Heart Rate Recovery Patterns Following Treadmill Test in Normal Individuals
Previous studies evaluating heart rate recovery following treadmill test have significant limitations. We evaluated heart rate recovery pattern in ninety five normal individuals of both genders and different age groups after strictly excluding any cardiac or systemic illness. We observed three distinct patterns of heart rate recovery. Some individuals had significant fall in heart rate during the first minute of recovery. Second group had greater reduction in heart rate during second and third minute of recovery. The third group had nearly similar fall in heart rate during first minute of recovery and during next two minute. However all individuals had a reduction of fifty beats per minute or more during initial three minutes of recovery. Subsequently reduction in heart rate was very slow. None of the individuals reached pre-exercise heart rate up to the end of seven minutes of recovery. Our observations will help better planning of future studies trying to correlate significance of heart rate recovery with diagnosis or prognosis.
Introduction
Heart rate response during exercise and recovery are considered important in interpretation of exercise stress test [1]. In normal individuals, there is a rapid fall in heart rate during recovery phase of stress test. It is considered a sign of circulatory efficiency and fitness [2]. Late heart rate recovery considered to suggest cardiac dysfunction and poor long term prognosis [3, 4, 5, 6, 7, 8, 9, 10, 11]. However, there is no clear recommendation which can be applied to an individual under question. This is because of several factors.
Firstly, some workers have studied only males [12]. It has been shown that men have lower parasympathetic drive and less rapid heart rate recovery [13, 14].
Secondly, different workers have used different recovery protocols. Some workers have used a cool down walking at 1.5 mph at 2.5% grade for two minutes [4, 5]. Others have used suppine position immediately after exercise.6 It has been shown that a cool down period decreases diagnostic sensitivity [15]. Putting the patient immediately in suppine position increases venous return resulting in rapid decline in heart rate [6]. Shetler K, et al. has evaluated patients who assumed a sitting position after an exercise stress test [16]. Authorities also feel that recovery protocols have not yet been standardized in clinical practice and it is yet a challenge in heart rate recovery literature [14, 17].
Thirdly, heart rate recovery is defined as the difference between the peak heart rate and a specific time in recovery [18]. Different workers have measured heart rate recovery at different intervals from cessation of exercise. Some workers have measured heat rate thirty seconds after exercise [19, 20, 21]. Morise AP, et al. measured heart rate recovery at the end of one minute [9]. Nishmi EO, et al. measured heart rate recovery at the end of two minutes [5]. Antelmi I, et al. also observed that heart rate recovery was more pronounced in the first two minutes after stopping of exercise [14]. Adabag AS, et al. measured heart rate recovery after three minutes [22].
Fourthly, different workers have suggested different values for defining slow heart rate recovery depending on the protocol used. Morise AP, et al. have suggested that a heart rate recovery of twelve beats per minute or less in the first minute of recovery should be considered abnormal for those who undergo an upright cool down protocol [9]. Cole CR, Watanabe J, et al. have proposed a heart rate reduction of less than eighteen beats per minute as abnormal for patients assuming a supine position immediately after the exercise stress test [3, 6]. Nishme EO, et al. have proposed a reduction of less than 22 beats per minute within two minutes of recovery as abnormal for those who assumed a sitting position after exercise [5]. Adabag AS, et al. has shown that a heart rate recovery of less than fifty beats per minute is an independent predictior of all cause death in asymptomatic men [22]. Antelmi I, et al. in a study of healthy asymptomatic individuals without any clinical or laboratory evidence of heart disease, found significant correlation between heart rate variability indices and heart rate recovery only in the third and fourth minute after exercise [14]. Johnson NP, et al. also observed that heart rate recovery after two minutes may be an independent predictor of adverse cardiovascular outcome [11].
Fifthly some authors have excluded persons younger than thirty years [5]. It is established that younger individuals have faster recovery of heart rate than older ones [14].
Most of the studies have evaluated high risk population. Study sample of Shelter K, et al. [16], Cole CR, et al. [23] consisted of patients referred for treadmill test due to clinical indications including patients referred for coronary angiography. It means that in these patients clinicians had high suspicion of coronary artery disease. Study sample of Cole CR, et al. [4] included subjects with ‘heart disease’ Detailed evaluation of the publication of Watanabe J, et al. [6] reveals that the group with abnormal heart rate recovery had significantly lower peak heart rate (P<0.0001), proportion of heart rate reserve used (P = 0.0001), peak MET (P=0.0001) and significantly higher incidence of angina (P=0.001), echocardiographic evidence of ischemia (P = 0.001) and increase in left ventricular size after exercise (P = 0.001). In the study of Nishime EO, et al. [5], cases had higher incidence of hypertension (P < 0.001), smoking (P<0.001), diabetes mellitus (P<0.001), insulin use (P <0.001), hypercholesterolemia (P < 0.001), use of lipid lowering drugs (P<0.001), prior CAD (P<0.001), prior myocardial infarction (P<0.001), prior coronary artery bypass grafting (P<0.001), higher systolic blood pressure (P<0.001) and higher intake of cardioactive drugs (P<0.001). These patients attained less MET (P<0.001), attained less peak heart rate (P<0.001) and had more chronotropic incompetence (P<0.001) and higher Duke Treadmill score (P<0.001), It is therefore clear that these patients were destined to have high mortality irrespective of their heart rate recovery.
Heart rate recovery is also influenced by age, gender, resting heart rate and peak heart rate [14]. There is no study that has evaluated heart rate recovery pattern in ‘normal’ individuals of different age group and both genders after strictly excluding various cardiovascular risk factors. Such data is necessary to correctly interprete the significance of heart rate recovery in a given individual.
We, therefore, evaluated heart rate recovery patterns in normal individual after strictly excluding any cardiovascular disease and conventional cardiovascular risk factors. We also tried to evaluate the correlation of heart rate, peak MET and percentage of age adjusted target heart rate attained by the individual.
Material and Methods
Inclusion criteria
- Absence of any cardiovascular symptoms.
- Absence of any family history of premature coronary artery disease on sudden cardiac death.
- Normal clinical examination.
- Normal resting twelve lead electrocardiograms i.e. absence of any evidence of ventricular hypertrophy, intraventricular conduction defects, preexcitation, ST- segment or T wave changes.
- Normal 2- dimensional and colour Doppler echocardiographic examination.
- Absence of any conventional cardiovascular risk factor e.g. smoking, hypertension, diabetes mellitus or dyslipidemia.
- Absence of any history of use of cardioactive drugs.
- No new electrocardiographic change on standing and during active hyperventilation prior to exercise.
- Absence of any chronic systemic illness.
- Absence of any clinical, electrocardiographic or echocardiographic evidence of left and/or right ventricular hypertrophy.
- Absence of any evidence of autonomic neuropathy.
- Patients who were not having pacemaker implantation.
- Resting heart rate above 55 beats per minute. Resting heart rate less than 55 beats per minute could be due to intrinsic disease of the sinoatrial node or inherently increased parasympathetic tone. These conditions could affect the heart rate response during exercise and recovery.
Exclusion criteria
- Patients with any contraindication for exercise stress testing [24].
- Conditions that could hamper exercise capacity e.g. debility, orthopaedic problems, haemoglobin concentration less than 10gm% left or right ventricular dysfunction chronic pulmonary disease or any evidence of pulmonary artery hypertension [25, 26].
- Conditions that could affect correct interpretation of exercise electrocardiogram e.g. new appearance of any intraventricular conduction defect or preexcitation during exercise [27].
- Development of any bradyarrhythmia, tachyarrhythmia or frequent premature beats during exercise.
- When any possibility of myocardial ischemia could not be excluded with confidence e.g. new development of any of the following findings during exercise or recovery-horizontal ST-segment depression of less than 1mm, upstoping ST-segment depression, ST-segment depression localized to inferior leads with significantly downsloping Pq segment, isolated shallow inversion of T waves, increasing frequency of premature ventricular beats.
Exercise test protocol
- Mason RE, et al. lead system was used. All twelve leads were recorded simultaneously [28].
- Bruce protocol was followed [29].
- Pre-exercise heart rate was measured before onset of exercise i.e. after standing and active hyperventilation.
- Exhaution rather than age adjusted target heart rate was taken as the end point to achieve maximal heart rate and exclude any possibility of exercise induced myocardial ischemia [30].
- Exercise was terminated if there was development of angina, any magnitude of ST-segment elevation, ST- segment depression of one mm, any intraventricular conduction defect, increasing frequency of premature ventricular contractions or inability to exercise from any cause [31].
- Patient was immediately put in supine position.
- Recovery was recorded for seven minutes. Recovery period was extended if indicated. Ninety five individuals qualified for final analysis (67 males and 28 females). Age ranged from 22 to 73 years.
Evaluation of heart rate
Computer derived heart rate was used for analysis. Heart rate wass calculated manually if it was felt that there was some error in computer calculation of heart rate. Age predicted maximal heart rate was calculated by the formula of i.e. 220-age [32].
Statistical Analysis
Difference between different groups was evaluated using unpaired ‘T’ test [33].
Results
Depending on time wise decline in heart rate during recovery period, we could identify their separate groups.
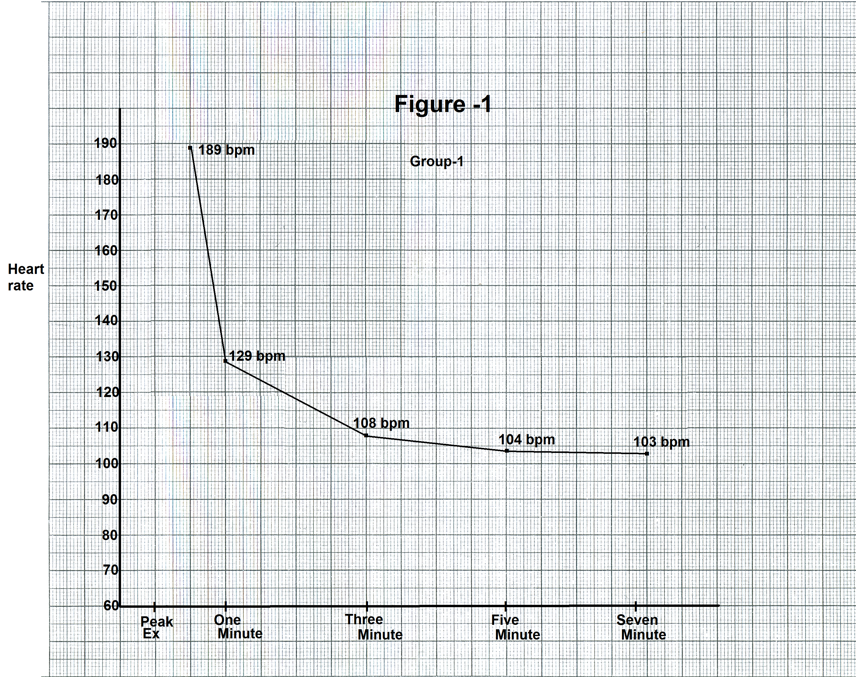
Group 1 Individuals showing maximum decline in heart rate during first minute of recovery. It included 57 individuals (41 males and 16 females). Representative graph from one case is shown in Figure 1.
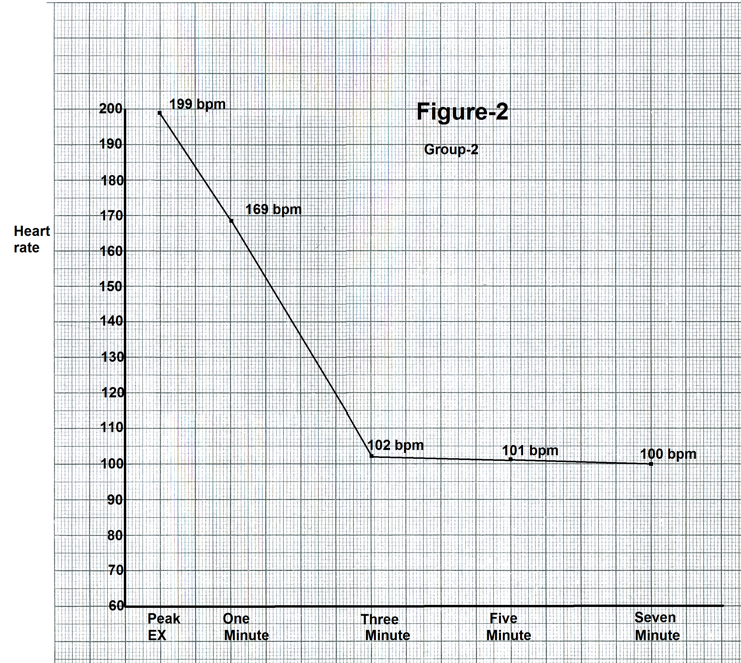
Group 2 Individuals showing maximum decline in heart rate during second and third minute of recovery. This group included 22 cases (17 males and 5 females). Representative graph from one case is shown in Figure 2.
Group 3 Individuals having no significant difference in decline in heart rate during first minute and during next two minutes. Representative graph from one case is shown in Figure 3.
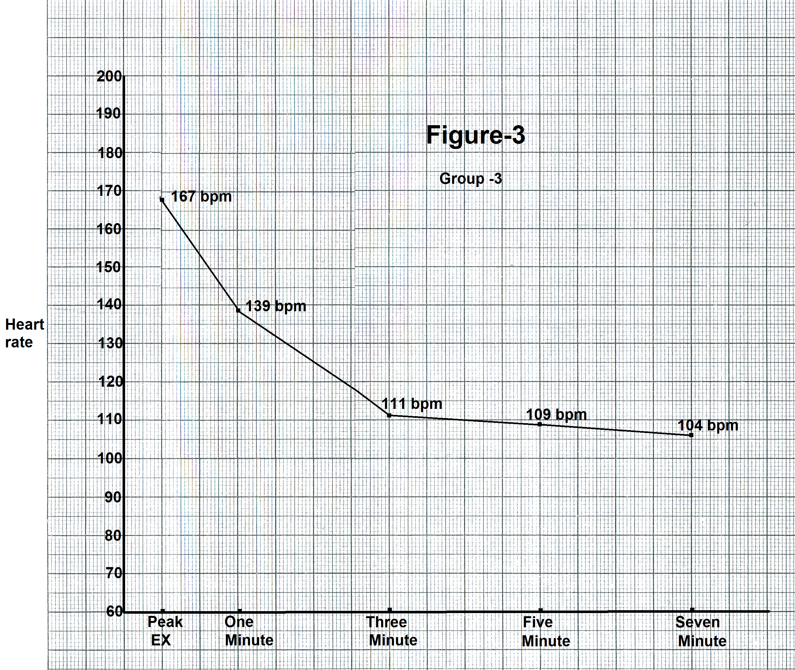
Difference of less than five beats per minute was considered insignificant. This group had 16 cases (9 males and 7 females) Baseline parameters of the three groups and the P values of differences are shown in Table 1. Individuals in group 1 were significantly younger than individuals of group
2 and 3 (P<0.001). Resting supine heart rate of individuals of group1 was also significantly lower than individuals of group 2 (P < 0.001) and group 3 (P<0.01). Resting supine systolic blood pressure was relatively higher in group 2 as compared to group 1 (P= 0.02) and group 3 (P< 0.01). There was no significant difference in the resting supine diastolic blood pressure in the three groups. Work load parameters of the three groups and the P values of difference are shown in the Table 2.
| Parameter (Mean±SD) | Group 1 | Group 2 | Group 3 | P values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| Age (years) | 28.16±14.02 | 43.54±12.32 | 49.5±12.38 | <0.001 | >0.10 | <0.001 |
| Sex M/F | 41/16 (2.6:1) | 17/5 (3.4:1) | 9/7 (1.28:1) | |||
| Resting HR/ min | 71.41±9.31 | 81.36±13.05 | 80.12±10.12 | <0.001 | >0.10 | <0.01 |
| SBP( mm Hg) | 119.82±9.31 | 124.36±9.55 | 116.87±10.22 | 0.02 | <0.01 | >0.10 |
| DBP (mm Hg) | 78.39±7.20 | 78.90±10.14 | 82.5±6.83 | >0.10 | >0.10 | >0.05 |
Table 1: Baseline parameters.
| Parameter (Mean±SD) | Group 1 | Group 2 | Group 3 | P values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| Exercise duration (minutes) | 9.56±1.61 | 8.95±1.56 | 8.25±1.64 | >0.10 | >0.10 | 0.01 |
| Peak MET | 10.96±1.67 | 9.80±2.25 | 9.34±1.88 | >0.10 | >0.10 | <0.02 |
| % of THR attained | 91.66±9.16 | 98.22±4.74 | 96.81±9.99 | 0.01 | >0.10 | >0.05 |
Table 2: Exercise parameters.
Work load parameters of the three groups and the P value of differences are shown in Table 2. Group 3 had relatively less total duration of exercise as compared to group 1 (P=0.01). Peak metabolic equivalent was also lower in group 3 as compared to group 1 (P<0.02). All individuals attained target heart rate. Percentage of target heart rate attained was marginally lower in group 1 (P=0.01).
Exercise parameters of the three groups and the P values of differences are shown in Table 3. There was no significant difference in the three groups regarding preexercise heart rate increase from resting heart rate to preexercise heart rate, peak heart rate, and total increase in heart rate over resting heart rate and total increase in heart rate over preexercise heart rate.
| Parameter (Mean±SD) | Group 1 | Group 2 | Group 3 | P values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| Pre-exercise HR/minute | 96.41±19.51 | 104.0±15.01 | 101.0±18.93 | >0.05 | >0.10 | >0.10 |
| Peak exercise HR/minute | 169.50±15.72 | 171.72±23.84 | 167.12±22.76 | >0.10 | >0.10 | >0.10 |
| Increase from resting HR to pre-exercise HR | 24.08±13.06 | 22.5±9.52 | 22.37±14.76 | >0.10 | >0.10 | >0.10 |
| Total increase in HR over resting HR | 95.52±14.85 | 91.90±24.41 | 87.06±22.04 | >0.10 | >0.10 | >0.10 |
| Total increase in HR over preexercise HR | 73.01±15.90 | 67.5±23.05 | 65.0±20.27 | >0.10 | >0.10 | >0.10 |
Table 3: Exercise heart rate parameters.
Heart rate recovery patterns in the three groups are shown in Table 4. Heart rate decline during the first minute of recovery was significantly higher (P< 0.001) in group 1 as compared to group 2 and 3. Heart rate recovery from the end of first minute to the end of third minute was significantly lower (P < 0.001) in group 1 as compared to group 2 and 3. There was minimal further decrease in heart rate in all the three groups from end of third minute to the end of fifth minute. Decline in heart rate from the end of 5th minute to the end of 7th minute was still smaller. However, statistically, it was more in group 2 (P<0.01). Total heart rate recovery from peak exercise to the end of 7th minute was significantly more in group 1 as compared to group 2 (P=0.02) and group 3 (P<0.001). None of the persons reached resting heart rate by the end of seventh minute. There was no significant difference between the three groups regarding difference between peak heart rate and heart rate at the end of seventh minute of recovery.
| Recovery time | Group 1 (Mean±SD) | Group 2 (Mean±SD) | Group 3 (Mean±SD) | P values | ||
|---|---|---|---|---|---|---|
| 1 v/s 2 | 2 v/s 3 | 1 v/s 3 | ||||
| From peak HR to end of 1st minute | 48.33+13.00 | 22.18+8.26 | 21.17+4.68 | <0.001 | >0.10 | <0.001 |
| From end of 1st minute to end of 3rd minute | 21.70+7.17 | 34.72+10.99 | 28.56+4.46 | <0.001 | >0.05 | <0.001 |
| from end of 3rd minute to end of 5th minute | 4.54+4.35 | 4.81+4.90 | 5.31+3.46 | >0.10 | >0.10 | >0.10 |
| From end of 5th minute to end of 7th minute | 2.01+2.34 | 5+4.56 | 2.62+2.38 | 0.01 | <0.01 | >0.10 |
| Total HR recovery by the end of 7th minute | 76.35+12.91 | 66.1 +19.14 | 61.93 + 9.71 | 0.02 | >0.10 | <0.001 |
| HR above resting HR at the end of 7th minute | 19.05+10.38 | 19.77+11.03 | 18.06+13.23 | >0.10 | >0.10 | >0.10 |
Table 4: Reduction in heart rate per minute during recovery phase.
We also analyzed the effect of gender on heart rate recovery (Table 5). There was no effect of gender on heart rate recovery in any of the three groups.
| Group | Heart rate recovery (Mean±SD) | P value | |
|---|---|---|---|
| Male | Female | ||
| Group 1 | 48.56±13.64 | 47.83±12.35 | > 0.10 |
| Group 2 | 36.06±10.54 | 31.16±12.38 | > 0.10 |
| Group 3 | 25.55±5.40 | 29.78±4.26 | 0.1 |
Table 5: Effect of Gender.
Discussion
Decline in heart rate during recovery after exercise stress test depends on decrease in the sympathetic drive and reactivation of the parasympathetic drive [23]. We observed significantly higher decline in heart rate during the first minute of recovery in group 1. Individuals of group 1 were significantly younger, had significantly lower resting supine heart rate, exercised for longer duration and attained higher metabolic equivalent (Table 2). Antelmi I, et al. also observed that younger individuals recovered faster than older individuals. They, however, observed the difference between the second to the fifth minute of recovery and not during the first minute of recovery as observed by us Antelmi I [14]. We observed that the decline in heart rate was significant only during the first three minutes of recovery. Subsequently the decline in heart rate was not significant. We observed that the resting heart rate was significantly lower in group 1 with maximal decline in heart rate during the first minute of recovery. This could be because of relatively higher parasympathetic tone in individuals of group 1. Rapid recovery of parasympathetic tone could be responsible for rapid heart rate recovery during first minute of recovery in individuals of group 1.
Antelmi I, et al. observed that the resting heart rate correlated significantly with heart rate recovery during the fourth and fifth minute [14]. Other workers have observed rapid decline in heart rate with in thirty seconds in players and athletes [19, 20, 21]. Decrease in the heart rate during the first two minutes of recovery relates to the return of vagal tone whereas decreasing sympathetic tone becomes important in the later stages of recovery [34, 35]. Our observations and observations of these workers suggest that younger individuals have greater parasympathetic activity and, therefore, greater heart rate recovery during the first minute. Our observations show that evaluation of heart rate during the first three minutes of recovery is more relevant than trying to evaluate heart rate recovery after three minutes.
Antelmi I, et al. observed that subjects with greater increase in heart rate during exercise had a faster recovery from second to fifth minute [14]. This relationship was not observed in the first minute after exercise. We, however, did not observe any correlation between heart rate recovery and magnitude of increase in heart rate during exercise in any of the three groups (Table 3). This difference in observation could be because of difference in the autonomic profile of tested individuals. Further, the primary aim of Antelmi I, et al. was to correlate heart rate recovery with 24 hours heart rate variability unlike our study that focused on variability in heart rate recovery patterns and their correlation with other parameters [14]. This difference in the primary aims of the studies could affect the results. Also, heart rate variability does not correlate with heart rate recovery. Antelmi I, et al. have themselves concluded that the hypothesis of association between heart rate recovery and 24 hours heart rate variability was not substantiated [14]. They observed that heart rate recovery was most pronounced in the first two minutes of recovery whereas strongest correlation between heart rate recovery and heart rate variability was identified at fourth minute of recovery. Our study showed that heart rate recovery had no correlation with increase in heart rate during exercise.
Antelmi I, et al. observed that heart rate recovery was more rapid in women than in men. They attributed it to higher parasympathetic drive in women as observed in their study on heart rate variability [13]. We did not observe any impact of gender on heart rate recovery in any group (Table 5).
Males have greater aerobic capacity and can take greater work load [36]. Longer duration of exercise and higher value of peak MET in group 1 of our study could to because of greater number of males in group 1. We used the formula of Fox et al 32 for calculating target heart rate (220-age). This resulted in greater calculated target heart rate in group 1 individuals who were significantly younger (Table 1). This can explain relatively lower percentage of target heart rate attained by individuals of group 1 inspite of the fact that there was no significant difference in the peak heart rate amongst the three groups.
We observed that maximum decrease in heart rate occurred in initial three minutes. Subsequently there was very slow and minimal decline in heart rate. Our study shows that normal individuals have a reduction of about 50 to 60 beats per minute in the first three minutes of recovery with further reduction of 5 to 10 beats per minute in next four minutes. Our study shows that normal individuals have a decline in heart rate by 50 to 60 beats per minutes by the end of third minute of recovery. Delayed recovery in heart rate suggests longer persistence of exercise induced increase in sympathetic activity during recovery. This could be because of slow recovery of ischemia induced left ventricular this function. This speculation is supported by long term follow up of asymptomatic individuals. Sylveis FR, et al. have observed that a heart rate recovery of less than 50 beats per minute was an independent predictor of all causes that in asymptomatic men [36].
We observed that none of the tested individuals reached resting heart rate even by the end of seventh minute of recovery (Table 4). This shows that, in normal individuals, sympathetic activity increased during exercise may not return to base line up to seven minutes after cessation of exercise [37].
Our study shows that there is significant interindividual variability in pattern of heart rate recovery following treadmill stress test. Messay D, et al. have also observed significant differences in exercise and recovery pattern among different category of players. This is probably due to interindividual variability in functions of sympathetic and parasympathetic system during exercise and recovery [19]. Heart rate variability is considered parameter of parasympathetic activity. Studies on heart rate variability have also shown significant interindividual variability [13].
Conclusion
Our study shows that, there is significant interindividual variability in heart rate recovery pattern following treadmill stress test in normal individuals However, all normal individual have a reduction of fifty beats per minute or more in initial three minutes of recovery. Reduction of less than 50 beats in initial three minutes of recovery can be considered abnormal. Our data will help planning of future studies correlating heart rate recovery patterns with long term prognosis in individuals without any clinical or laboratory evidence of any cardiac or other systemic illness.
References
-
Mittal SR (2021) Significance of heart rate profile during treadmill stress test - A critical appraisal. J Cardiol 5(1): 00015.
-
Master AM, Oppenheimer ET (1929) A simple exercise tolerance test for circulatory efficiency with standard tables for normal individuals. Am J Med Sci 177(2): 223- 243.
-
Cole CR, Blakstone EH, Pashkow FJ, Snader CE, Lauer MS (1999) Heart rate recovery immediately after exercise as a predictor of mortality. N Engl J Med 341(18): 1351- 1357.
-
Cole CR, Foody JM, Blackstone EH, Lauer MS (2000) Heart rate recovery after submaximal exercise testing as a predictor of mortality in cardiovascularly healthy cohort. Ann Intern Med 132(7): 552-555.
-
Nishime EO, Cole CR, Blackstone EH, Lauer MS (2000) Heart rate recovery and treadmill exercise score as predictor of mortality in patients referred for exercise ECG. JAMA 284(11): 1392-1398.
-
Watanabe J, Thamilarasan M, Blackstone EH, Thomas JD, Lauer MS (2001) Heart rate recovery immediately after treadmill exercise and left ventricular systolic dysfunction as predictor of mortality: the case for stress echocardiography. Circulation 104: 1911-1916.
-
Marshedi Meibady A, Larson MG, Levy D, O Donnel CJ, Vasan RS (2002) Heart rate recovery after treadmill exercise testing and risk of cardiovascular disease events (The Framingham Heart study). Am J Cardiol 90(8): 848- 852.
-
Vivekanathan DP, Blackstone EH, Pothier CE, Lauer MS (2003) Heart rate recovery as a predictor of mortality independent of the angiographic severity of coronary disease. J Am Coll Cardiol 42(5): 831-838.
-
Morise AP (2004) Heart rate recovery: Prediction for the risk to-day and target of therapy tomorrow?. Circulation 110(18): 2778-2780.
-
Gera N, Taillor LA, Ward RP (2009) Usefulness of abnormal heart rate recovery on exercise testing to predict high risk finding on single photon emission computed tomography myocardial perfusion imaging in men. Am J Cardiol 103(5): 611-614.
-
Johnson NP, Goldberger JJ (2012) Prognostic value of late heart rate recovery after treadmill exercise. Am J Cardiol 110(1): 45-49.
-
Lipinsky MJ, Vetrovee CW, Froelicher VF (2004) Importance of first two minutes of heart rate recovery after exercise treadmill testing in predicting mortality and the presence of coronary artery disease in men. Am J Cardiol 93(4): 445-449.
-
Antelmi I, De Paula RS, Shinzato AR, Peres CA, Mansur AJ, et al. (2004) Influence of age, gender, body mass index and functional capacity on heart rate variability in a cohort of subjects without heart disease. Am J Cardiol 93(3): 445-450.
-
Antelmi I, Chuang EY, Grupi CJ, Latorre Mdo R, Mansur AJ (2008) Heart rate recovery after treadmill electrocardiographic stress test and 24 hours heart rate variability in healthy individuals. Arq Bras Cardiol 90(6): 380-385.
-
Ashley EA, Myers J, Froelicher V (2000) Exercise testing in clinical medicine. Lancet 356(9241): 1592-1597.
-
Shetler K, Marcus R, Froelicher VF, Vora S , Kalisetti D, et al. (2001) Heart rate recovery: validation and methodology issues. J Am Coll Cardiol 38(7): 1980-1987.
-
Beckie TM, Beckstead JW, Kip KE, Fletcher G (2014) Improvement in heart rate recovery among women after cardiac rehabilitation completion. J Cardiovasc Nurs 29(1): 38-47.
-
Thomas GS, Wann LS, Ellestad MH (2018) Predicting prognosis with the exercise test. In: Thomas GS (Eds.), Ellestad’s Stress Testing. 6th (Edn.), Oxford, UK, 2018:228-267.
-
Messay D, Verma SK (2008) Comparison of cardiovascular response to exercise and recovery pattern in players. Journal of Exercise Science and Physiotherapy 4(1): 55- 65.
-
Lauer M, Froelicher ES, Williams M, Kligfield P (2005) Exercise testing in asymptomatic adults: a statement for professionals from the American Heart Association Council on clinical cardiology, subcommittee on Exercise Cardiac Rehabilitation and Prevention. Circulation 112(5): 771-776.
-
Imai K, Sato H, Hori M, Kusuoka H, Ozaki H, et al. (1994) Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J Am Coll Cardiol 24(6): 1529- 1535.
-
Adabag AS, Granditis GA, Prineas RJ, Crow RS, Bloomfield HE, et al. (2008) Relation of heart rate parameters during exercise test to sudden death and all-cause mortality in asymptomatic men. Am J Cardiol 101(10): 1427-1443.
-
Cole CR, Blackstone EH, Pashkow FJ, Snader CE, Lauer MS (1999) Heart rate recovery immediately after exercise as a predictor of mortality. New Eng J Med 341(18): 1351- 1357.
-
Thomas GS, Ellested MH (2018) Contraindications and safety for stress testing. In: Thomas GS (Eds.), Ellestad’s Stress Testing. 6th (Edn.), Oxford, UK, 2018: 71-81.
-
Sharma HB, Kailashivya J (2016) Gender difference in exercise capacity and the contribution of body composition and haemoglobin concentration: a study of young Indian hockey players. J clin Diagn Res 10(11): 9-13.
-
Chin CF, Messenger JC, Greenberg PS, Ellestad MH (1979) Chronotropic incompetence in exercise testing. Clin Cardiol 2(1): 12-18.
-
Gibbons RJ, Balady GJ, Bricker JT, Chaitman BR, Fletcher GF, et al. (2002) ACC/AHA 2002 guideline update for exercise testing: A report of the American College of Cardiology/American Heart Association Task Force on practice guideline committee on exercise testing. J Am Coll Cardiol 40(8): 1531-1540.
-
Mason RE, Likar I (1996) A new system of multiple lead exercise electrocardiography. Am Heart J 71(2): 196- 205.
-
Bruce R, Blackman J, Jones J, Strait J (1963) Exercise testing in adult normal subjects and cardiac patients. Pediatrics 32: 742-756.
-
Jain M, Nikonde C, Lin BA, Walker A, Wackers FJ (2011) 85% of maximal age predicted heart rate is not a valid end point for exercise treadmill testing. J Nucl Cardiol 18(6): 1026-1035.
-
Fletcher GF, Ades PA, Kligfield P, Arena R, Balady GJ, et al. (2013) Exercise standards for testing and training: a scientific statement from the American Heart Association. Circulation 128(8): 878-934.
-
Fox S III, Naughton JP, Haskell WL (1971) Physical activity and the prevention of coronary heart disease. Ann Clin Res 3(6): 404-432.
-
Student ‘T’ test - an overview.
-
Lohiri MK, Kannankeril PJ, Goldberger JJ (2008) Assessment of autonomic function in cardiovascular disease: physiological basis and prognostic implication. J Am Coll Cardiol 51(18): 1725-1735.
-
Tsuji H, Venditti FJ, Manders ES, Evans JC, Larson MG, et al. (1994) Reduced heart rate variability and mortality risk in elderly cohort: the Framingham Heart Study. Circulation 90(2): 878-883.
-
Sylvies FR, Ellestad MH (2018) Cardiovascular and pulmonary responses to exercise. In: Thomas GS (Eds.), Ellestad’s Stress Testing. 6th (Edn.), Oxford, UK, 2018: 375-412.
-
Adabag AS, Granditis GA, Prineas RJ, Crow RS, Bloomfield HE, et al. (2008) Relation of heart rate parameters during exercise test to sudden death and all-cause mortality in asymptomatic men. Am J Cardiol 101(10): 1437-1443.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study