The Impact of Age on the Health Locus of Control in Different Cultural Contexts during the Covid-19 Pandemic
The current study analyzes the impact of age life cycles on the Health Locus of Control construct in different cultural contexts during the Covid-19 pandemic. The purpose is to examine whether different age categories impact the health behavior of individuals and change the Internal Health Locus of Control (IHLC), Powerful Others Health Locus of Control (PHLC), and Chance Health Locus of Control (CHLC) during the outbreak in Asia and Europe of the Covid-19 pandemic. A total of 2617 respondents aged 18–80 from Asia and Europe completed an online version of the Multidimensional Health Locus of Control Scale – Form A. To examine the impact of age on the Health locus of control construct, the study participants were divided into three age groups: up to 35, from 36 to 50, and over 50. Data analysis reveals that along with the influence of cultural context on the Health locus of control construct, age periods also impact and change IHLC, PHLC, and CHLC levels. Respondents from Asia, under the age of 35 and in mature adulthood, have a strong tendency to rely on themselves (IHLC) in the regulation of their health behavior. Europeans, compared to Asians, have consistently lower IHLC levels throughout the life cycle. Results also yield differences in relation to PHLC: Europeans, compared to Asians, are less likely to trust powerful others at an early age, while in adulthood, the health control by powerful others increases dramatically. Data analysis also shows that young Asians tend to rely on chance, fate, or luck (CHLC), however, this tendency is not observed among young Europeans. The opposite trend is observed with age: while in Asian culture levels of CHLC decrease with age, in European contexts, these levels increase.
Introduction
Humanity entered a new paradigm of existence in 2020. This new paradigm, tentatively referred to as the Covid-19 pandemic, is marked by a global change in all areas of social life. A theoretical study published in 2014 analyzed the global crises humanity would face in the future, such as economic, migration, ecological crises and others, and it predicted the outbreak of a global health crisis, like the current pandemic [1]. At that time nobody imagined that this crisis would cause damage not only to human health but would also result in profound changes in the economy, politics, interstate relations, tourism, communication among people, and way of life. These cardinal changes, taking place before our eyes, gave us a reason to propose that in 2020 the world, as a whole, has entered a new paradigm of existence.
The Covid-19 pandemic has affected not only the physical health status of people, but the crisis situation proved also to be a significant factor in causing great damage to the mental health of people [2, 3, 4, 5]. The pandemic has had a particularly strong impact on adolescents, as they have been forced to start online education, break off contacts with their classmates and teachers, and stay in isolation at their homes. Our research team, formed of scientists coming from various universities and research centers in Asia, Europe, and the United States, understood the seriousness of the pandemic and foresaw the damage it would do to societies. This understanding was the reason for this psychological research to start immediately after the outbreak of the Covid pandemic. The scientific goal of the study was to “capture” the initial picture of the critical pandemic situation and to examine the way in which age life cycles affect the Health Locus of Control construct in different cultural contexts. This cross-cultural research was carried out at the very beginning of the pandemic outbreak – in the period from April to June 2020. The connection between the health locus of control and age periods in conditions of a pandemic will be discussed in the following sections.
Health Locus of Control Construct – Brief Clarifications
The term locus of control refers to attributing the causes of people’s behavior to external or internal factors. It was introduced by Julian Rotter in 1954, who proposed two types of locus of control: “internal” -the belief that the people can control outcomes in their own life, and “external” – the belief that life outcomes are controlled by powerful others, like authoritarian figures or fate, over which the individual has no influence [6]. Numerous studies demonstrated that the internality-externality dimension is playing an important role in the regulation of individual health behavior [7, 8, 9, 10, 11, 12, 13, 14]. In short, this dimension determines why some people believe they can control the outcomes in their own lives, whereas others believe that the control of events happens separately from and outside themselves.
The Health Locus of Control construct mediates perceptions of health-related behavior and determines the extent to which the individuals are prone to think that their real health behavior depends on themselves, on powerful others, or on external factors like chance and fate. Based on this theoretical assumption, scales have been created, which are used to measure the locus of control in relation to individual health expectations [15, 16, 17, 18, 19, 20, 21, 22]. As a result, the Multidimensional Health Locus of Control (MHLC) scale was developed, consisting of three major dimensions [18], as follows: Internal Health Locus of Control (IHLC), Powerful Others Health Locus of Control (PHLC), and Chance Health Locus of Control (CHLC). The first mentioned scale (IHLC) refers to the individuals’ belief that their health depends on their own behavior. The second scale (PHLC) refers to the belief that individual health is dependent upon the behaviors of powerful others (medical doctors). The third dimension (CHLC) was based on the belief that luck or chance factors determine health outcomes.
There are a number of research studies that support the important functions of the Health Locus of control construct in the regulation of individual health behavior [23, 24, 25, 26, 27, 28]. These studies, however, have been conducted in normal health conditions and provide information about the functions of this personality construct in a standard health situation. The aim of the current study is to examine the changes that occur in the health locus of control as a function of age and culture in a critical pandemic situation.
Age, Cultural Context, and Health Locus of Control
Health is a fundamental issue in all societies and is the key to well-being and happiness. Successful approaches to health care must be based on accurate cross-cultural understandings of what might be termed universal and of what is culture-bound. The very conceptions of health have been altered in response to advances in social science. Health is a positive state of well-being, rooted in the concept of quality of life and not just of the absence of disease [29]. A study examined the health locus of control among Native Americans. The research included 3665 participants aged 15 to 93 years. The main objective was to observe demographic correlates of health beliefs, as measured by the multidimensional locus of control scale. The results on gender differences showed women had a higher score on the Chance locus of control dimension than men. Age positively correlated with lower IHLC and higher PHLC. In turn, the level of education was associated with lower CHLC. The life experiences of Native Americans are likely responsible for these findings and contribute to the relationship of health beliefs to healthy behaviors [30].
In a large-scale study of 2388 men and 2454 women aged 40-79, the relationship of the HLC to socio-demographic variables such as smoking and drinking was examined. The study was completed in a rural community in Japan. Results showed that elderly subjects, women, and participants with fewer years of education showed more external health beliefs. Participants who participated in adverse health behavior, such as smoking and excess drinking, also showed more external health beliefs [31].
The Health Locus of Control construct has been used in tracing successful aging. A study compared patients with cancer and the control group. Results showed that the IHLC contributes to a positive effect in cancer patients when they are sufficiently healthy to still exert control over their health [32]. The role of IHLC was also demonstrated by the study of A. Zhang, et al. [33]. The authors examined how the internal health locus of control is associated with older adults’ self- rated health. They reveal that the internal health locus of control was directly associated with positive health ratings and shed light on its important role in the psychological mechanism of health perception and health promotion.
Age has been seen as a factor in many studies [34]. Results show that HLC beliefs change with age, as developmental theories of health control striving will predict. However, scales to measure the health locus of control have been used to study not only adults but children, too. To understand children’s health behavior, it is important to assess the degree to which they believe their health to be the result of self-actions, the actions of “powerful” adults, or random events and fate. In this direction goes the study of E. Perrin, et al. [35]. Results of the study on HLC in healthy children and children with chronic physical illness show that younger, compared to older children, have a significantly stronger belief that the chance and powerful others control their health. Another large-scale study of 10,579 schoolchildren aged 11-16 examined the relationship between age, smoking behavior, and health locus of control beliefs. Smokers compared to non-smokers indicated less belief in powerful others (e.g. medical doctors) or in personal control, but they believe more in the importance of chance in determining health outcomes [36].
Most studies on HLC are focused on mature adults or the aged. A study on aged people from 69 to 100 living in a retirement community found that optimism correlated positively with IHLC [37]. Another age-related study explored the relationship between HLC expectancies and age attitudes on the process of aging. For example, the relationship between health locus of control, self-efficacy beliefs, and lifestyle behaviors was studied in a sample of 57 healthy elderly subjects, and as result, positive relationships were found among these variables. Data analysis shows, that most of the participants were characterized by an internal health locus of control belief (91.2%), high generalized self- efficacy (57.9%), and good health behaviors. The individuals, dominated by IHLC and high generalized self-efficacy, are more likely to benefit from a health education program than those with an external locus of control and low self-efficacy [38].
In another study, the impact of age on locus of control was studied as related to patients’ preferences for shared decision-making in general medical practices. The authors examined 234 patients in order to find out if there was a relationship between the health locus of control, preferred communication style, hospital anxiety, and depression. They found that age is a mediator on which communication style, health locus of control, and depression depend. With an increase in age, participation in personal decision-making as well as external and internal health locus of control decline, while the results of depression go up [38]. The correlation between age and the health locus of control is also proven by longitudinal studies. For example, in their four-year longitudinal study Bailis, et al. [34] revealed the correlation between age and the health locus of control beliefs. They examined changes in HLC among 124 members of a health- promotion facility aged between 22 and 81 and showed that HLC beliefs changed with age.
Research Purpose and Hypotheses
According to the existing cultural tradition, we take for granted that all personality phenomena have arisen in, and are influenced by, a certain cultural context. The research goal of the current study is to reveal that during the pandemic situation, the health locus of control of individuals living in different cultural contexts is also influenced by age. We assume that in different cultural contexts, age life cycles impact the health locus of control construct in different ways. In this case, it is important for us to check how this happens in a critical pandemic situation. In this regard, the following hypothesis has been formulated:
Hypothesis
During the Covid-19 pandemic, age stages influence differently on HLC in the Asian and European samples and change in different ways the levels of IHLC, PHLC, and CHLC.
Method & Participants
The participants in the study were representatives of European and Asian cultures. The total sample included 2617 subjects aged between 18 and 80 (M = 37.98, SD = 15.20), 1412 of which were drawn from Asia, (45.9% identified as female, 49.6% as male respondents, and 4.5% preferred not to answer), and 1205 were representatives of European samples (64.6% identified as female, 34.5% as male respondents, and 0.9% preferred not to answer). The average age of participants from Asia was 32 years (M = 31.50, SD = 12.77). The average age of participants from Europe was 45 years (M = 44.96, SD = 14.51).
The study included the following respondents: from Asia – China (N = 500), India (N = 500), Indonesia (N = 412); from Europe – Bulgaria (N = 405), Germany (N = 400), Hungary (N = 400).
Materials and Procedure
The study was conducted online from April to June 2020. The Research Ethics Approval Procedure was not applied in this study, as the survey was anonymous, and respondents completed the online questionnaire voluntarily. In addition, the questionnaire is an internationally recognized research instrument, published in a renowned scientific journal, and repeatedly used in research.
To examine the validity of the hypothesis, we employed the Multidimensional Health Locus of Control Scale – Form A. As mentioned above, this scale was developed based on Rotter’s concept of the external-internal locus of control, however, in this case, the scale examines the differences between the internal, chance, and powerful others’ health locus of control dimensions [18, 19]. Numerous studies on the health locus of control Schneider A, et al. [39, 40, 41, 42, 43, 44, 45, 46, 47, 48] have shown that the MHLC scales are moderately reliable (i.e. they have Cronbach alphas in the .60–.75 range and test-retest stability coefficients ranging from .60–.70). In the present sample, the MHLC reliability is moderate with Cronbach’s alpha from 67 and 77.
To test the validity of the hypothesis the subjects were divided into three age groups. The concept of Armstrong [49], on the twelve stages of the human life cycle, was used to distinguish the three age categories. The subjects were divided into three age groups, as follows: Early Adulthood – up to 35 years; Midlife – from 36 to 50; Mature Adulthood – over 50. It is believed that in the context of European and/ or Asian cultures, these three age groups will impact and contribute in different ways to changes in IHLC, PHLC, and CHLC levels.
To check the results for the aforementioned hypotheses, the following statistical methods were employed: descriptive statistics, paired-samples t-test, independent samples t-test, and two-way ANOVA analysis of variance.
Results
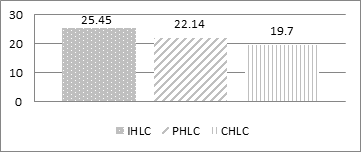
The assumption, formulated in the hypothesis, that the cultural context is a determinant of personality phenomena, is based on a number of empirical studies. This could be taken for granted if the study was conducted during a normal, rather than in an extreme, pandemic situation. The results show that in the extreme pandemic situation cultural differences also influence and change the health locus of control configuration (IHLC/PHLC/CHLC) in different ways. The results show that for the entire sample (N = 2581), the highest mean value was observed in IHLC (M = 25.45; SD = 5.54), followed by PHLC (M = 22.14, SD = 6.14), and CHLC (M = 19.70, SD = 5.82) was positioned in third place. The binary comparison of the mean values using the paired-samples t-test showed that statistically significant differences were obtained in the levels of the three variables (p< .001). These results for the total sample lend support to the more powerful effects of IHLC when compared to PHLC and CHLC (Figure 1).
Independent T-test samples were used to compare the means of the MHLC subscales for respondents from Europe and Asia. The results indicated that the scores were significantly higher on the IHLC subscale for respondents from Asia than for participants from Europe. The effect size is small and indicated that only 2% of the variance in the IHLC is explained by cultural differences. However, the scores were significantly higher on the subscale of PHLC for the respondents from Asia compared to respondents from Europe. In this case, the effect size was medium and indicated that 6% of the variance of PHLC has to be explained by cultural differences. A comprehensive analysis of the impact of cultural differences on the configuration of the Health Locus of control construct during a pandemic situation is presented by Krumov, et al. [50].
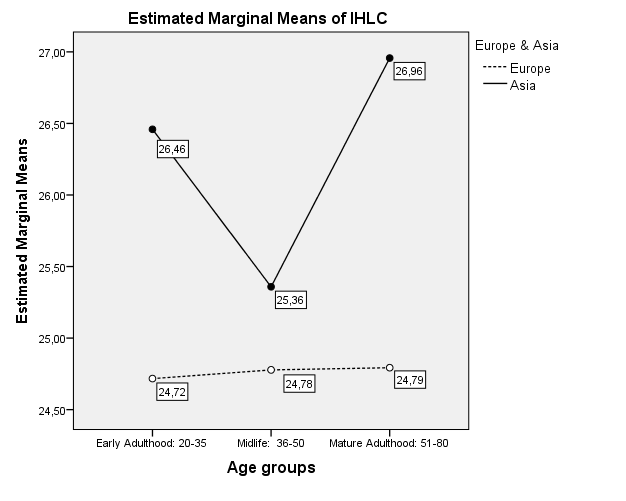
The main scientific subject of this study, however, is to prove that during an extreme pandemic situation, along with cultural contexts, age differences also influence the HLC, and contribute to significant changes in IHLC, PHLC, and CHLC levels. Results show that age differences influence the configuration of the Health Locus of control construct in the two samples, i.e., the separate stages of the human life cycle contribute in different ways to changes in relation to IHLC, PHLC, and CHLC levels. As pointed out above, for the purpose of the analysis the entire sample was divided into three age groups: Early Adulthood – up to 35 years; Midlife – from 36 to 50 years; Mature Adulthood – participants older than 50. It is proposed that in the context of European and/or Asian cultures, these three age groups will impact and contribute in different ways to changes in relation to IHLC, PHLC, and CHLC levels. A two-way ANOVA analysis of variance was performed to determine if there was a difference in IHLC by culture type and age group. As the data from the analysis show, there is a statistically significant effect of the interaction between the factors “type of culture” and “age group” – F(2,2447) = 3.22, p < .05, with a small effect size, η = .05.
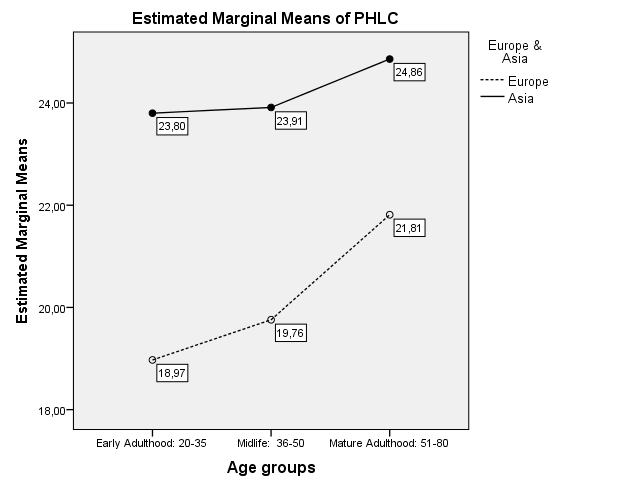
Figure 2 shows that the statistically significant two- factor differences are due to the first and especially to the third age group. However, while in Asians, IHLC is most pronounced in early and late adulthood, in Europeans, IHLC levels are consistently lower over the three life cycles.
Significant two-factor effects were also observed with respect to PHLC – F(2,2449) = 3.72, p < .05, with small effect size, η = .05. The trends are illustrated in Figure 3, which shows that cross-cultural differences in PHLC decrease with age.
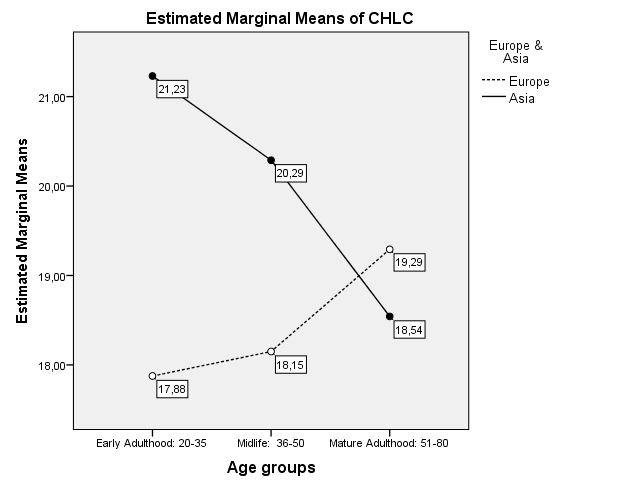
The two-factor effects on CHLC are most pronounced – F(2,2446) = 20.63, p < .001 in the magnitude of the effect η = .13. The results are visualized in Figure 4.
Results show that while in Asian cultures CHLC levels decrease with age, in European cultures the opposite trend is observed. Interestingly, the differences between the two groups are somewhat equalized in relation to respondents over 50 years.
Discussion
Results support the assumption that not only in a normal, but also in a pandemic situation, the differences in relation to IHLC, PHLC, and CHLC levels are due to variances between the characteristics of different cultural contexts (Figure 1). This finding is not surprising, as it is in line with the cultural tradition, according to which personal phenomena are influenced by the cultural context in which they arise [51, 29, 52, 53, 54, 55, 56, 57]. In addition, this is in line with findings of many cross-cultural studies, according to which different cultural contexts affect in different ways manifestations of personal and social phenomena [58, 59, 60, 61, 62, 63, 64, 65, 66, 67]. Moreover, data received from a study conducted by Krumov KD, et al. [50] during a pandemic situation suggest that cultural influences can be explained through the four dimensions formulated in Hofstede’s cultural theory: power distance (PDI), uncertainty avoidance (UAI), masculinity-femininity (MAS), and individualism-collectivism (IDV) [68, 69, 70, 71]. Since the cultural influence, according to the cultural paradigm, is taken for granted, as mentioned above, the main conclusion in the current study is that along with cultural context, age periods also influence the HLC configuration. In this case, it is assumed that in different cultural contexts, stages of the human life cycle (Early Adulthood, Midlife, and Mature Adulthood) affect HLC in different ways, and contribute to changes in relation to IHLC, PHLC, and CHLC levels. The influence of each age stage on HLC, during the Covid-19 pandemic situation, is mediated by the specific features of different Asian and European cultural contexts. The results show that when comparing the two samples (Europeans and Asians), each age group (Early Adulthood, Midlife, or Mature Adulthood) corresponds to different levels of IHLC, PHLC, and CHLC.
The results, illustrated in Figure 2, reveal that in each age group, the IHLC configurations are quite different in the two cultures. Respondents from Asia under the age of 35 have a strong tendency to rely on themselves to regulate their health behavior in the pandemic situation. This self-attribution to the health control decreases sharply among the individuals from the Midlife group, while among the representatives of Mature Adulthood, the tendency to self-attribute (to rely on oneself) rises sharply. Statistically significant two- factor differences between Europeans and Asians are due to the first and especially the third age group. Results are quite different in the European sample. It is clear that in a pandemic, Europeans’ age groups do not have a significant impact on their internal health locus of control attribution. This means that their attitudes toward controlling their own health behavior remain relatively unchanged throughout the life cycle. Moreover, Europeans have consistently lower IHLC levels over the three life cycles than Asians.
As for the attribution of health behavior control to the powerful others (PHLC), the trend is quite different (Figure 3). Both Asians and Europeans, with increasing age, tend to trust the powerful others (doctors, health institutions, government) to control their health behavior. In this respect, there are some differences between the two cultural groups. Europeans, compared to Asians, are less likely to trust powerful others at an early age, while in adulthood, their health control on the part of the powerful others increases dramatically.
Of particular interest is the picture that has been revealed in relation to CHLC. The results shown in Figure 4 reveal an opposite trend, characteristic of both cultures. While in a pandemic situation, in relation to their health, the young Asians tend to rely on chance, fate, or luck, such a tendency is not observed among the young Europeans. The opposite trend is observed with age: while in Asian culture, CHLC levels decrease with age, in the European context, these levels increase. Of further interest, the differences between the two cultural groups gradually disappear, and CHLC levels are almost equal in the oldest period.
Strengths, Weaknesses, and Future Research Goals
The most important strength of the study is the fact that it tested the Health locus of control construct at the beginning of the Covid-19 pandemic, which has never happened before and will never be repeated under the same conditions. Another positive feature of the research is the use of the measurement instrument MHLCS, which has established validity and reliability. The third positive feature of the study is the fact that the respondents belong to the three European and three Asian countries, i.e., are ad hoc typical representatives of Asian and European cultures. A weakness of the study is that it had to be conducted very quickly, and the use of representative (stratified) national samples for each country was not possible. That condition prevented a comparative analysis between the separate countries. As a result, the analysis was performed only between the total participants of the two cultural regions (The Asian and European). The future goal is to conduct the same research again but in the expected post-pandemic situation. This will enable us to reveal, through comparative analysis, the cultural influences on HLC in two different situations – pandemic and post-pandemic.
Conclusion
The survey shows that in the Covid-19 pandemic situation, most participants rely on IHLC and/or PHLC, whereas fewer rely upon their health being under the control of chance or luck (CHLC). These different levels of expression regarding IHLC, PHLC, and CHLC, however, are partly due to the different impacts of cultural contexts. The research illustrates that in the pandemic situation, along with cultural differences, age periods also influence the configuration of HLC. Respondents from Asia under 35 have a strong tendency to rely on themselves in regulating their health behavior during a pandemic situation. This tendency decreases sharply among respondents from the Midlife group, while among the representatives of Mature Adulthood, the tendency to rely on themselves rises sharply. In the European sample, this picture is quite different. Europeans’ age groups do not have a significant impact on their internal health locus of control during the pandemic. This means that their attitudes to personal control of their own health behavior remain unchanged throughout the life cycle.
With respect to PHLC, the research supports some differences between the two cultural groups. Europeans, compared to Asians, at an early age are less likely to trust powerful others, while in adulthood, health control on the part of the powerful others increases dramatically. In relation to CHLC, results show that young Asians tend to rely more on chance, fate, or luck, however, this tendency is not observed among young Europeans. With increasing age, the differences between the two groups gradually disappear, and the CHLC levels are almost equal in the oldest period.
Acknowledgments
The authors thank all anonymous survey participants who voluntarily completed the online questionnaire.
Funding This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Krumov K, Larsen K, Krumova A, Hristova P (2014) The crises of our times as a challenge to the sustainable development of modern civilization. Journal of innovation, entrepreneurship and sustainable development 1(2): 3-8.
-
Brailovskaia J, Teismann T, Friedrich S, Schneider S, Margraf J (2021) Suicide ideation during the COVID-19 outbreak in German university students: Comparison with pre-COVID 19 rates. Journal of Affective Disorders Reports 6: 100228.
-
Gelezelyte O, Dragan M, Grajewski P, Kvedaraite M, Lotzin A, et al. (2021) Factors associated with suicide ideation in Lithuania and Poland amid the COVID-19 pandemic. Crisis: The Journal of Crisis Intervention and Suicide Prevention. Advance online publication.
-
Javed B, Sarwer A, Erik B, Soto EB, Mashwani ZR (2020) The coronavirus (COVID-19) pandemic’s impact on mental health. The International Journal of Health Planning and Management 35(5): 993-996.
-
Shoib S, Saleem A, Javed S, Das S, Pinto da Costa M (2022) Suicide in Trans Individuals During the COVID-19 Pandemic. Indian Journal of Psychological Medicine 44(1): 66-69.
-
Rotter JB (1966) Generalized expectancies for internal versus external control of reinforcement. Psychological Monographs: General and Applied 80(1): 1-28.
-
April K, Dharani B, Peters, K (2012) Impact of Locus of Control Expectancy on Level of Well-Being. Review of European Studies 4(2): 124-136.
-
Benassi VA, Sweeney PD, Dufour CL (1988) Is there a relation between locus of control orientation and depression? Journal of Abnormal Psychology 97(3): 357-367.
-
Blanchard E, Scarboro M (1973) Locus of control and the prediction of voting behavior in college students. Journal of Social Psychology 89(1): 123–129.
-
Deutchman IE (1985) Internal-External Locus of Control, power and political participation. Psychological Reports 57(3): 835-843.
-
Judge TA, Erez A, Bono JE, Thoresen CJ (2002) Are measures of self-esteem, neuroticism, locus of control, and generalized self-efficacy indicators of a common core construct? Journal of Personality and Social Psychology 83(3): 693-710.
-
Lefcourt HM, Dyal JA (1984) Cross-cultural research with the locus of control construct. New York: Academic Press, Inc.
-
Roddenberry A, Renk K (2010) Locus of Control and Self-Efficacy: Potential Mediators of Stress, Illness, and Utilization of Health Services in College Students. Child Psychiatry & Human Development 41(4): 353-370.
-
Salmani Nodoushan MA (2012) The impact of locus of control on language achievement. International Journal of Language Studies 6(2): 123-136.
-
Ferraro LA, Price JH, Desmond SM, Roberts SM (1987) Development of a Diabetes Locus of Control Scale. Psychological Reports 61(3): 763-770.
-
Lewis KS, Jennings AM, Ward JD, Bradley C (1990) Health belief scales developed specifically for people with tablet-treated type 2 diabetes. Diabetic Medicine: A journal of the British Diabetic Association 7(2): 148- 155.
-
Saltzer EB (1982) The Weight Locus of Control (WLOC) scale: A specific measure for obesity research. Journal of Personality Assessment 46(6): 620-628.
-
Wallston KA, Wallston BS, DeVellis RF (1978) Development of Multidimensional Health Locus of Control (MHLC) Scale. Health Education Monographs 6(2): 160-170.
-
Wallston BS, Wallston KA, Kaplan GD, Maides SA (1976) Development and validation of the Health Locus of Control (HLC) Scale. Journal of Consulting and Clinical Psychology 44(4): 580-585.
-
Wallston KA, Wallston BS (1982) Who is responsible for your health: The construct of health locus of control. In: Sanders G, Suls J (Eds.), Social Psychology of Health and Illness. Hillsdale, N.J.: Lawrence Erlbaum & Associates. pp. 65-95.
-
Whitman L, Desmond SM, Price JH (1987) Development of a Depression Locus of Control Scale. Psychological Reports 60(2): 583-589.
-
Wood WD, Letak JK (1982) A mental-health locus of control scale. Personality and Individual Differences 3(1): 84-87.
-
Brincks AM, Feaster DJ, Burns MJ, Mitrani VB (2010) The influence of health locus of control on the patient- provider relationship. Psychology, health & medicine 15(6): 720-728.
-
Burker EJ, Evon DM, Galanko J, Egan T (2005) Health locus of control predicts survival after lung transplant. Journal of Health Psychology 10(5): 695-704.
-
Jacobs-Lawson JM, Waddell EL, Webb AK (2011) Predictors of Health Locus of Control in Older Adults. Current Psychology 30(2): 173-183.
-
Johansson B, Grant JD, Plomin R, Pedersen NL, Ahern F, et al. (2001) Health locus of control in late life: A study of genetic and environmental influences in twins aged 80 years and older. Health Psychology 20(1): 33-40.
-
Knott CL, Clark EM, Kreuter MW, Rubio DM (2003) Spiritual health locus of control and breast cancer beliefs among urban African American women. Health Psychology 22(3): 294-299.
-
Norman P, Bennett P, Smith C, Murphy S (1998) Health locus of control and health behaviour. Journal of Health Psychology 3(2): 171-180.
-
Krumov K, Larsen K (2013) Cross-cultural psychology: why culture matters. IAP - Information Age Publishing, PO Box 79049, Charlotte, NC 28271, USA, ISBN: 9781623963163.
-
Egan JT, Leonardson G, Best LG, Welty T, Calhoun D, et al. (2009) Multidimensional health locus of control in American Indians: The strong heart study. Ethnicity & Disease 19(3): 338-344.
-
Kuwahara A, Nishino Y, Ohkubo T, Tsuji I, Hisamichi S, et al. (2004) Reliability and validity of multidimensional health locus of control scale in Japan: Relationship of demographic factors and health-related behaviors. The Tohoku Journal of Experimental Medicine 203(1): 37-45.
-
Knappe S, Pinquart M (2009) Tracing criteria of successful aging? Health locus of control and well-being in older patients with internal diseases. Psychology, Health & Medicine 14(2): 201-212.
-
Zhang A, Jang Y (2017) The Role of Internal Health Locus of Control in Relation to Self-Rated Health in Older Adults. Journal of Gerontological Social Work 60(1): 68- 78.
-
Bailis DS, Segall A, Chipperfield JG (2010) Age, Relative Autonomy and Change in Health Locus of Control Beliefs: A Longitudinal Study of Members of a Health-promotion Facility. Journal of Health Psychology 15(3): 326-338.
-
Perrin EC, Shapiro E (1985) Health locus of control beliefs of healthy children, children with a chronic physical illness, and their mothers. The Journal of Pediatric 107(4): 627-633.
-
Eiser JR, Eiser C, Gammage P, Morgan M (1989) Health Locus of Control and Health Beliefs in Relation to Adolescent Smoking. British Journal of Addiction 84(9): 1059-1065.
-
Guarnera S, Williams RL (1987) Optimism and locus of control for health and affiliation among elderly adults. Journal of Gerontology 42(6): 594-595.
-
Waller KV, Bates RC (1992) Health locus of control and self-efficacy beliefs in a healthy elderly sample. American Journal of Health Promotion 6(4): 302-309.
-
Schneider A, Korner T, Mehring M, Wensing M, Elwyn G, et al. (2006) Impact of health locus of control and psychological co-morbidity on patients’ preferences for shared decision making in general practice. Patient Education and Counseling 61(2): 292-298.
-
Kassianos AP, Symeou M, Ioannou M (2016) The health locus of control concept: Factorial structure, psychometric properties and form equivalence of the Multidimensional Health Locus of Control scales. Health Psychology Open 3(2): 1-10.
-
Cooper D, Fraboni M (1990) Psychometric study of Forms A and B of the multidimensional health locus of control scale. Psychological Reports 66(3): 859-864.
-
Athale N, Aldridge A, Malcarne VL, Nakaji M, Samady W, et al. (2010) Validity of the multidimensional health locus of control scales in American sign language. Journal of Health Psychology 15(7): 1064-1074.
-
De Las Cuevas C, Peñate W, Betancort, Cabrera C (2015) What do psychiatric patients believe regarding where control over their illness lies? Validation of the multidimensional health locus of control scale in psychiatric outpatient care. The Journal of Nervous and Mental Disease 203(2): 81-86.
-
Gutkin TB, Robbins JR, Andrews L (1985) The health locus of control scale: Psychometric properties. Educational and Psychological Measurement 45(2): 407-409.
-
O’Looney BA, Barrett PT (1983) A psychometric investigation of the Multidimensional Health Locus of Control questionnaire. British Journal of Clinical Psychology 22(3): 217-218.
-
Ross TP, Ross LT, Short SD, Cataldo S (2015) The multidimensional health locus of control scale: Psychometric properties and form equivalence. Psychological Reports 116(3): 889-913.
-
Luszczynska A, Schwarzer R (2005) Multidimensional Health Locus of Control: Comments on the Construct and its Measurement. Journal of Health Psychology 10(5): 633-642.
-
Wallston KA (2005) The Validity of the Multidimensional Health Locus of Control Scales. Journal of Health Psychology 10(4): 623-631.
-
Armstrong T (2019) The Human Odyssey: Navigating the Twelve Stages of Life. Ixia Press.
-
Krumov KD, Larsen KS, Liu J, Schneider JF, Krumova AK, et al. (2022) Health locus of control in a pandemic situation: cross-cultural differences between European and Asian respondents. Health Psychology Report 10(3): 227-237.
-
Berry JW, Poortinga YH, Breugelmans SM, Chasiotis A, Sam DL (2011) Cross-cultural psychology: Research and applications. Cambridge University Press.
-
Leung K, Bond MH (2004) Social axioms: A model for social beliefs in multicultural perspective. Advances in Experimental Social Psychology 36: 119-197.
-
Matsumoto D, Yoo SH (2006) Toward a new generation of cross-cultural research. Perspectives in Psychological Science 1: 234-250.
-
Minkov M (2012) Cross-cultural analysis: The science and art of comparing the world’s modern societies and their cultures. Los Angeles, CA: Sage.
-
Sam DL, Berry JW (2017) Cross-Cultural Psychology (Critical Concepts in Psychology), In: 1st (Edn,), Routledge, Taylor & Francis Ltd, London, UK.
-
Saucier G, Kenner J, Iurino K, Malham PB, Chen Z, et al. (2015) Cross-cultural differences in a global “survey of world views”. Journal of Cross-Cultural Psychology 46(1): 53-70.
-
Schwartz SH (2004) Mapping and interpreting cultural differences around the world. In: Vinken H, Soeters, J, et al. (Eds.), Comparing cultures: Dimensions of culture in a comparative perspective. Leiden, The Netherlands: Brill, pp: 43-73.
-
Berry JW (1969) On cross-cultural comparability. International journal of Psychology 4(2): 119-128.
-
Ember CR, Ember M (1998) Cross-Cultural Research. In: Bernard HR (Ed.), Handbook of Methodology in Cultural Anthropology. Walnut Creek, CA: Altamira Press, pp: 647-668.
-
Inglehart R (1997) Modernization and Postmodernization: Cultural, Economic and Political Change in 43 Societies. Princeton, Princeton University Press.
-
Kemmelmeier M, Burnstein E, Krumov K, Genkova P, Kanagawa C, et al. (2003) Individualism, collectivism and authoritarianism in seven societies. Journal of Cross- Cultural Psychology 34(3): 304–322.
-
Markus H, Kitayama S (1991) Culture and self: Implications for cognition, emotion and motivation. Psychological Review 98(2): 224-253.
-
Matsumoto D (1989) Cultural influences on the perception of emotion. Journal of Cross-Cultural Psychology 20: 92-105.
-
Triandis HC (1995) New directions in social psychology: Individualism and collectivism. Boulder, CO: Westview Press.
-
Segall MH, Dasen PR, Berry, JW, Poortinga YH (1990/1999) Human Behavior in Global Perspective: An Introduction to Cross-Cultural Psychology. In: 1st & 2nd (Edn.), New York, USA, Pergamon.
-
Witkin HA, Berry JW (1975) Psychological differentiation in cross-cultural perspective. Journal of Cross-Cultural Psychology 6(1): 4–87.
-
Hofstede G (1991) Cultures and Organizations: Software of the Mind. London, UK: McGraw-Hill.
-
Hofstede G (2001) Culture’s consequences: Comparing values, Behaviors, Institutions and Organizations across Nations. In: 2nd (Edn.), Thousand Oaks, CA: Sage Publications.
-
Hofstede G (2006) What did GLOBE really measure? Researchers’ minds versus respondents’ minds. Journal of International Business Studies 37: 882-896.
-
Hofstede G, McCrae RR (2004) Culture and personality revisited: Linking traits and dimensions of culture. Cross-Cultural Research 38(1): 52-88.
-
Hofstede G, Neuijen B, Ohayv DD, Sanders G (1990) Measuring organizational cultures: A qualitative and quantitative study across twenty cases. Administrative Science Quarterly 35(2): 286-316.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury