Evaluation the Efficacy of Some Plant Extracts and Antibiotics on the Formation of Biofilm Bacterial Species Isolated From a Variety of Clinical Sources
The aim of this research was to shed light on isolation and identification of bacterial species from patients with different genders and age groups and determined the antimicrobial effects of various new plant-based extracts and antibiotics on the isolates. Disk diffusion assay was used to determine the susceptibility of bacterial isolates towards several antibiotics. The Minimum inhibitory concentration (MIC) and Minimum Bactericidal Concentration (MBC) for all extracts were conducted against every isolated species of bacteria in 96-well microtiter plates. The findings of this study and according to the VITIK2 data, among the 180 swaps and samples collected from patients, only 92 cases (51.11%) showed a positive bacterial culture which distributed as follows; 41 (44.56%) isolates matched with Staphylococcus aureus, 20 (21.73%) isolates matched with Escherichia coli, 14 isolates of Pseudomonas aeruginosa represent (15.21%), 11 isolates of Klebsiella pneumoniae which gave (11.95%) and only 6 isolates were correspond to Staphylococcus haemolyticus at (6.52%). The antibiotics findings of this study indicated variable resistance profiles for most of the isolates against the antibiotics used, however all isolates exhibited great sensitivity to the meropenem. Furthermore, testing findings for plant extracts revealed that MBC values ranged from 1.95 to 500 μg/mL, while MIC for 17 examined extracts ranged from 0.97 to 250 μg/mL. As a positive control, meropenem's MIC against all isolated species ranged from 3.9 μg/mL to 62.5 μg/mL, whereas its MBCs varied from 7.8 to 125 μg/mL. In light of this, this study is the first to demonstrate the effectiveness of novel plant extracts against virulent bacterial strains isolated from urine, burn, and wound infections. According to the outcomes of this study, the evaluated plant extracts are more effective in combating bacteria than the antibiotics that are used in the treatment regimen.
Introduction
Biofilm is a microbial community of microbes that bond to a surface and are surrounded in an extracellular polymeric substance (EPS) matrix [1]. These extracellular polymeric substances (EPS) give cells a layer of defence against various stresses and antibiotics, which can lead to major issues in both industrial and therapeutic settings [2]. Biofilm can be formed by about 40-80% of bacteria and it is generally considered to cause detrimental effects in several situations [3]. Formation of biofilms is a significant challenge for healthcare, medical, and food industries since they allow bacteria to stick to a range of surfaces, during a few minutes, that followed by mature biofilms developing within a few days or hours [4, 5]. Considering human health, biofilms on medical devices in hospitals and on patient’s tissues can result in persistent infections [6]. Formation of biofilms inside the processing facilities in food industries leading to food spoilage and endangering consumer’s health [7]. Although bacterial biofilm may have beneficial effects, in view of its serious impact on human health, scientists have mainly focused on control of harmful biofilms [8].
Plant extracts and products are a rich source of compounds that have numerous reported biological activities containing antibacterial, antifungal as well as anti-biofilm potential, hence this property turns them into an efficient resource to explore for the finding of beneficial and novel antimicrobial component with feasible new mechanisms of action [9, 10, 11]. Natural products from plants represent a precious source of anti-biofilm properties. Examples of this composition are styrylpyrones and quinic acid derivatives from the polar metabolites of Helichrysum italicum against Pseudomonas aeruginosa [12]. Epigallocatechin-3-gallate (EGCG) is a potent inhibitor of the formation of those biofilms that use amyloid fibres and pEtN-cellulose as main extracellular matrix components [13]. Based on the literature secondary metabolites of plants such as phenolic compounds not only have shown destructive activity on bacteria, but also has revealed anti-biofilm properties via affecting the bacterial regulatory mechanisms such as quorum-sensing (QS) or other global regulator systems [14]. Tannins (sometimes called tannic acid) as water-soluble polyphenols isolated from Eustigma oblongifolium inhibited biofilm formation by staphylococcus aureus independently of growth mechanisms [15]. In this article, I have reported plant’s extracts and antibiotics having anti-biofilm activity and evaluated them against various biofilm-producing bacterial strains.
Materials and Methods
Preparation of the Media
The preparation of all the media for culture was done in accordance with the manufacturing company’s guidelines, and they were autoclaved for 15 minutes at 121 °C to sterilize them.
