Infundibular “Spasm” Masquerading as Failed Balloon Pulmonary Valvuloplasty in an Infant and its Dramatic Response to Beta Blocker
A 3-month-old infant with severe valvular PS showed significant dynamic infundibular obstruction which masqueraded as residual PS following Balloon Pulmonary Valvuloplasty (BPV). The obstruction responded dramatically to intravenous metoprolol. Interventionalists should be familiar with this occurrence to avoid damage to pulmonary valve by further balloon dilatation.
Introduction
Pulmonary valve balloon dilatation is an established procedure by now. Thousands of children have undergone PVBD since its description by Kan in 1982 [1]. In the earlier era using a Balloon: Annulus ratio (BAR) of at least 1.2 was the common practice to avoid suboptimal valve opening, however it carries the risk of development of significant valvular insufficiency. Many institutes including that of the authors now a day adopted a protocol of using a lower BAR (<1.1) to avoid the above complication [2]. In some cases, mainly in older children and adults, relief of valvular stenosis may unmask a dynamic infundibular obstruction resulting in a persistent residual right ventricular outflow gradient [3]. This dynamic subvalvular obstruction may masquerade (mistaken) as residual PS due to sub optimal dilatation especially when using a lower BAR. Meticulous analysis of post procedural waveform may help to differentiate between the two. Post procedural use of propranolol generally reduces this dynamic infundibular gradient as well as helps in differentiating dynamic obstruction from fixed obstruction [4].
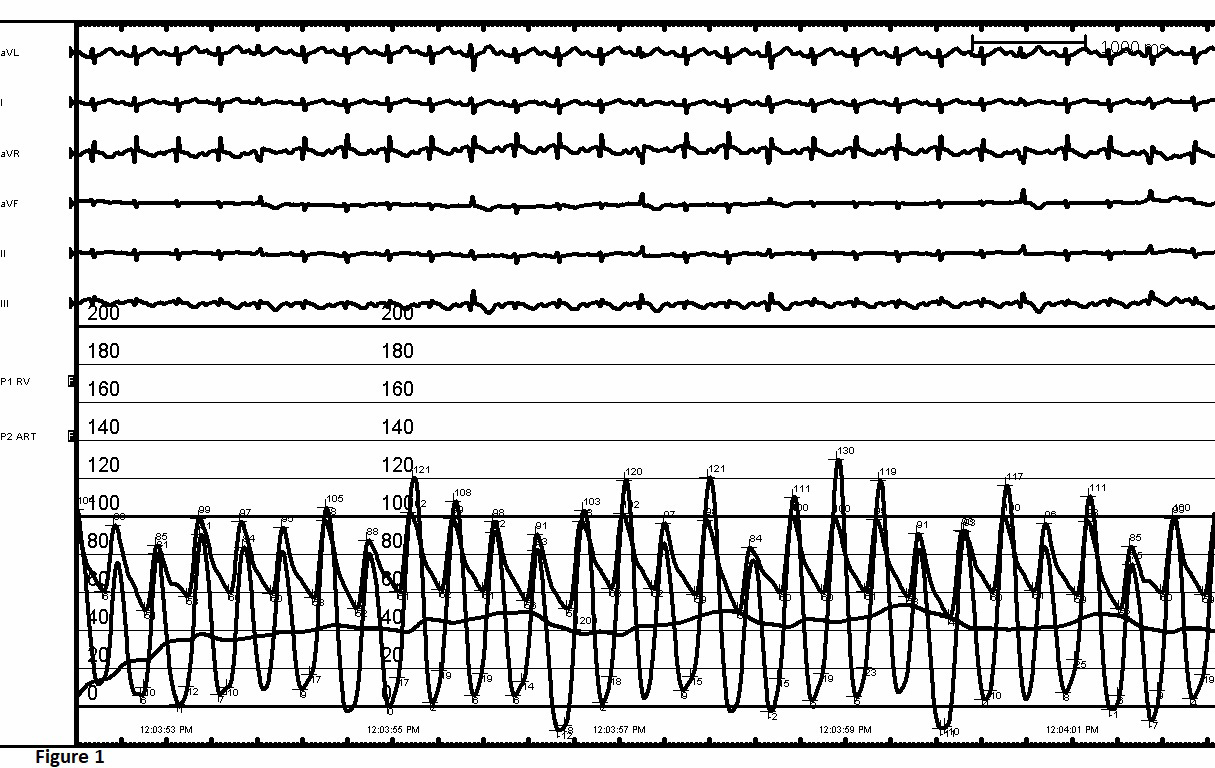
A three-month-old male child presented with feeding difficulty, failure to thrive and progressive fast breathing since last one month. On clinical examination a grade 3/6 ejection systolic murmur at the parasternal area with a systolic ejection click was noted. ECG showed right axis deviation and right ventricular hypertrophy. Echocardiography revealed severe valvular PS (Peak PG of 90 mmHg) with doming of anatomically normal leaflets and normal biventricular function. Being symptomatic child was taken for balloon pulmonary valvuloplasty shortly after diagnosis. After performing right heart study, which showed normal RV function and systemic RV pressure (Figure 1), we crossed the pulmonary valve with a 0.035 mm straight Terumo wire. Balloon dilatation of the pulmonary valve was done with a low profile Tyshak (8 mm x 2 cm) balloon.
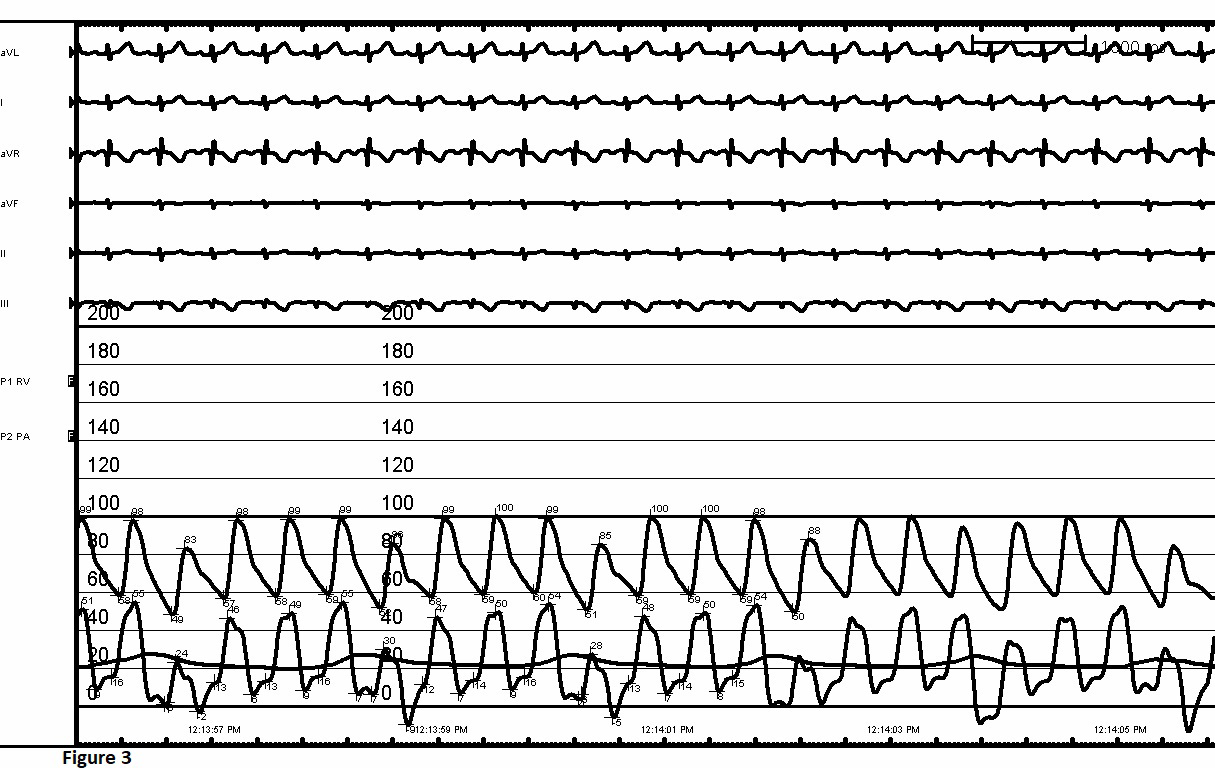
The waist disappeared after second dilatation. However, decrease of RV pressure was suboptimal (100 mm Hg to 80 mm of Hg) (Figure 2). Initial intuition for the presence of residual gradient was attributed to suboptimal valvular dilatation due to the usage of a smaller balloon (BAR of 1.05). The pressure waveform of right ventricle did not show a significant bifid square top pattern that is usual after a successful PVBD. A repeat angiogram showed development of significant dynamic infundibular obstruction. We used 0.1 mg/kg injection Metoprolol; following which RV pressure decreased to 45 mm Hg and pressure gradient across the valve decreased to 24 mm Hg within a minute. The waveform also changed. (Figure 3) No post procedural PR was noted. Child was discharged after 24 hrs of observation on 2mg/kg/ day of oral Propranolol.
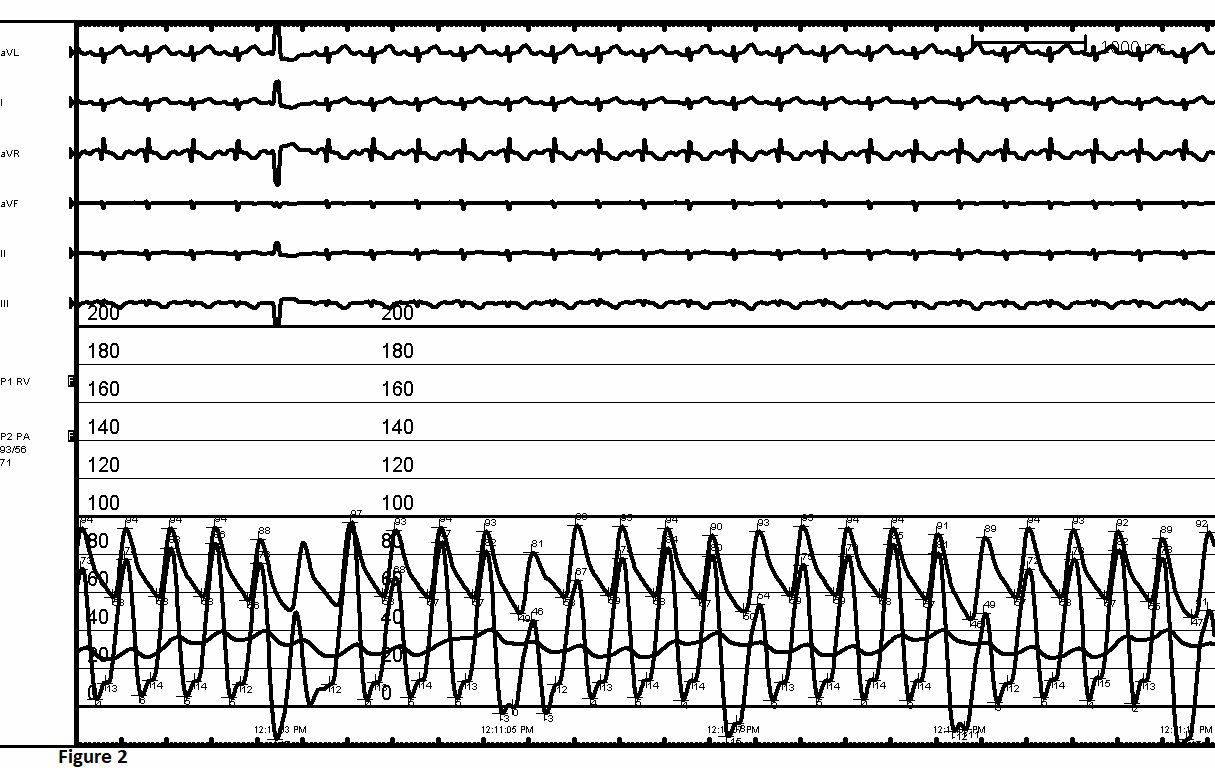
Showing persistence of RV pressure due to Dynamic Infundibular Obstruction.
Discussion
The conventional practice in balloon pulmonary valvuloplasty is to use a balloon size which is 1.2 to 1.4 times that of the PV annulus (BAR 1.2 to 1.4) [5]. In our institution we typically use a BAR of 1.0 to 1.1. Dynamic Infundibular stenosis is a phenomenon frequently encountered following balloon pulmonary valvuloplasty. It can masquerade as residual PS if not analysed properly by angiography and pressure tracing. The degree of this dynamic obstruction is directly related to the age of the patient and the severity of PS [6]. To avoid development of this infundibular hypertrophy early intervention is advised even in asymptomatic patients with severe PS. It is uncommon to see significant dynamic obstruction below 6 months of age. Generally, this dynamic obstruction responds well to beta-blockers and the sub- valvular muscle hypertrophy resolves within 6 months. However, our patient responded dramatically to injectable metoprolol within one minute which is seldom seen. He was discharged after 24 hrs of observation on oral propranolol therapy.
Conclusion
A conservative BAR of 1.0 to 1.1 should be initially used during BPV in neonates and infants. Possibility of development of dynamic infundibular obstruction following Balloon pulmonary valvuloplasty should always be kept in mind even in infants and neonates. In these scenarios on-table intravenous Metoprolol should be tried under hemodynamic monitoring.
Acknowledgement
We thank Professor Shyam S Kothari for his valuable advice in the preparation of the Manuscript.
Declarations
- Ethical Approval: The case report has been submitted to the journal as per the ethical guidelines of the Institute Ethics committee.
- Conflict of Interest: On behalf of all authors, the corresponding author states that there is no conflict of interest.
- Informed Consent: Informed consent has been taken from parents before the procedure and for publishing.
References
-
Kan JS, White RI, Mitchell SE, Gardner TJ (1982) Percutaneous balloon valvuloplasty: a new method for treating congenital pulmonary-valve stenosis. N Engl J Med 307: 540-542.
-
Pathak SJ, Pockett CR, Moore JW, Howaida GElS (2016) Effect of balloon: annulus ratio on incidence of pulmonary insufficiency following Valvuloplasty. Congenit Heart Dis 11(5): 415-419.
-
Thapar MK, Rao PS (1989) Significance of infundibular obstruction following balloon valvuloplasty for valvar pulmonic stenosis. Am Heart J 118: 99-103.
-
Moulaert AJ, Buis-Liem TN, Geldof WC, J Rohmer (1976) The post valvulotomy propranolol test to determine reversibility of the residual gradient in pulmonary stenosis. J Thorac Cardiovasc Surg 71(6): 865-868.
-
Rao PS (2007) Percutaneous balloon pulmonary valvuloplasty: state of the art. Cathet Cardiovasc Diagn 69(5): 747-763.
-
Thapar MK, Rao PS (1990) Use of propranolol for severe dynamic infundibular obstruction prior to balloon pulmonary valvuloplasty (a brief communication). Cathet Cardiovasc Diagn 19(4): 240-241.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study