“A Logical Reasoning of Spongy Myocardium”- A Case of LV Non Compaction Cardiomyopathy
Left ventricular noncompaction cardiomyopathy (LVNC) or spongy myocardium is a rare congenital disorder prominently distinguished by deep abnormal trabeculations and intertrabecular recesses which communicate with the ventricular cavity that can be detected on Transthoracic Echocardiography (TTE) or cardiac MRI (CMR) studies. LVNC can occur in isolation or coexists with other cardiac and/or systemic anomalies and the common clinical complications are heart failure, arrhythmias, and cardio embolism. The American Heart Association classified it as a primary genetic cardiomyopathy. We described the case of a 28years old young adult who presented with heart failure for the first time. Transthoracic echocardiography showed a trabeculated, sponge-like appearance of the ventricular apical and inferolateral segments. Following evaluation with CMR imaging revealed non compaction of the left ventricle. Here we discussed the diagnosis of this case and reviewed the medical literature that concerned to LVNC.
Introduction
Left ventricular non-compaction (LVNC) is an uncommon cardiomyopathy caused by intrauterine failure of the myocardium to compact in the absence of any coexisting congenital heart defects [1]. It was first described in 1926 by Grant as spongy myocardium. The prevalence rate in general population is between 0.05% and 0.25% [2, 3], though the American Heart Association classified it as a primary genetic cardiomyopathy it’s not easy to explain the genetic basis for the phenotype expression of LVNC. We can find cases of both hereditary and sporadic forms of LVNC and its not clear if the occurrence in childhood is has genetic basis as it also seen in adulthood. Some of the genes associated with the occurrence of LVNC include tafazzin, LDB3, LMNA, SCN5A, MYH7, and MYBPC3 [4, 5, 6, 7]. The clinical presentation varies from aymptomatic to developing heart failure, thromboembolism, ventricular arrhythmias and sudden cardiac death. However, most mode of presentation is heart failure associated with left ventricular systolic dysfunction [8, 9, 10].


However, this time patient presented with heart failure which was managed conservatively.

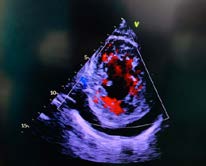

On initial evaluation with a TTE, trabeculae were located on the poster lateral wall of the left ventricle with blood flow into intertrabecular recesses detected by color Doppler mode (Figure 2). The ratio of non-compacted myocardium to compact myocardium at the end of systole was > 2:1 (Figure 3).
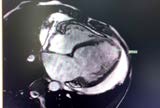
The patient also had moderate left ventricular systolic dysfunction and an ejection fraction of 30-35% with a markedly dilated left atrium and left ventricle. Moderate mitral and tricuspid regurgitation, moderate pericardial effusion with morphologically normal cardiac valves and no coexisting congenital anomalies were detected. Further evaluation by a cardiac MRI showed the 2 layered appearance of LV, with trabecular network and thinned overlying apical myocardium associated with apical hyperkinesia and late gadolinium contrast endocardia enhancement. The ratio of no compacted to compacted myocardium ratio was greater than 2.3 in the left ventricle, global hypo kinesis with depressed left ventricle ejection fractions of 35-40%, LA enlargement and with no evidence of a left ventricular thrombus (Figure 4).
These findings led to the diagnosis of LVNC. The patient had no sign cant arrhythmias during his hospital stay and the course was unattempt. After medical management with β- blockers, ACEI, loop diuretic, Spiro lactone and digoxin, he was discharged home with an advice of Automatic Implantable Cardioverter Defibrillator (AICD) placement.
Case Discussion
In summary, LVNC is an uncommon and controversial cause of cardiomyopathy. It is becoming a popular topic in the field of cardiology due to its multiple possible etiologies, pathogenesis, diagnostic criteria, and clinical course. Moreover, due to its highly variable manifestations, the management of this condition should be individualized. The main symptoms of LV noncompaction cardiomyopathy are similar to other patients with heart failure and the prevalence of isolated LVNC in patients with heart failure is reported to be 3 % [11]. Dyspnea is the most common symptom, followed by NYHA Class II-III heart failure, chest pain and arrhythmias [12]. A large percentage of patients are asymptomatic and appear to have a favorable prognosis [13]. Asymptomatic patients have a 2 % incidence of heart failure while symptomatic patients have a 61 % incidence [8].
Various genes are implicated in and are recognized to play some role in pathogenesis of LVNC. Screening of up to 3 generations of affected individuals has been recommended. A well-known gene SCN5A involved in the pathophysiology of multiple cardiac arrhythmias like Brugada syndrome, long QT type III is also associated with LVNC which was screened on 62 patients of Shan, et al. study [14]. Genetic testing may be useful in screening relatives of patients with LVNC and a known genetic mutation, but it is not helpful for making a diagnosis in patient with heart failure symptoms [15]. In our case screening of patient’s relatives up to 3 generation was did not showed any abnormality. In addition, though concern regarding myocardial biopsy of our patient was been made but we were unable perform and is the limitation of our study as the genetic cause couldn’t be ruled out.
There are currently no universally-accepted criteria for classifying and diagnosing LVNC. A typical echocardiographic examination of LVNC by Jenni criteria is the most popular TTE criteria till date with 3 major components proposed, all are required for diagnosis and are measured in the end systolic PSAX view [16].
- Two myocardial layers must be present, a thin compacted and a thick non compacted without any other congenital abnormalities.
- The ratio of non-compacted to compacted layer must be more than 2:1.
- Blood flow within the intertrabecular recesses which indicates communication with the ventricular cavity detected by color Doppler mode.
They also noted that noncompaction was predominantly localized to mid-lateral, apical, and mid-inferior areas of the LV [16]. Even using standardized TTE criteria, the diagnosis of LVNC can be inappropriately made based on the presence of prominent trabeculae in the left ventricle [17]. TTE has certain technical limitations like reliable quantitative delineation of LV wall thickness is dependent on adequate acoustic windows, particularly for the anterior and lateral segments that are easier to assess by CMR [18].
CMR provides non-oblique images with excellent and uniform contrast at the endocardial borders that encompass all levels and regions of the LV and permit virtually complete reconstruction of the chamber [19]. Jacquire criteria which diagnose LVNC is one of the popular CMR criteria with a sensitivity and specificity of 94% when the ratio of the trabeculated LV mass to the global LV mass is more than 20% [20]. A study by Petersen et al. using CMR found that pathological non-compaction had a non-compaction to compaction ratio >2.3 in end-diastole and the specificity and negative predictive values were both 99% [21].
Therefore TTE is usually the initial modality of choice for diagnosis followed by CMR for confirmation [22, 23]. A study done by Garcia- Pavia et al also suggested that definitive diagnosis will be made by the presence of both TTE –Jenni and CMR-Jacquire criteria with one of the followings [24]:
- Presence of either heart failure, arrhythmia or thromboembolism.
- Presence of a pathogenic mutation.
- Presence of regional wall motion abnormalities.
- Positive family history.
Patients with evidence of heart failure should receive guideline-directed medical therapy (GDMT). AICD
implantation should be considered in patients with obvious sustained ventricular tachycardia, inexplicable syncope or in patients with left ventricular EF less than 35% persisting despite adequate therapy, as a primary prevention of sudden cardiac death. Benefit of resynchronisation therapy has been described in a group of patients with LVNC [25]. Stollberger, et al. describe improvement of the systolic function in the left ventricle in the course regular control echocardiography in a number of patients with LVNC after bi-ventricular pacing [26]. In the case of patients with end stage heart failure despite adequate pharmacotherapy, the use of mechanical heart support or enlisting in a transplantation programmer must be considered. Conclusion LVNC is a rare myocardial disorder which is underreported in our part of the world and this case highlighted the importance of elaborative echocardiography and CMR for its diagnosis.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
-
Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R (1990) Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation 82(2): 507-513.
-
Weiford BC, Subbarao VD, Mulhern KM (2004) Noncompaction of the ventricular myocardium. Circulationm 109(24): 2965-2971.
-
Ritter M, Oechslin E, Sütsch G, Attenhofer C, Schneider J, et al. (1997) Isolated noncompaction of the myocardium in adults. Mayo Clin Proc 72(1): 26-31.
-
Monserrat L, Hermida PM, Fernandez X, Rodriguez I, Dumont C, et al. (2007) Mutation in the alpha- cardiac actin gene associated with apical hypertrophic cardiomyopathy, left ventricular non-compaction, and septal defects. Eur heart J 28(16): 1953-1961.
-
Vatta M, Mohapatra B, Jimenez S, Sanchez X, Faulkner G, et al. (2003) Mutations in Cypher/ZASPin patients with dilated cardiomyopathy and left ventricular non- compaction. J Am Coll Cardiol 42(11): 2014-2027.
-
Kenton AB, Sanchez X, Coveler KJ, Makar KA, Jimenez S, et al. (2004) Isolated left ventricular noncompaction is rarely caused by mutations in G4. 5, α-dystrobrevin and FK Binding Protein-12. Molecular genetics and metabolism 82(2): 162-166.
-
Hermida PM, Monserrat L, Castro BA, Laredo R, Soler R, et al. (2004) Familial dilated cardiomyopathy and isolated left ventricular noncompaction associated with lamin A/C gene mutations. Am J Cardiol 94(1): 50-54.
-
Bhatia NL, Tajik AJ, Wilansky S, Steidley DE, Mookadam F (2011) Isolated noncompaction of the left ventricular myocardium in adults: a systematic overview. J Card Fail 17(9): 771-778.
-
Stöllberger C, Wegner C, Finsterer J (2013) CHADS2- and CHA2DS2VASc scores and embolic risk in left ventricular hypertrabeculation/noncompaction. J Stroke Cerebrovasc Dis 22(6): 709-712.
-
Udeoji DU, Philip KJ, Morrissey RP, Phan A, Schwarz ER (2013) Left ventricular noncompaction cardiomyopathy: updated review. Ther Adv Cardiovasc Dis 7(5): 260-273.
-
Kovacevic PT, Jenni R, Oechslin EN, Noll G, Seifert B, et al. (2009) Isolated left ventricular noncompaction as a cause for heart failure and heart transplantation: a single center experience. Cardiology 112(2): 158-164.
-
Oechslin E, Jenni R (2011) Left ventricular non- compaction revisited: a distinct phenotype with genetic heterogeneity? Eur Heart J 32(12): 1446-1456.
-
Fazio G, Sutera L, Corrado G, Novo S (2007) The chronic heart failure is not so frequent in non-compactation. Eur Heart J 28(10): 1269-1269.
-
Quaife RA, Salcedo EE, Wolfel EE (2013) Non-compaction cardiomyopathy: underdiagnosed or over diagnosed? Current Cardiovascular Imaging Reports 6(6): 498-506.
-
Shan L, Makita N, Xing Y, Watanabe S, Futatani T, et al. (2008) SCN5A variants in Japanese patients with left ventricular noncompaction and arrhythmia. Mol Genet Metab 93(4): 468-474.
-
Jenni R, Oechslin E, Schneider J, Jost CA, Kaufmann PA (2001) Echocardiographic and pathoanatomical characteristics of isolated left ventricular non- compaction: a step towards classification as a distinct cardiomyopathy. Heart 86(6): 666-671.
-
Niemann M, Störk S, Weidemann F (2012) Left ventricular noncompaction cardiomyopathy: an overdiagnosed disease. Circulation 126(16): e240-e243.
-
Klues HG, Schiffers A, Maron BJ (1995) Phenotypic spectrum and patterns of left ventricular hypertrophy in hypertrophic cardiomyopathy: morphologic observations and significance as assessed by two- dimensional echocardiography in 600 patients. J Am Coll Cardiol 26(7): 1699-1708.
-
Grothues F, Smith GC, Moon JC, Bellenger NG, Collins P, et al (2002) Comparison of interstudy reproducibility of cardiovascular magnetic resonance with two- dimensional echocardiography in normal subjects and in patients with heart failure or left ventricular hypertrophy. J Am Coll Cardiol 90(1): 29-34.
-
Jacquier A, Thuny F, Jop B, Giorgi R, Cohen F, et al. (2010) Measurement of trabeculated left ventricular mass using cardiac magnetic resonance imaging in the diagnosis of left ventricular non-compaction. Eur Heart J 31(9): 1098-1104.
-
Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, et al. (2005) Neubauer S. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol 46: 101-115.
-
Finsterer J, Stoellberger C, Towbin JA (2017) Left ventricular noncompaction cardiomyopathy: cardiac, neuromuscular, and genetic factors. Nat Rev Cardiol 14(4): 224-237.
-
Stollberger C, Finsterer J (2004) Left ventricular hypertrabeculation/noncompaction. J Am Soc Echocardiogr 17(1): 91-100.
-
Garcia PP, Luis JDP (2014) Left ventricular noncompaction: a genetic cardiomyopathy looking for diagnostic criteria. J Am Coll Cardiol 64(19): 1981-1983.
-
Oginosawa Y, Nogami A, Soejima K, Aonuma K, Kubota S, et al. (2008) Effect of cardiac resynchronization therapy in isolated ventricular noncompaction in adults: Follow‐ up of four cases. J Cardiovasc Electrophysiol 19(9): 935- 938.
-
Stollberger C, Blazek G, Bucher E, Finsterer J (2008) Cardiac resynchronization therapy in left ventricular hypertrabeculation/non-compaction and myopathy. Europace 10(1): 59-62.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study