Neurology then and Now Letter
I review the changes in the teaching and practice of neurology as they occurred over two generations of neurologists assuming a generation to be approximately 30 years. I illustrate the highlights and mention some of the leading figures who have contributed to altitude medicine and clinical neurology as it is taught and practiced today.
The Change in Vocabulary
In 2003 the completion of the Human Genome project led to the introduction of a new vocabulary into clinical neurology. This became imperative to accommodate terms such as “whole genome sequencing”, “microanalysis” RNAi and “kariotyping”. Rare neurological diseases ceased to remain clinical curiosities without hope of treatment and some became preventable such as phenylketonuria [1].
Grand Round
The obligatory practice of selecting a suitable patient to be presented at Grand Rounds has been abandoned in favor of audio-visual presentations usually eschewing actual patients. The nearest to the previous style was a Grand round given by Dr. Phillip Pearl “a Neuroscience Talk and Piano Performance”. Dr. Pearl is Director of Epilepsy and Clinical Neurophysiology at Boston Children's Hospital. He played the piano to illustrate the points about epilepsy in children. Patient interviews at grand rounds have been abandoned because of ethical considerations.
Raymond D. Adams, MD (1911–2008) [2] the founder of the Massachusetts General Hospital’s clinical neurology program was an advocate of Grand Rounds in the classical style (Figure 1).
Letter to Editor
Internet Service
The ability of neurologists to access Internet Service is usually thought to begin around 2006. This changed dramatically the learning ability of clinical neurologists and their training. No longer was it necessary to spend hours in libraries but a short look at a cell phone is usually sufficient to find answers to difficult problems.
Rounds instead of starting at the bedside began in the office with a review of the problem rather than at the bedside with clinical examination of the patient. This was a radical change that required changes in teaching, record keeping and style of clinical activities in the hospital.
Traditionally, the journeyman years were a time of travel after completing apprenticeship. This tradition dates back to medieval times and continued for neurologists today. It was imperative to spend time at the National Hospital for Nervous Diseases in London now National Hospital for Neurology and Neurosurgery (NHNN), Queen Square, where Consultant Neurologists, that is unpaid neurologists such as Macdonald Critchley, Charles Symonds and Arnold Carmichael did morning ward rounds (Figure 2).
In 1957 Peter Kynaston Thomas (PK) (Figure 3) became senior registrar in neurology at the National hospital, Queen Square. He was in that position in 1961 when his duties included the procurement of patients for demonstrating at Grand Rounds. Macdonald Critchley told PK to bring a patient with amyotrophic lateral sclerosis (ALS) to the lecture theater. Unfortunately for PK there was no such patient at that time in the hospital. PK thought that he would bring a patient with the Landry Guillen-Barre syndrome instead and tell Macdonald about this switch before he began his demonstration, but Critchley would not listen, no matter how hard PK tried. Critchley was known for his showmanship and some considered him a better actor than neurologist. This then resulted in a superb demonstration of the clinical signs of ALS on a patient who did not have the disease.
Peter’s love for travel lead him and Anita, his second wife, to the then highest road in the world at Khardung La (5600 m) pass at the Indian-Tibetan border. We met by chance in Chisumle a village below the pass. Subsequently we collaborated on the investigation of Neurological manifestations of chronic mountain sickness (CMS), the burning feet-burning hands syndrome, in Cerro de Pasco, Peru [3]. We demonstrated, for the first time, the reduced basal laminal thickness in the sural nerves of patients with CMS (Figure 4). This was unexpected but not surprising. We considered this not part of a neuropathic process but rather representing an adaptive phenomenon to life at high altitude and for CMS patients the result of severe hypoxia [3].
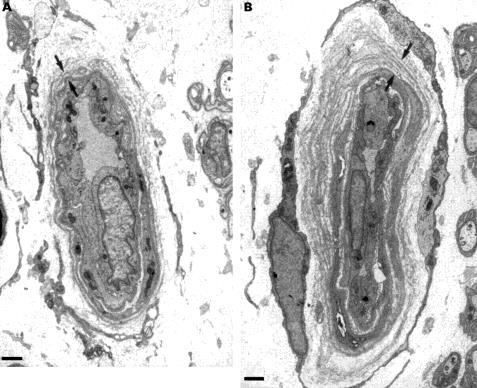
The mean thickness of the basal laminal zone was less in the three patients with CMS (1.13 (0.04) μm than in the control subjects, (1.67 (0.11) μm) [3].
In Boston, meanwhile, the journey man tradition in neurology continued at the Massachusetts General Hospital and Boston City Hospital (Derek Ernest Denny- Brown, 1901-1981) who was a New Zealand-born neurologist working in Oxford, London and Boston, who made major contributions to neurology, such as the development of electromyography, the physiology of micturition, the treatment of Wilson's disease he epitomized the journeyman style of training for a career in clinical neurology.
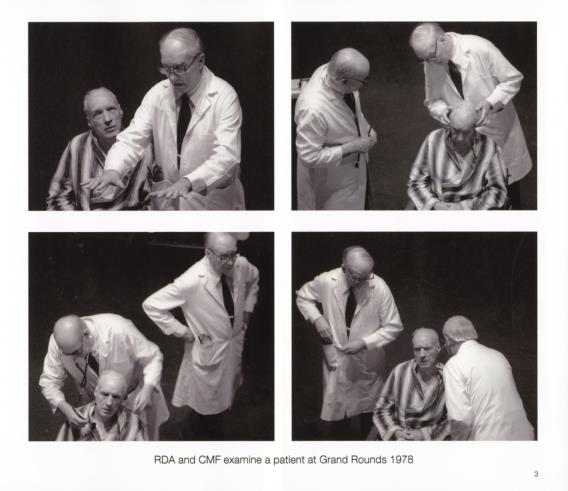

The newly established department of neurology at the University of New Mexico (Figure 7) attracted faculty from far afield including the Massachusetts General Hospital and it soon acquired the nick name “the Harvard on the Mesa”. Neurology was taught as it was while Raymond D. Adams and C Miller Fisher where in charge at MGH (Figure 5).

Finally this era came to an end in 1990 with the beginning of neurology as it is now practiced using largely computerized patient care.
References
-
Scriver CR (1994) Science, medicine and phenylketonuria. Acta Paediatr 407: 11-18.
-
Walter J Koroshetz (2009) Raymond D. Adams, MD (1911–2008). Neurology 72(6): 488-489.
-
Thomas PK1, King RH, Feng SF, Muddle JR, Workman JM (2000) Neurological manifestations in chronic mountain sickness: the burning feet-burning hands syndrome. J Neurol Neurosurg Psychiatry 69: 447- 452.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury