How the will Mediates Brain Functions: A Look at Dyslexia (and Dyscalculia)
To a malfunctioning of parts of the brain, medical science is inclined to seeking out physical (neural) causes. Hypotheses as regards probable causes are made known and all these are within the ambience of the physical (empirical) attestation, after all every effect has to be proportionate to its cause. This means that if there is a physical effect, then it has to arise from a physical cause. We can tweak that line to say that no immaterial cause can produce a material effect. This is because it goes against the cause and effect principle. It is in this line of thought that many brain scientists are quick to dismiss any cause that is not as neurally material as its effect. But from experience we are certain of the fact that sometimes the effect is not sufficiently explained by the cause that is being proffered. This is what is seen as regards the brain and its functioning on a consciously evident scale. The cause sometimes is not robust enough to account for the effect. When this happens, what becomes of the integrity of medical science? Departing from the aforesaid question, we pose another question: is the Will explainable by trends found in medical science? The answer to that is already evident, as medical science is empirical (materially verifiable), and the will is not materially evident. In this research, we want to assert that the will is powerful enough to cause certain effects and changes in the functioning of the brain, as will be seen in the actions expressed in and by the human person. To make concrete the hypothesis proposed by this research, consideration is given to the cases of Dyslexia (and dyscalculia).
What is the Human Will: A Philosophical Analysis
We ought to note above all else that willing or the use of the human will is the essential reserve of the human person. Therefore, asserting or regarding the will as the human will might appear tautological. Nonetheless for the sake of emphasis, we insist on regarding it as the human will. Aristotle in his Nicomachean Ethics, differentiates between a voluntary and an involuntary act [1]. He considers the former as having the moving principle in the agent himself that is internalized to and in the agent. But in the latter, he sees the moving principle as that which is external to the agent. He notes: that which is done under compulsion or by reason of ignorance is involuntary, the voluntary would seem to be that of which the moving principle is in the agent himself, he being aware of the particular circumstances of the action (c.340 BCE).
It is involuntary, if the individual has been drawn to act by something that is not in him, but outside him. Therefore, when one is compelled to carry out an act, the moving principle is the one or the thing that is compelling him to act, and not the actor himself. In other words, there is a spatial distinction between the cause of the action and the action itself. Hall RH [2] outlines this Aristotelian stance notes that something is involuntary if (a) it is either an action or a passion, and (b) it takes place either under compulsion or owing to ignorance. Something is voluntary if (a) it is either an action or a passion, and (b) it takes place neither under compulsion nor owing to ignorance.
He will eventually arrive at a refined position regarding the aforementioned Aristotelian stance when he says that something is involuntary if (a) it is either an action or a passion, and (b) the person who does the action or feels the passion is not in control of the action or passion. Something is voluntary if (a) it is either an action or a passion, and (b) the person who does the action or feels the passion, is in control of the action or passion [2].
The difference therefore between that which is voluntary and involuntary is seen in how control-laden the action or passion is. We would still insist upon the Aristotelian stance which says that the difference lies in the position of the moving principle, be it within or without. This implies that the will itself is a moving principle. Let it be said, that Aristotle does not use the term will, however, later considerations of the term, Will, have linked it synonymously to that which is voluntary (volitionally). To this, we can say that the moving principle is the will.
Thomas Aquinas on his own part, conceives of the will as inherently having the principle of motion, as he states that “… it is indeed first of all evident that the will moves it very self” [3]. Aquinas gives a detailed rendition of what the will does in the human person. On his line of thought, we ought to assert that the will is always moved towards the good. This good, can be either subjective or absolute. However, that which the will essentially tends towards as its end is the absolute good. It is because the will has the capacity to incline itself towards the good that can be subjective (selfishly oriented), that we have individuals engaging in acts against the law. Nonetheless, the full richness of this intellectual appetite, is found in the Sunum Bonum. The movement of the will is internally orchestrated, but it is triggered from an external source.
Human beings by using their intellect in the process of discovery move themselves to knowledge, as they move from things actually known to unknown things that were only potentially known. Just so, they by actually willing something move themselves actually to will something else. For example, human beings, by willing health, move themselves to will to take medicine, since they because they will health, begin to deliberate about things that conduce to health and finally will to take medicine when deliberation has so determined. Therefore, deliberation, which indeed results from the will of one willing to deliberate, precedes the will to take medicine. Therefore, since the will moves itself by deliberation, and deliberation is an inquiry that does not yield only one conclusion but leads to contrary conclusions, the will does not move itself necessarily. And since the will has not always willed to deliberate, something else needs to move the will to will to deliberate. And if the will indeed moves itself to deliberate, it is also necessary that deliberation precede the movement of the will, and that an act of the will precede the deliberation. And since there cannot be an infinite regression, we need to hold that regarding the first movement of the will, something external, at whose instigation the will would begin to will, moves the will of anyone not always actually willing [3].
This does in every way indicate that the movement of the will is very much dependent on the interaction that occurs between the human person and the environment in which he or she belongs. It should be reiterated that the principle of movement is that of the will, it is found within the human person. The deliberation that occurs initially before the finality of choice by the will is arrived at, is done by the intellect. It is therefore seen that the choice carried out by the will according to Aquinas, is one that is intellectual in nature, fitting the essence of the human person. However, when the good that is in consideration is not in dispute, the will inclines towards it without deliberation. As Aquinas notes it “Since such an object contains nothing repulsive, the will is naturally and wholly attracted to it” [4]. It is therefore brazenly clear that the will can move in and of itself and can also be moved by the intellect (all internally, which does not negate the fact that such movement starts from without).
Scotus J D does not seem to align himself with the above thought of Aquinas, as he notes that the faculty of the will contains in it the power of necessary movement, not contingent on any other thing except itself. He would however assert that it is only God that had the power to move the will. That is to say that it is God and the will itself, that has the power to move the will, even though he will note that the will can either be aligned naturally or deliberately, he insists that the will has a free power of volition that is intrinsically (essentially) its own [5]. Hobbes T [6], is of the opinion that deliberation is principally an act that must precede the will before it moves.
He notes in deliberation, the last appetite, or aversion, immediately adhering to the action, or to the omission thereof, is that we call the will; the act, not the faculty, of willing. And beasts that have deliberation, must necessarily also have will. The definition of the will, given commonly by the Schools, that it is a rational appetite, is not good. For if it were, then could there be no voluntary act against reason. For a voluntary act is that, which proceedeth from the will, and no other. But if instead of a rational appetite, we shall say an appetite resulting from a precedent deliberation, then the definition is the same that I have given here. Will therefore is the last appetite in deliberating. And though we say in common discourse, a man had a will once to do a thing, that nevertheless he forbore to do; yet that is properly but an inclination, which makes no action voluntary; because the action depends not of it, but of the last inclination, or appetite. For if the intervenient appetites, make any action voluntary; then by the same reason all intervenient aversions, should make the same action involuntary; and so one and the same action, should be both voluntary and involuntary. By this it is manifest, that not only actions that have their beginning from Covetousness, Ambition, Lust, or other Appetites to the thing propounded; but also those that have their beginning from Aversion, or Fear of those consequences that follow the omission, are Voluntary Actions.
Hume D [7], reechoes the above statement of Hobbes as he states that the power to act or not to, is fittingly the reserve of the will. He asserts but to proceed in this reconciling project with regard to the question of liberty and necessity; …it will not require many words to prove, that all mankind have ever agreed in the doctrine of liberty as well as in that of necessity, and that the whole dispute, in this respect also, has been hitherto merely verbal. For what is meant by liberty, when applied to voluntary actions? We cannot surely mean that actions have so little connection with motives, inclinations, and circumstances, that one does not follow with a certain degree of uniformity from the other, and that one affords no inference by which we can conclude the existence of the other. For these are plain and acknowledged matters of fact. By liberty, then, we can only mean a power of acting or not acting, according to the determinations of the will; that is, if we choose to remain at rest, we may; if we choose to move, we also may. Now this hypothetical liberty is universally allowed to belong to everyone who is not a prisoner and in chains. Here, then, is no subject of dispute.
Locke J [8] considering the concept of the will notes I find the will often confounded with several of the affections. Especially desire and one put for the other. This, I imagine, has been no small occasion of obscurity and mistake in this matter and therefore is, as much as may be, to be avoided. For he that shall then his thoughts inward upon what passes in his mind when he wills, shall see that the will or power of volition is conversant about nothing but that particular determination of the mind whereby, barely by a thought, the mind endeavors to give rise, continuation, or stop to any action which it takes to be in its power. This, well considered, plainly distinguished from desire, which may have quite a contrary tendency from that which our will sets us upon. A man whom I cannot deny may oblige me to use persuasions to another, which, at the same time I am speaking, I may wish may not prevail with him. In this case, it is plain the will and desire run counter. I will the action that tends one way, while my desire tends another, and that the direct contrary.
Locke considers the will to be solely a faculty of volition and nothing else. That is to say that the will has a power that is voluntary in nature. Even when it comes about that the will of another human has been compelled and forced into action, there is yet a show of the voluntary nature of the will, but this time of the one that is forcing the other. This is to say that the will of the other overrides the will of the one that is being compelled; which is to say that in any case the show of the will is witnessed.
Can we then refer to the human will as a faculty? Can it be referred to as a power? Can it be referred to as a physical entity or something metaphysical that has its homologue in the brain? What we can surmise about the will is that it is a power that has the capacity to and for volitional movement that is rational. That is to say that it can freely move itself, thereby moving the individual, the human person, who possesses it. It is an entirely metaphysical entity whose effect is felt in all that the human person does physically. The human will is itself intellectual faculty that is the principal agent in that which pertains to the making of choices either prior to or after sound deliberation. It is referred to as intellectual or rational, because its movement is always in line with what the rational human person has deemed to be good. In furtherance, we are asserting that the will, as espoused by Aquinas, targets that which is good, be it relative (subjective) or objective.
Analysis: Dyslexia
A Working Definition: Dyslexia is the difficulty in learning to decode (read aloud) and to spell [9]. The hypothesis offered is that dyslexia is occasioned by problems at the level of phonological representation [9, 10, 11]. This is based off the research done by Orton [12] and Bannatyne [13], who surmised that such condition is characterized by auditory sequencing, auditory discrimination and associating auditory symbols with sequences of visual symbols [9, 12, 13]. Dyslexia is construed as the low end of a normal distribution of word reading ability [14, 15]. It has been considered as a synonymous reality to the concept of reading disability [16, 17], and nothing more. However, it has received more consideration in other areas like poor decoding (we can refer to this as the second characterization of dyslexia), as Shaywitz, et al. [18], notes
Dyslexia is a specific learning disability that is neurobiological in origin. It is characterized by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary consequences may include problems in reading comprehension and reduced reading experience that can impede growth of vocabulary and background knowledge.
More to the above groupings that are linked to the generic name of dyslexia, there is a third group, or characterization that see readers who struggle to read, and yet do not fall under the purview of the dyslexic as detailed out in the above two. This group of persons is referred to as dyslexia with “persistent intractability to high quality intervention” [19].
As Elliot [19] puts it…we can only make such a determination post hoc (in reference to the persistent intractability to high quality intervention dyslexia, addition mine) on the basis of response to instruction over time, rather than on the basis of initial performance on a range of cognitive tests (as seen in the first and second characterization of dyslexia, addition mine).
What is being said here is that this particular group cannot be likened to the group that has reading disability or decoding impairment. This is because they have a certain difficulty in reading that is not to be compared to the aforementioned. Another grouping to this dyslexia phenomenon is that which is referred to as a pervasive neurodiverse disorder that goes beyond reading difficulties [20]. That is to say that one can be dyslexic even when one does not struggle with reading difficulties [21]. To this group, commonly known indicators include difficulties with memory (in reference to working memory), processing speed, attention, concentration, time management, self-organization and the capacity to express oneself orally [22, 23].
We can therefore outline the four classes that fall under the umbrella case of dyslexia to be:
- Reading disability
- Poor decoding skills
- Persistent intractability to high quality intervention
- Pervasive neurodiverse disorder that goes beyond reading difficulties.
Amidst the four outlined above, we are certain that the problem with dyslexia is more auditory that otherwise. Research carried out by the likes of Snowling and Griffiths, Vellutino et al., at different times have narrowed down the issue with the auditory system of the dyslexic to the one affecting the phonological structure of speech [24]. According to Snowling, problems with phonology lead to difficulty in learning mappings between orthography and phonology and other difficulties which include problems learning new spoken words, poor verbal short-term memory and problems with word retrieval and picture naming [25].
However, it would be too hasty to conclude that every phonologically related issue is dyslexia [26]. This is because there are occurrences of those children who have not an iota of reading difficulties that define dyslexia, but who have problems with phonological awareness [9, 27]. In addition to this, there are many individuals with dyslexic deficits that are not subsumed to the phonological domains [28, 29]. Therefore we can assert with Pennington [26] that “Dyslexia is the outcome of multiple risks which accumulate towards a threshold for what is usually termed ‘diagnosis’. We can identify some of these other risks as a. Deficit in semantic knowledge; this is because as regards the aforementioned, children with a low language show some weakness in learning to read words, especially if those words are difficult to decode [30]. b. Deficit in letter position coding (for instance slime and smile, mile and lime etc; Kohnen, et al. [31]. c. Differences in paired-associate learning or statistical learning [32]. d. Pre-school variations amongst 8-9 years old as regards oral language [33]. e. These four in addition to the phonological problem, will all be needed to really ascertain if the issue that one confronts is dyslexia or not.
Dyscalculia (Dyslexic Co-Occurrences)
Co-occurrences in this ambience can also be referred to as comorbidities. Comorbidity can be found between disorders within the same diagnostic grouping, for instance, reading disorder and mathematics disorder (both learning disorders with shared risk factors) as well as between disorders from different diagnostic groupings, such as between reading disorder and behavioral and emotional disorders [9, 34].
Comorbidity is the condition of having two or more diseases at the same time [35]. It could be that one of the diseases occasions the other, or provides the necessary environment for the other to thrive. With respect to this, and in the thought pattern of Moll et al., even if the comorbidity rate between a certain neurological deficit and another may vary considerably, on an average, “it can be asserted that about 40% of children with dyslexia will have another disorder accompanying the former” (2020). Therefore, we can list out comorbidities that align themselves with dyslexia, they include:
a. Developmental Language Disorder: characterized by persistent difficulties in expressive and/or receptive language [36, 37, 38, 39]. b. Attentional and Motor Coordination Problems [39, 40] c. Speech sound disorder [41] d. Socio-emotional and behavioral disorders [42] e. Anxiety and depression [43].
What should be considered is that these cannot be viewed as the core features of dyslexia, even though they add to it, making it more difficult to arrive at a validly strong prognosis of its occurrence, thereby making it difficult for a swift intervention [9, 44]. Another Comorbidity that I have chosen to itemize separately from the rest is Dyscalculia.
We can term dyscalculia as the dyslexia for all that is quantitative (mathematics). Much like reading disorder, dyscalculia is classified as a specific learning disorder in DSM5 [45]. It co-occurrence with dyslexia according to Snowling, Hulme and Nation is in between 30% and 70% of the cases [46, 47].
According to the British Dyslexia Association (BDA), Dyscalculia is a specific and persistent difficulty in understanding numbers which can lead to a diverse range of difficulties with mathematics. It will be unexpected in relation to age, level of education and experience and occurs across all ages and abilities. Mathematics difficulties are best thought of as a continuum, not a distinct category, and they have many causal factors. Dyscalculia falls at one end of the spectrum and will be distinguishable from other math
Assumable Prognosis
issues due to the severity of difficulties with number sense, including subitizing, symbolic and non-symbolic magnitude comparison, and ordering. It can occur singly but often co- occurs with other specific learning difficulties, mathematics anxiety and medical condition [48].
Dyscalculia is actually that compound term that represents a difficultly in math, ranging from the inability to apply math principles to solve problems to the inability to decipher the meaning of numbers; it is can also be known as the blindness of and to numbers otherwise known as acalculia, which is manifested in a distorted ability towards arithmetic [49]. The Symptoms of this includes:
- Difficulty working with numbers
- Being confused by math symbols
- Difficulty with basic facts (addition, subtraction, multiplication and division)
- A tendency to reverse or transpose numbers (eg 76:
We can itemize the types of dyscalculia to include: a. Verbal (interpretation of verbal math terms) b. Operational (performing basic arithmetic operations) Lexical (reading written math terms, symbols) c. Graphical (symbol manipulation) d. Ideognostic (mental calculations) e. Practognostic (pictorial representations) [49].
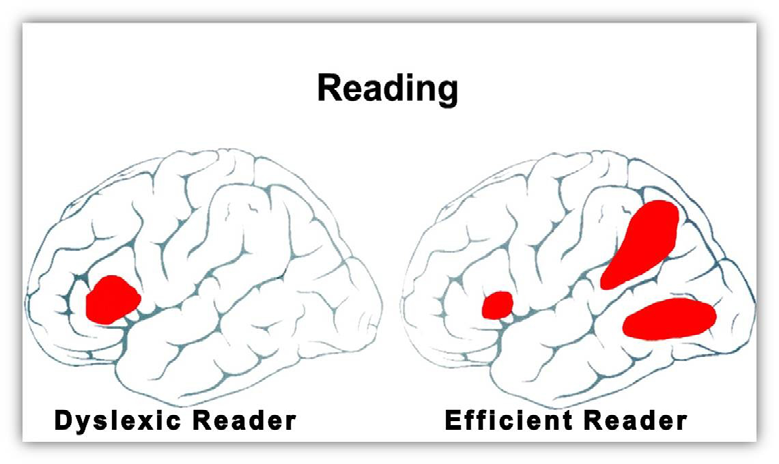
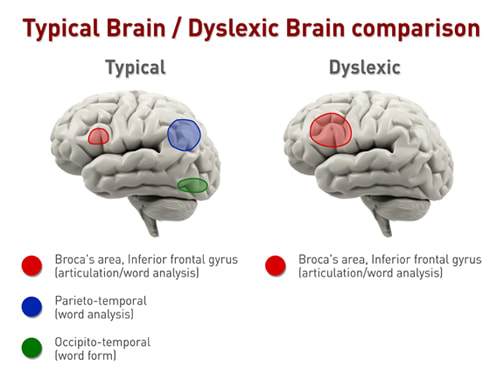
Figure 2: Credited to Marci Peterson: https://www.marcipetersonet.com/what-is-dyslexia.html From the above diagram Figure 1 we name the Dyslexic reader as A and the efficient reader as B. This prognosis is assumed because we do not certainly know yet what necessitates the composition of the brain of the one with dyslexia to differ from the one without it. It is very obvious that there is no difference in structure between A and B. However there are apparent areas that fire in the brain of B, which does not fire in A. To outline this area, a look is given to Figure 2. In this we can refer to the typical as 1 and the dyslexic as 2. In 1, there are three regions as much as B in figure 1 that comes alive when the brain of non-dyslexic is engaged in reading and understanding. They include the Broca Area, the Inferior gyrus, the parieto-temporal and occipito-temporal areas. It is of great value to notice that that of the Broca area (the inferior gyrus) is not as enlarged as it is in that of the dyslexic (as seen in 2 of figure 2). What this implies is that the dyslexic involves more effort in trying to level up with those that are his or her peers. This would prove to be near impossible because the other areas that are supposed to come alive when reading, comprehension and the likes are engaged in are dormant.
An analysis of the above diagram does not furnish us with the requisite prognosis as regards why some certain individuals suffer from dyslexia. Many assumable prognosis are of the opinion that this has to do with the genes that are responsible for the developmental formation of those areas of the brain. However, it is certainly valid to note that the brain of the dyslexic is structurally similar to that of a non- dyslexic, the difference only seen when it concerns the areas that come alive when reading and its attendant activities are called to play. There is a caveat to the above, this is because when using magnetic resonance imaging (MRI), slight differences in the brains of the dyslexic and non-dyslexic are noted.
According to Richards, et al. [50], a significant difference in fMRI connectivity occurred between children with dyslexia and normal reading controls in the left inferior frontal gyrus and its correlations with right and left middle frontal gyrus, right and left supplemental motor area, left precentral gyrus, and right superior frontal gyrus. There were no significant differences for the seed regions placed in the middle frontal gyrus, occipital gyrus or cerebellum. Children with dyslexia had greater functional connectivity from the left inferior frontal gyrus seed point to the right inferior frontal gyrus than did the children without dyslexia.
It should be said that “these structural and functional differences between dyslexics and good readers are often associated with phonological processing” (The capacity to grasp how words are made up of smaller units of sound, also referred to as phonemes, is called phonological processing) [51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61]. In order to give credence to what is being said here, functional connectivity tools were used.
According to Richards, et al. [50], Functional connectivity is a powerful noninvasive technique used to investigate the distribution of neural networks in participants who are normal controls and who have well characterized clinical disorders.
In a work carried out by Horwitz, et al. [54], they opined, after investigating the functional connectivity of the angular gyrus and its spatial connections during phonological processing, that there is a lack of coherence between measurements in the angular gyrus and parieto- temporal regions, (thereby, addition mine) suggesting functional disconnection between the brain regions involved in the phonological analysis process at the initial stages of phonological decoding.
However, in an fMRI study carried out by Pugh, et al. [56], functional disconnections were noticed between the angular gyrus and the parietal regions in the left hemisphere of the brain, and this region is known for its phonological processing. In another study by Shaywitz, et al. [60], they found out that Functional connectivity between the occipitotemporal region and inferior frontal gyrus in the left hemisphere was found to be present in controls under a real- word reading condition.
Berninger, et al. [50], reeling off the results from other research note that Poor readers, will exhibit functional connections between the left occipitotemporal region and right middle and inferior frontal gyri. The eventuality of all that is being said here is that there are three regions that fall short in reference to dyslexia, and they include left inferior frontal gyrus, right inferior frontal gyrus, and bilateral cerebellum [50, 51]. This is already clearly noticeable in the two figures above.
What we can surmise is the fact that there are aspects of the human reality that cannot be designed or constructed and to such reality; there is always a desire to understand all that pertains to it. In spite of how much we try to understand it, we still do not control how such human biological reality is designed or constructed. One certain reality that (which is being discussed now) is the brain. To this we can assert that no one has control over how his/her brain is going to look like or function. The brain of the dyslexic is microscopically structured differently but this does not in any make them less human than the non-dyslexic. What can be said with certainty is that the true cause of this issue (this is not an abnormality) is not yet certain. Therefore, till it is empirically attestedly certain, we say that it is still uncertain. In line with the aforementioned conclusion, Macchi W [62], notes that:
The specific origin of dyslexia is unknown; however, the disorder is likely to run in families. To that end, dyslexia appears to be a hereditary disorder, with children who have a family history of learning and reading problems being more likely to acquire dyslexia than children who do not have a family history. Other variables that may contribute to the severity of the condition have also been discovered. Six separate genes, for example, have been discovered to potentially raise an individual’s chance of dyslexia. Four of these genes are known to be involved in neuronal migration, an early stage of brain formation that leads to the establishment of specialized brain regions… People have an inherent ability to recognize words as babies, which aids in language acquisition. However, these words are frequently identified as a single sound rather than as a collection of component sounds. For example, the word “refrigerator” will be recognized as having a certain sound and will not need to be broken down into the components “re,” “fri,” “ger,” and “ator” for the child to grasp. However, this is not the case when a child is learning to read or write. Reading and writing skill development is dependent on phonological processing, which is described as a child’s capacity to identify letters, assemble them into phonemes, and uses those phonemes to build or interpret a word. According to brain scans, the etiology of dyslexia is a decreased capacity to interpret words in this manner owing to changes in the development and function of particular areas of the brain.
It is already seen from the above quotation, that a gene explanatory stance is being endorsed as a possible cause for dyslexia. It is nonetheless to assert that this is not a disease but a condition that the individual is born with. Further research is ongoing to make certainly verifiable this possibility of understanding this condition by making reference to the genes.
How Does the Human will Mediate this Condition?
It should be noted that treatment for this sort of condition initially consists of “defining the disorder, advising parents, and possibly also advising teachers”. According to Schulte- Korne G, Subsequent treatment depends on the severity of dyslexia and psychological symptoms or concurrent disorders. Drug treatment is not beneficial for dyslexia. Only if a dyslexia sufferer also has attention deficit hyperactivity disorder (ADHD) can drug treatment for ADHD also improve learning abilities inside and outside school.
In defining the disorder, it is necessary to obtain a confirmed diagnostic picture of the condition. According to the DITC (Dyslexia in the Classroom) handbook, done by the International Dyslexia Association [63], a comprehensive evaluation typically includes intellectual and academic achievement testing, as well as an assessment of the critical underlying language skills that are closely linked to dyslexia. These include receptive (listening) and expressive language skills, phonological skills including phonemic awareness, and also a student’s ability to rapidly name letters and names. A student’s ability to read lists of words in isolation, as well as words in context, should also be assessed. If a profile emerges that is characteristic of readers with dyslexia, an individualized intervention plan should be developed, which should include appropriate accommodations, such as extended time. The testing can be conducted by trained school or outside specialists.
Once the above is certified, then thinkers like Schulte- Korne G, holds that the treatment of Dyslexia should be moderated and this can be done in two forms: “the treatment of the core problems with reading and spelling and the treatment of any concurrent psychological disorders” (2010). As regards the treatment of the core problems with reading and spelling, He is of the opinion that:
Reading support depends on an individual child’s development. On the basis of detailed analysis of developmental status in reading, reading support should be provided regularly, at least once a week for at least a year. In addition to this therapy, establishing a reading-friendly family environment with frequent reading sessions and reading together can also substantially boost reading development… Spelling support must be given separately from reading support. As with reading support, individual developmental status must be determined at the outset. Support is then designed around this. Beginning with support in phonics (spelling individual sounds), children learn regular trends in spelling. For example, in English the diphthong is usually spelled using the digraph ou (it is occasionally spelled ow, as in fowl, but more often ou, as in found). There are similar examples for double consonants, which in English words only follow short vowels (filling with -ll-, but filing with -l-). Children also learn how to use this knowledge (2010).
The psychological problems that might be linked to dyslexia include ADHD, anxiety or depression to this psychotherapy is recommended. In addition to the aforementioned, persons with such condition who are suffering from anxiety and depression can be significantly helped by such treatment. If a sufferer also has ADHD, drug treatment is also indicated when the disorder is severe.
As it stands a huge responsibility resides on instructors of these dyslexic individuals (by instructors we mean, educators: teachers and tutors; Parents and professionals). To fully equip these instructors, the DITC handbook [63] recommends the following,
- Clarify or simplify written directions.
- Present a small amount of work.
- Highlight essential information.
- Use a placeholder in consumable material.
- Provide additional practice activities.
- Provide a glossary in content areas.
- Develop reading guides.
- Use an audio recording device.
- Use of assistive technology. Assistive technology products such as tablets, electronic readers/dictionaries/ spellers, text to speech programs, audio books, and more can be very useful tools.
- They also recommend further that other areas be explored like:
- Use explicit teaching procedures. Teachers can include explicit teaching steps within their lessons (i.e., present an advanced organizer, demonstrate the skill, provide guided practice, offer corrective feedback, set up independent practice, monitor practice, and review).
- Repeat directions. If directions contain several steps, break down the directions into subsets. Simplify directions by presenting only one portion at a time and by writing each portion on the chalkboard as well as stating it orally. When using written directions, be sure that students are able to read and understand the words as well as comprehend the meaning of sentences.
- Maintain daily routines. Many students with learning problems need the structure of daily routines to know and do what is expected.
- Provide a copy of lesson notes. The teacher can give a copy of lesson notes to students who have difficulty taking notes during presentations.
- Provide students with a graphic organizer. An outline, chart, or blank web can be given to students to fill in during presentations.
- Use step-by-step instruction. New or difficult information can be presented in small sequential steps. This helps learners with limited prior knowledge who need explicit or part-to-whole instruction.
- Simultaneously combine verbal and visual information. Verbal information can be provided with visual displays (e.g., on an overhead or handout).
- Write key points or words on the chalkboard/ whiteboard. Prior to a presentation, the teacher can write new vocabulary words and key points on the chalkboard/whiteboard.
- Use balanced presentations and activities. An effort should be made to balance oral presentations with visual information and participatory activities. Also, there should be a balance between large group, small group, and individual activities.
- Use mnemonic instruction. Mnemonic devices can be used to help students remember key information or steps in a learning strategy.
- Emphasize daily review. Daily review of previous learning or lessons can help students connect new information with prior knowledge [63].
From all that has been outlined so far, it is quite obvious where the treatment is directed to in what pertains to the dyslexic condition - it is the WILL of the individual.
It should be aptly noted that the will that is being considered here is not that which pertains to the moral sphere - free will. Even though the will that is considered takes under its shade the aspect of free will, what is being elaborated upon here is not the aforementioned.
The human will is a faculty in the human person that falls under the purview of his rationality. That is to say that the human person has a rationally composed will in addition to his intellect. The aspect of the will has been studied in psychology under the term of volition. According to P. Haggard, one can earmark five areas in which volition in the human person is elaborated. They include:
- Internal Generation: Volitional = Not Externally Triggered
- Decisional Control: Volition = Not Habitual, Not Automatic
- Goal Directedness: Reasons, Values, Outcomes
- Spontaneity
- Subjective Experience [64].
Of above listed, that which relates primarily to what is being espoused here is the subjective experience. Haggard notes saying that for an act to be volitional, one must be aware that one is acting and aware of initiating one’s act. For example, someone who sleepwalks is unaware of their walking action and did not choose to initiate it. Someone who makes a reflex action in response to an immediate stimulus, such as a sneeze, is aware of their action but is also aware that they did not choose to initiate it. In general, volitional actions feel entirely different than physically comparable involuntary movements (2019).
The conscious voluntary nature of an action arising from the human species can be dubbed as willful or volitional. In Wittgenstein perturbed thinking, he would ask, “what is left over if I subtract the fact that my arm goes up from the fact that I raise my arm?” [65]. The answer is already before us, which is conscious volitional impulse.
The preSMA and the remote areas connected to it (for instance the prefrontal cortex) has been considered neuroscientifically as the brain arena in which volition is triggered. The earlier concept of volition as based of a channeling from the soul to the brain is rejected by modern neuroscience. The volition is neurally based is what is being accepted today. As regards the preSMA, Haggard says that when Fried and colleagues stimulated the preSMA, patients reported ‘an urge’ to move a specific part of the contralateral body. As they had not yet actually moved, this could not be a retrospective intervention. When more-intense stimulation was applied through the same electrodes, the corresponding part of the patient’s body indeed moved on five of the six stimulations that were reported as producing both urge and movement. It is unclear whether the urge reported by the patients resembled the normal conscious experience of intending to act. Moreover, the experience evoked by stimulation might arise not in the preSMA itself, but in remote areas connected to it, such as the parietal cortex. However, such studies do at least suggest that a conscious experience akin to intention is part of the normal neural preparation for voluntary movement [66].
What has been stated above opens us up to a consideration as to whether a stimulation of the preSMA is fitting enough to pass as a conscious voluntary action or not. As an addendum Haggard notes that Future investigations should focus on decisions to inhibit voluntary action, and the contribution of predictive monitoring; these decisions involve a medial prefrontal area, anterior to the classical preSMA (2008).
It can be opined that the subjects did not have the desire, the willing desire, to engage in those consciously voluntary actions but they got this when a current got to their brains. Seeing the electrodes attached to the prefrontal region of the brain, leading to actions occasioned by the passing of an electric current, it can be said that they were induced into such actions or such desire to act was induced. In such wise, can it be said that those electrode mode trigger can pass for a subjective experience? In whatever way that we think of it, every volitional act must have a trigger, be it from without or within (from persons or from things). For thinkers like Otto Rank, the will has the capacity to organize the human self and inhibit instinctual drives [67]. The will is individually composed, that is to say that it distinguishes one person from another [68]. Therefore even if one is to have electrodes sending electric currents to the prefrontal area of the brain, it does not in any way ensure that the force of the will is carried out. That is to say that there might be an impulse (albeit a desire) to act, but there is always the will, which is either inhibits or aligns itself with that impulse or desire. The will is that powerful.
Conclusion: the Power of the will
It is necessary not to lose sight of where we are, namely the power of the will as regards dyslexia. The reference element here is dyslexia even though the umbrella element is brain functions. It is necessary to recall a statement that was earlier asserted, which is that the earlier concept of volition as based of a channeling from the soul to the brain is rejected by modern neuroscience. The volition is neurally based is what is being accepted today. What if neuroscience is viewing this from one side? I mean if electric current flowing to the prefrontal area of the brain can elicit volitional acts, who is to say that volitional acts arising from within do no map themselves out on areas of the brain? Can electrode inducing volitional acts be endorsed in not to simple acts (like the raising of one’s hand or the eating of a fruit in front of one)? Can such be used in complicated cases of choices made for instance in settling down with a partner or in the making of future bound choices etc. Complex choices might find the electric current electrode induction falling flat on its face. Using Ockham’s razor, it would be safe to say that the will, the power of volition which is trigger based, be it internal or external, has a fine connection to the biological- ness of the brain, as its activity is mapped neurally on the brain, whenever a volitional trigger is initiated. The volitional activity is a human activity and it is represented neurally in the brain, once it is about to be carried out and when it is carried out, and even after it is carried out.
In reference to the dyslexic situation, it is necessary to note that reinforcement via specific channeling and focusing of the mind to the activity that is to be carried out is necessary to producing a positive outcome. It should be stated that dyslexia is not an illness, it is a condition that can be dealt with by primarily a steering of the will of the dyslexic. Multitasking is not what is required, but mono-tasking that is able to yield the necessary result. Patient tutoring and guidance will enable the dyslexic to come to terms with his or her condition, leading him or her to adopt certain means (one that has been taught already to him or her) that will occasion the needed results for him or her in life. Willfully tailoring the dyslexic towards that which rewards, making him or her focus on attaining to the positives with the attendant rewards in store for such person, is able to assist ameliorate this condition. Once the dyslexic is made to habitually make us of the means of focusing, he or she becomes aware of how to use this means in achieving any result that there is. Focusing of the will (the enabling of the will power), can be seen even in habitual operations. Think of it this way:
When one begins an action that will eventually lead or become a habit, one is very conscious and quite bad in it. As one continues in such action, one becomes more effective and quite fluid in the execution of the action. It gets to the stage that one attains to the result even when one is not fully conscious (as one was when the action was first done). Many instances can be cited in reference to the above: typing, driving, playing any musical instrument (or even vices like: doing drugs). The seeming explanation to this is that there is a neural pathway in the entire mix of interconnecting neurons that was created and strengthened over time, such that once it is initiated, it seamlessly passes through till it reaches the point where its reward waits. A habit is in many cases aimed at a reward (selfish or even selfless).
When the will of the person is aimed towards getting at something, the person brings to bear all that he or she can muster to the attainment of that which he or she wants. One might add that there might be persons that are not this purposeful as regards getting to set targets. Yet we want to allude here, that each person is purposeful and will drive in what relates to him or her as an individual. That means, what works for or triggers me, might not work for or trigger you (this was earlier asserted as we noted that the will is individually composed, that is to say that it distinguishes one person from another.
The will is that nonphysical attribute of the intellectual faculty of the human person that is capped with the ability to making choices that bears an intellectual insignia to it. It is that power that enables one to focus on a set goal or target. Dyslexia can be many others, but it is foundationally an inability to focus. An enforcing of the will in arenas where this focus is lacking is all the treatment one needs (unless there are other underlying medical conditions that would require medical intervention). The one tutoring the dyslexic should himself or herself, be wilful in execution in anything that pertains to the individual with the condition.
References
-
Aristotle, Nicomachean ethics, III, i.
-
Hall RH (1977) The Voluntary and the Involuntary in Aristotle’s Nicomachean Ethics. University of Kansas Journal pp: 1-25.
-
Aquinas T (1270) De Malo VI.
-
Aquinas T (1485) Summa theologiae. 1a, 82: 1.
-
Scotus J D Opius Oxoniense. I, xvii (i-ii); II, xxiv-xxv, pp: 1300-1302.
-
Hobbes T (1651) Leviathan CHAPTER VI.: Commonly called the Passions and the Speeches by which they are Expressed. London: Penguin Books.
-
Hume D (1740) A Treatise of Human Nature VIII: “of Liberty and Necessity (Oxford: Oxford University Press 1967), pp: 368.
-
Locke J (1689) An Essay concerning Human Understanding.
-
Snowling MJ, Hulme C, Nation K (2020) Defining and Understanding Dyslexia: Past, Present and Future. Oxford Review of Education 46(4): 501-513.
-
Shankweiler D, Liberman IY, Mark LS, Fowler CA, Fischer FW (1979) The Speech Code and Learning to Read. Journal of Experimental Psychology: Human Learning and Memory 5(6): 531-545.
-
Snowling M, Hulme C (1994) The Development of Phonological Skills. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences 346(1315): 21-27.
-
Orton ST (1937) Reading, Writing and Speech Problems in Children. (London: Chapman & Hall, 1937).
-
Bannatyne A (1974) Diagnosis: A Note on Recategorization of the Wisc Scaled Scores. Journal of Learning Disabilities 7: 272-274.
-
Rogers EM (1983) Diffusion of Innovations. Free Press, New York, pp: 1-236.
-
Shaywitz SE, Escobar MD, Shaywitz BA, Fletcher JM, Makuch R (1992) Evidence that Dyslexia may Represent the Lower Tail of a Normal Distribution of Reading Ability. N Engl J Med 326(3); 145-150.
-
Fletcher JM, Lyon GR, Fuchs LS, Barnes MA (2019) Learning Disabilities: From Identification to Intervention. In: 2nd Edition (Edn.), NYC: The Guilford Press.
-
Pennington BF, McGrath LM, Peterson RL (2019) Diagnosing Learning Disorders: From Science to Practice. In: 3rd Edition (Edn.), NYC: The Guilford Press.
-
Lyon GR, Shaywitz SE, Shaywitz BA (2003) Defining Dyslexia, Comorbidity, Teachers Knowledge of Language and Reading: A Definition of Dyslexia. Annals of Dyslexia 53: 1-14.
-
Elliott JG (2020) It’s Time to Be Scientific about Dyslexia. Reading Research Quarterly 55(S1): S61-S75.
-
Cooke A (2001) Working Party of the Division of Educational and Child Psychology of the British Psychological Society. Critical Response to Dyslexia, Literacy and Psychological Assessment. (Report by a Working Party of the Division of Educational and Child Psychology of the British Psychological Society). A view from the chalk face. Dyslexia. pp: 47-52.
-
Ryder D, Norwich B (2018) What’s in a name? Perspectives of Dyslexia Assessors Working with Students in the UK Higher Education Sector. Dyslexia 24(2): 109-127.
-
Asghar ZB, Siriwardena AN, Elfes C, Richardson J, Larcombe J, et al. (2018) Performance of candidates disclosing dyslexia with other candidates in a UK medical licensing examination: Cross-sectional study. Postgrad Med J 94(1110): 198-203.
-
Asghar Z, Williams N, Denney M, Siriwardena AN (2019) Performance in Candidates Declaring Versus those not Declaring Dyslexia in a Licensing Clinical Examination. Med Educ 53(12): 1243-1252.
-
Vellutino FR, Fletcher JM, Snowling MJ, Scanlon DM (2004) Specific reading disability (dyslexia): what have we learned in the past four decades? Journal of Child Psychology and Psychiatry 45(1): 2-40.
-
Snowling MJ, Nash HM, Gooch DC, Thomas MEH, Hulme C, et al. (2019) Developmental outcomes for children at high risk of dyslexia and children with developmental language disorder. Child Development 90(5): e548-e564.
-
Pennington BF (2006) From single to multiple deficit models of developmental disorders. Cognition 101(2): 385-413.
-
Snowling MJ, Lervag MM (2016) Oral language deficits in familial dyslexia: A meta-analysis and review. Psychol Bull 142(5): 498-545.
-
Saksida A, Iannuzzi S, Bogliotti C, Chaix Y, Demonet JF, et al. (2016) Phonological skills, visual attention span, and visual stress in developmental dyslexia: Insights from a population of French children. Developmental Psychology 52(10): 1503-1516.
-
White S, Milne E, Rosen S, Hansen P, Swettenham J, et al. (2006) The role of sensorimotor impairments in dyslexia: A multiple case study of dyslexic children. Dev Sci 9(3): 237-255.
-
Nation K, Margaret J, Snowling (1998) Semantic Processing and the Development of Word-Recognition Skills: Evidence from Children with Reading Comprehension Difficulties. Journal of Memory and Language 39(1): 85-101.
-
Saskia K, Lyndsey N, Anne C, Naama F, Genevieve M (2012) When ‘slime’ becomes ‘smile’: Developmental letter position dyslexia in English. Neuropsychologia 50(14): 368-3692.
-
Nation K, Mak MHC (2019) Orthographic learning and learning to read: Implications for developmental dyslexia. In: Compton DL, Washington J, McCardle P (Eds.), Dyslexia 101: Revisiting etiology, diagnosis, treatment and policy, pp.71-81.
-
Hulme C, Nash HM, Gooch D, Lervag A, Snowling MJ (2015) The foundations of literacy development in children at familial risk of dyslexia. Psychol Sci 26(12): 1877-1886.
-
Angold A, Costello EJ, Erkanli A (1999) Comorbidity. J Child Psychol Psychiatry 40(1): 57-87.
-
Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M (2009) Defining comorbidity: implications for understanding health and health services. Ann Fam Med 7(4): 357-363.
-
Bishop DVM, Adams C (1990) A prospective study of the relationship between specific language impairment, phonological disorders and reading retardation. J Child Psychol Psychiatry 31(7): 1027-1050.
-
Catts HW, Adlof SM, Hogan TP, Weismer SE (2005) Are specific language impairment and dyslexia distinct disorders? J Speech Lang Hear Res 48(6): 1378-1396.
-
Bishop DV, Snowling MJ, Thompson PA, Greenhalgh T, the CATALISE-2 consortium (2017) Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J Child Psychol Psychiatry 58(10): 1068- 1080.
-
Rochelle KSH, Talcott JB (2006) Impaired balance in developmental dyslexia? A meta-analysis of contending evidence. J Child Psychol Psychiatry 47(11): 1159-1166.
-
Gooch DC, Hulme C, Nash HM, Snowling MJ (2014) Comorbidities in preschool children at risk of dyslexia: The role of language ability. J Child Psychol Psychiatry 55(3): 237-246.
-
Pennington BF, Bishop D (2009) Relations among speech, language and reading disorders. Annu Rev Psychol 60(1): 283-306.
-
Carroll J, Maughan B, Goodman R, Meltzer H (2005) Literacy difficulties and psychiatric disorders: Evidence for co-morbidity. J Child Psychol Psychiatry 46(5): 524-532.
-
Francis DA, Caruana N, Hudson JL, McArthur GM (2019) The association between poor reading and internalising problems: A systematic review and meta- analysis. Clin Psychol Rev 67: 45-60.
-
Rose J (2009) Identifying and teaching children and young people with dyslexia and literacy difficulties (DCSF- 00659-2009). DCSF Publications.
-
(2013) The Diagnostic and Statistical Manual of Mental Disorders. In: 5th (Edn.), DSM–5; American Psychiatric Association.
-
Moll K, Snowling MJ, Hulme C (2020) Introduction to the special issue “comorbidities between reading disorders and other developmental disorders”. Scientific Studies of Reading 24(1): 1-6.
-
Landerl K, Moll K (2010) Comorbidity of learning disorders: Prevalence and familial transmission. J Child Psychol Psychiatry 51(3): 287-294.
-
(2023) British Dyslexia Association, Bracknell UK.
-
Pandey S, Agarwal S (2014) Dyscalculia: A Specific Learning Disability among Children. Scientific and Technical Information Processing 2: 912-918.
-
Richards TL, Berninger VW (2008) Abnormal fMRI Connectivity in Children with Dyslexia During a Phoneme Task: Before But Not After Treatment. J Neurolinguistics 21(4): 294-304.
-
Eckert MA, Leonard CM, Richards TL, Aylward EH, Thomson J, et al. (2003) Anatomical correlates of dyslexia: frontal and cerebellar findings. Brain 126(Pt 2): 482-494.
-
Eden GF, Jones KM, Cappell K, Gareau L, Wood FB, et al. (2004) Neural changes following remediation in adult developmental dyslexia. Neuron 44: 411-422.
-
Fulbright RK, Jenner AR, Mencl WE, Pugh KR, Shaywitz BA, et al. (1999) The cerebellum’s role in reading: a functional MR imaging study. AJNR Am J Neuroradiol 20: 1925-1930.
-
Horwitz B, Rumsey JM, Donohue BC (1998) Functional connectivity of the angular gyrus in normal reading and dyslexia. Proc Natl Acad Sci U S A 95: 8939-8944.
-
Paulesu E, Frith U, Snowling M, Gallagher A, Morton J, et al. (1996) Is developmental dyslexia a disconnection syndrome? Evidence from PET scanning. Brain 119(Pt 1): 143-157.
-
Pugh K, Mencl W, Shaywitz B, Shaywitz S, Fulbright R, et al. (2000) The angular gyrus in developmental dyslexia: Task-specific differences in functional connectivity within posterior cortex. Psychol Sci 11: 51-56.
-
Richards TL, Berninger VW, Aylward EH, Richards AL, Thomson JB, et al. (2002) Reproducibility of proton MR spectroscopic imaging (PEPSI): comparison of dyslexic and normal-reading children and effects of treatment on brain lactate levels during language tasks. AJNR Am J Neuroradiol 23: 1678-1685.
-
Schulte KG, Grimm T, Nothen MM, Muller MB, Cichon S, et al. (1998) Evidence for linkage of spelling disability to chromosome 15. Am J Hum Genet 63: 279-282.
-
Shaywitz SE, Shaywitz BA, Pugh KR, Fulbright RK, Constable RT, et al. (1998) Functional disruption in the organization of the brain for reading in dyslexia. Proc Natl Acad Sci USA 95: 2636-2641.
-
Shaywitz SE, Shaywitz BA, Fulbright RK, Skudlarski P, Mencl WE, et al. (2003) Neural systems for compensation and persistence: young adult outcome of childhood reading disability. Biol Psychiatry 54: 25-33.
-
Simos PG, Breier JI, Fletcher JM, Bergman E, Papanicolaou AC (2000) Cerebral mechanisms involved in word reading in dyslexic children: A magnetic source imaging approach. Cereb Cortex 10(8): 809-816.
-
Macchi W (2022) Dyslexia: Causes and Effects in Children. Common Disord Deaf Stud Hearing Aids 10: 219.
-
(2023) International Dyslexia Association. DITC Handbook 2017.
-
Haggard P (2019) The Neurocognitive Bases of Human Volition. Annual Review of Psychology 70: 9-28.
-
Wittgenstein L (1953) Philosophical Investigations. In: 3rd (Edn.), Hoboken-NJ: Wiley, UK.
-
Haggard P (2008) Human volition: towards a neuroscience of will. Nat Rev Neurosci 9(12): 934-946.
-
Rank O (1968) Will therapy and truth and reality. Alfred Knopf, New York.
-
Hafstein S (1978) Will, Choice and Fate Perspectives on Rankian thought. J Otto Rank Assoc 1(13): 65-79.
- A Review of Gene Therapy for Parkinson's Disease to Control Dopaminergic Neurons
- Late-Onset Myasthenia Gravis in a Patient with Recurrent Breast Cancer: A Case Report
- Covid-Induced Dystonia and Opsoclonus: A Case Report
- Generalized Tonic-Clonic Seizure in a Pediatric Patient with Sunflower Syndrome: A Case Report
- Comparison of Doppler Guided Seldinger Technique Versus Classic Palpatory Seldinger Technique for Radial Artery Cannulation-an Open Label Randomized Controlled Trial
- Brown Sequard Syndrome: Understanding the Complexities of Spinal Cord Injury