 291-293.
-
Shamay-Tsoory SG, Aharon-Peretz J (2007) Dissociable prefrontal networks for cognitive and affective theory of mind: A lesion study. Neuropsychologia 45(13): 3054-3067.
-
McGuire J, Barbanel L, Brüne M, Langdon R (2015) Re-examining Kohlberg's conception of morality in schizophrenia. Cogn Neuropsychiatry 20(5): 377-381.
-
McGuire J, Brüne M, Langdon R (2017) Judgment of moral and social transgression in schizophrenia. Compr Psychiatry 76: 160-168.
-
Kay SR, Fiszbein A, Opler LA (1987) The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull 13(2): 261-276.
-
Guy W (1976) Clinical Global Impressions. In: ECDEU Assessment Manual for Psychopharmacology, DHEW publication, no. (ADM) 76-338.
-
Hamilton M (1960) A rating scale for depression. J Neurol Neurosurg Psychiatry 23(1): 56-62.
-
Young RC, Biggs JT, Ziegler VE, Meyer DA (1978) A Rating scale for mania: reliability, validity and sensitivity. The British Journal of Psychiatry 133(5): 429-435.
-
Baron-Cohen S, O'riordan M, Stone V, Jones R, Plaisted K (1999) Recognition of faux pas by normally developing children and children with Asperger syndrome or high-functioning autism. J Autism Dev Disord 29(5): 407-418.
-
Brüne M (2003) Theory of mind and the role of IQ in chronic disorganized schizophrenia. Schizophr Res 60(1): 57-64.
-
Greene JD (2015) The rise of moral cognition. Cognition 135: 39-42.
-
Moll J, de Oliveira-Souza R (2007) Moral judgments, emotions and the utilitarian brain. Trends in Cognitive Sciences 11(8): 319-321.
-
Shenhav A, Greene JD (2014) Integrative moral judgment: dissociating the roles of the amygdala and ventromedial prefrontal cortex. J Neurosci 34(13): 4741-4749.
-
Kalbe E, Schlegel M, Sack AT, Nowak DA, Dafotakis M, et al. (2010) Dissociating cognitive from affective theory of mind: a TMS study. Cortex 46(6): 769-780.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury