Anomalous Right Coronary Artery Origin from Left Sinus (R- ACAOS) Coronary Intervention Case Series; “Our Approach” - A Single Center Experience
Anomalous origin of right coronary artery (RCA) from the left coronary sinus is very rare coronary anomaly. Various individual case reports and case series have been reported in the literature. Patients with anomalous right coronary artery may often be asymptomatic and detected on incidental CT coronary angiogram or at times may present with acute coronary syndrome, sudden cardiac death or malignant arrhythmias. Coronary intervention in an anomalous right coronary artery is often challenging and any interventionist should be familiar with the incidence of this anomaly and always choose an optimal, safe and a good co- axial guiding catheter support for a successful intervention. Here, we present three individual cases with anomalous RCA presenting with positive stress test to acute coronary syndrome. All three cases underwent successful intervention with Judkins left 3.0 (JL 3.0) guiding catheter without any perioperative complications.
Introduction
Coronary arteries of anomalous origin are uncommon and encountered in 0.2-1.2% of patients undergoing percutaneous coronary intervention and represent a marked deviation of the normal anatomic pattern [1, 2]. Initially, these anomalies were diagnosed only during coronary angiographies performed in patients with valve disease or ischemic heart disease, and were considered to have no clinical significance. Later on, there began to be reports of sudden death in young athletes in whom the only sign of disease was an anomaly with origin in the coronary arteries [3, 4].
The clinical presentation is variable ranging from being asymptomatic to manifesting as angina, dyspnea, syncope, acute myocardial infarction, heart failure to sudden cardiac death. The most important factor to determine if the anomaly can cause sudden death or not in young individuals is determined by the dominance of the anomalous vessel as well as the course i.e; interarterial course (between aorta and pulmonary artery) . There are various theories to the mechanism of ischemia in an anomalous coronary artery including vessel spasm through the anomalous course, marked angulation at the origin of the anomalous artery and finally compression of the artery in the interarterial course when there is increase in pressure between the two vessels during exertion.
Anomalous RCA origin in the left sinus has been reported to be associated with acute myocardial infarction, arrhythmia or even sudden death. An anomalous origin of the right coronary artery (ARCA) from the left sinus of Valsalva has been reported in 6-27 % of patients with coronary anomalies [5]. This anomaly maybe associated with increased predisposition to developing significant epicardial atherosclerotic disease [6]. Because of the anomalous origin and the anatomical course of the artery, it is crucial to determine and make a systematic approach to evaluation of the coronary anatomy and distribution in order to avoid complications. In addition, it is essential to choose an ideal guiding catheter for selective angiogram and facilitate the proper lesion assessment and delivery of various devices. We report our three different cases with anomalous right coronary artery origin from left sinus that underwent successful percutaneous coronary intervention.
Case 1
A 32 year old male diabetic and hypertensive and current smoker referred from other center with diagnosis of acute inferior wall STEMI with initial coronary angiogram done revealing anomalous right coronary origin from
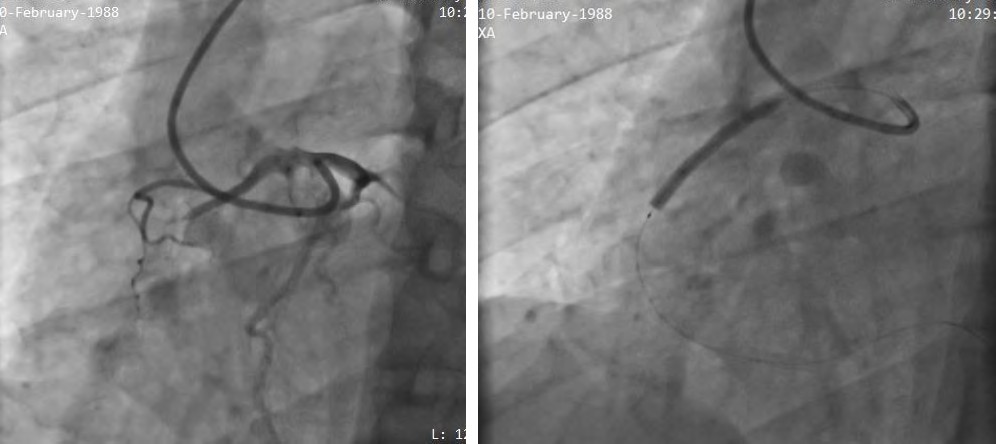
opposite sinus with total occlusion from mid segment of right coronary artery (Figure 1). His 2D echocardiogram revealed hypokinetic inferior wall with LV ejection fraction of 45%. We repeated the coronary angiogram through right femoral route which showed normal left coronary artery while difficult intubation to the right coronary artery with the Judkins right diagnostic catheter (JR3.5) from the conventional approach. We planned ahead for RCA intervention which was possible only with the JL 3.0 guiding catheter support .The lesion was crossed with a Sion Blue 0.014” (ASAHI Intec) and was predilated with 2.0x15mm Non-compliant (NC) balloon upto 20 atm (atmospheric pressure). A Combo Plus 3.0x38 mm Stent was deployed at 13 atm at mid–RCA and 2.75 x13 mm Combo plus stent deployed at 13 atm in the distal segment. Post dilatation was done with the 3.0x15mm NC balloon (Sapphire) at 18atm. A total of 10.000 IU of heparin was given with post procedure less than 10 % residual stenosis and no complications. He was later discharged on dual antiplatelets, statin, and beta blockers therapy.
Case 2
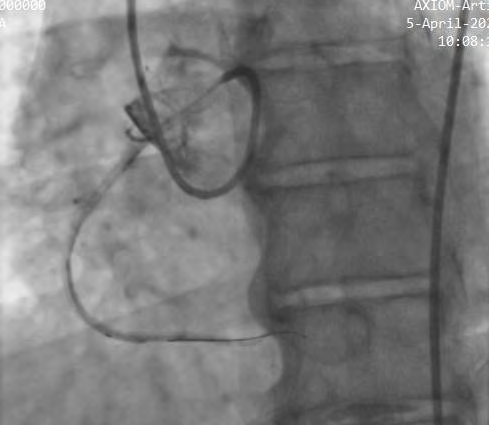
A 53 year old hypertensive and diabetic male with history of on and off exertional chest discomfort for 6 month duration was referred for a positive exercise stress test. Coronary angiogram done from right radial route revealed normal course and caliber of left coronary system with difficult engagement of the right coronary artery with the Tiger 5F catheter (Optitorque, TERUMO). Non selective engagement with a JR 6 F diagnostic catheter in the left sinus showed a 90 % tubular stenosis at the mid to distal segment of RCA. Selective cannulation of the RCA was finally done via 6 F JL 3.0 catheter with deeper prolapse of the catheter over the wire technique to facilitate the coaxial guiding into the anomalous RCA origin (Figure 2). The lesion was crossed with a floppy wire 0.014 “ BMW Universal wire ( Abbot , USA ) and subsequently direct stenting with Xience Xpedition stent 2.5x28mm (Abbot, USA) was done in the distal segment. No periprocedural complications noted and the patient was discharged the next day.
Case 3
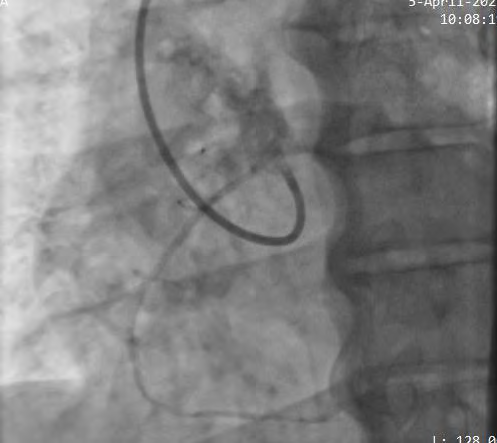
A 53 year male non diabetic non hypertensive underwent a coronary angiogram for recent Non ST elevation MI. She was medically managed at the other cardiac center and referred for further evaluation. His diagnostic angiogram from right radial artery revealed normal left coronary artery with difficult visualization of the right coronary artery. Another vascular access from the right femoral artery and subsequent angiogram done showed anomalous RCA origin from the left sinus at the same level with the left coronary origin. The RCA was annulated with the 7F JL 3.0 guiding

catheter with slight anticlockwise rotation in the level of left sinus which showed 70-80% stenosis at proximal to mid segment of right coronary artery (Figure 3). The lesion was crossed with 0.014 “ Sion Blue wire and Fielder XT coronary wire (Asahi Intec) loaded on a Corsair (Asahi Intec) micro catheter support . Then, the lesion was predicated with 1.5x 10 mm NC balloon followed by 2.5x15 mm NC balloon at 14 atm. A Promus Element (Boston Scientific) 2.5x32 mm stent was deployed in the mid RCA segment. The final result was good with well expanded stent and no post procedural complications.
Discussion
Detailed knowledge of the anomalous coronary artery is a must for all interventionists. Selective catheterization of an anomalous RCA may be technically difficult as well as time consuming. The acute angle of the origin of anomalous RCA with the aorta can create a slit- like orifice that may prevent selective cannulation, coaxial alignment, and adequate guide catheter support, which are essential for successful coronary intervention. Knowledge of variations in coronary artery origin can help in selecting appropriate catheters for diagnostic and therapeutic intervention [7]. Specifically, anomalous origin of the RCA from the left sinus of Valsalva was reported in 0.02% to 0.17% of coronary angiographies [8]. The artery is most commonly situated anterior and cephalad to the left main coronary artery.
Successful percutaneous treatment of stenotic lesions in anomalous RCA from left sinus Valsalva has been reported infrequently in the literature mostly in the form of small case series [9, 10, 11]. Cohen, et al [12] reported successful stenting in two cases of anomalous RCA with the use of a 6F Judkins left JL 5.0 guiding catheter. Topaz, et al [13] reported Amplatz AL-1 guiding catheter had been successfully used in 2 cases. Both undersized and oversized Judkins left catheter (JL3.0, JL 3.5, JL 4.0, JL 5.0) have been used successfully in many case series for anomalous RCA origin from left sinus as well as EBU 3.5 (Extra Backup) guiding catheter and Amplatz catheter (AL-1) in most case series [14]. In our case series, all three patients underwent successful anomalous RCA cannulation with JL 3.0 guiding catheter from femoral or radial route. The Judkins left catheter was pushed deep into the left sinus of Valsalva causing it to make an anterior and cephalad pointing U turn near the left coronary ostium. This larger curve prevented the catheter from automatically engaging the left coronary and allowed for selective cannulation of the anomalous RCA. Successful PCI of anomalous coronary arteries relies on optimal guiding catheters seating and backup support. In our experience, optimal guide support is relatively feasible and technically easier with a JL 3.0 guide catheter. There were no periprocedural complications and the total contrast volume and the duration of radiation exposure could be markedly minimized. However, with limited experience and rarity of the disease we cannot define the ideal guiding catheter support for the anomalous RCA origin and it differs between various individual operators worldwide. This case series in our three patients; highlights the importance of knowledge about the coronary anomaly as well as the challenges faced during intervention and the role of non-traditional guide catheters in the anomalous RCA origin.
Conclusion
Knowledge of different coronary anomalies is a must for all interventionists as well as cardiologists and optimal guide catheter selection is very essential for successful intervention in anomalous RCA origin from left sinus of Valsalva.
Conflict of Interest
All the authors have none to declare.
References
-
Kimbiris D, Iskandrian AS, Segal BL, Bemis CE (1978) Anomalous aortic origin of coronary arteries. Circulation 58(4): 606-615.
-
Click RL, Holmes DR, Vilestra RE, et al. (1989) Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival: a report from the coronary artery study. J Am Coll Cardiol 13(3): 531-537.
-
Barriales-Villa R, Moris C, Lopez-Muniz A, Hernandez LC, San Roman L, et al. (2001) Anomalias congenitas de las arterias coronarias en el adulto descritas en 31 anos de estudios coronariograficos en el Principado de Asturias: principales caracteristicas angiograficas clinicas. Rev Esp Cardiol 54(3): 269-281.
-
Roberts WC (1986) Major anomalies of coronary arterial origin seen in adulthood. Am Heart J 111(5): 941-963.
-
Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126,395 patients undergoing coronary angiography. Catheter Cardiovase Diagn 21(1): 28-40.
-
Jim MH, Siu CW, Ho HH Miu R, Wai-Luen L, et al (2004) Anomalous origin of the right coronary artery from the left coronary sinus is associated with early development of coronary artery disease. J Invasive Cardiol 16(9): 466- 468.
-
Leberthson RR, Dinsmore RE, Bharati S, Rubenstein JJ, Caulfield J, et al. (1974) Aberrant coronary artery origin from the aorta. Diagnosis and clinical significance. Circulation 50(4): 774-779.
-
Douglas JS, French RH, King SB (1985) Coronary artery anomalies. In: King SB, Douglas JS, editors. Coronary arteriography and angioplasty. New York: McGraw-Hill; pp: 33-85.
-
DiSciascio G, Goudreau E, Goudreau E, Cowley MJ, Nath A, et al. (1990) Coronary angioplasty of anomalous coronary arteries. Notes on technical aspects. Catheter Cardiovasc Diagn 21(2): 106-111.
-
Musial B, Schob A, Marchena DE, Kenneth MK (1991) Percutaneous transluminal coronary angioplasty of anomalous right coronary artery. Catheter Cardiovasc Diagn 22(1): 39-41.
-
Chakraborty B, Chan CN, Tan A (1995) Percutaneous transluminal coronary angioplasty of an anomalous right coronary artery arising from a separate ostium in the left sinus of valsalva. A case report. Angiology 46(7): 629-632.
-
Cohen MG, Tollesun TR, Peter RH, Harrison JK, Sketch MH (2002) Successful percutaneous coronary intervention with stent implantation in anomalous right coronary arteries from the left sinus of valsalva: a report of two cases. Catheter Cardiovasc Interv 55(1): 105-108.
-
Oral D, Dagalp Z, Pamir G, Alpman A, Omurlu K, et al. (1996) Percutaneous transluminal coronary angioplasty of anomalous coronary arteries. Case reports. Angiology 47(1): 77-82.
-
Uthayakumaran K, Subban V, Lakshmanan A, Pakshirajan B, Solirajaram R, et al (2014) Coronary intervention in anomalous origin of the right coronary artery (ARCA) from the left sinus of valsalva (LSOV): a single center experience. indian heart journal 66(4): 430-434.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study