Samples Collection
A total of 180 samples and swaps from patients of all ages and genders had been collected between October 2021 and June 2022. Overall, 180 samples were collected from different age groups and genders, with information about age and gender. The source of the clinical samples and swabs were from urine samples 120 cases (66.66%), wound (pus) swabs 40 cases (22.22%) and burns swaps 20 cases (11.11%). All of the samples and swabs were collected and sent to the lab in less than two hours. The kind of swabs can stop growing of bacteria for seventy-two hours. The collected specimens and samples have been streaked individually and directly onto solid medium that involved nutrient agar, blood agar, and MacConkey agar. Following a 24-hour incubation period at 37 °C, the petri dish plates were examined visually in order to look for any signs of bacterial growth.
Plant Extracts Preparation
The plant extracts were obtained from Tehran University of Medical Sciences, Tehran, Iran. The plant materials have been cleaned and then dried in the shade at room temperature. The maceration procedure with pure methanol was used to extract the powdered plant material (50g) 3 times in 48 hours (3 x 48hrs) at room temperature. A freeze dryer was used to lyophilize the extracts once the solvent had been extracted using a rotary evaporator. After that, the concentrated extracts were stored until analysis in opaque containers at 4° C in a dry, cool environment. In order to produce the extracts, 10 mg of extract powder were weighed, and 9 mL of deionized water and 1 mL of methanol were added as a co-solvent. This resulted in a final concentration of 1 mg/mL.
Identification of the Bacterial Isolates
Gram staining, biochemical characteristics, and colony morphology were used to identify the bacterial isolates. The biochemical tests that were employed included the methyl-red Voges Proskauer test, slide coagulase test, triple sugar iron test, oxidase, citrate utilisation, urease, sulphide, and indole motility tests. The VITKE 2 system was used to perform additional identification for bacterial isolates. A vacuum device automatically filled the card, sealed it, and put it into the VITEK 2 reader-incubator module (incubation temperature 35.5°C), where it was exposed to kinetic fluorescence measurements every 15 minutes. The ID- GPC database interpreted the results, and the results were obtained automatically.
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing was performed by disc diffusion method for all isolates. This test was performed as (Kirby-Bauer disk susceptibility test) according to Bauer A, et al. and as described by Standards NCoCL. Briefly, between three and five carefully chosen colonies of bacteria were removed from a pure culture and placed in a tube holding five millilitres of nutrient broth. The colonies of bacteria were gently mixed to form a homogenous suspension, which was then incubated at 37 °C until the suspension’s turbidity was adjusted to a McFarland 0.5. The remaining suspension was gently rubbed off with a sterile cotton swab by rotating it against the tubes inside surface. Next, the whole surface of Mullen Hinton agar was covered with the bacteria using the swab to spread them equally.
A set of antibiotic discs was placed on the surface of the Muller-Hinton plate after the inoculated plates were allowed to dry for 5 minutes at room temperature. The plates were incubated for 24 hours aerobically at 37ºC. From the backside of the plates, the diameter of the inhibition zone surrounding each disc was measured with a ruler. The results were compared to a standard inhibitory diameter for antibiotics to establish if the organism was susceptible (S), intermediate (moderate resistance) (MR), or resistant (R) to the antibacterial drugs evaluated.
Determining the Minimum Inhibitory Concentration (MIC)
The MIC for each extract was measured in 96-well microtiter plates against each isolated bacterial species using the previously published procedure by (42) in order to assess the antibacterial activity of the plant extracts on the formation of biofilm bacterial species isolated from various clinical sources. The Muller-Hinton Broth (MHB) growth method was used to create the test organisms, and then the suspensions of bacteria were adjusted to 0.5 McFarland turbidity standards (108 CFU/mL). The entire procedure took six hours to complete. All extracts had their concentrations diluted to two-fold, ranging from 1000 to 0.48 μg/mL (final volume 80 μL), with a DMSO content of ≤1%. The next step involved filling microtiter plates with 20 μL of bacterial suspensions and 100 μL of MHB. The plates were then incubated for 24 hours at 37°C. After the incubation period, microtiter plates were inspected at 620 nm using a spectrophotometer. Meropenem, a common antibiotic, was used as a positive control. MHB + DMSO were a negative control as well. The minimum inhibitory concentration (MIC) of a plant extract was determined by showing total inhibition of observable growth.
Determining the Minimum Bactericidal Concentration (MBC)
The MIC test was followed by an MBC measurement. After an 18–24-hour period of incubation at 37°C, 5 μL of the sample was placed onto MHA plates and added to the wells that showed no apparent growth. The concentration at which there was the least amount of bacterial growth or colony was then identified as the MBC.
Results
Isolation of Bacterial Species from Different Clinical Samples
Out of the total cases, there were 92 cases (51.11%) positive for bacterial infection with different genders and age groups and 88 cases (48.88%) were negative for bacterial growth as shown in Figure 1.
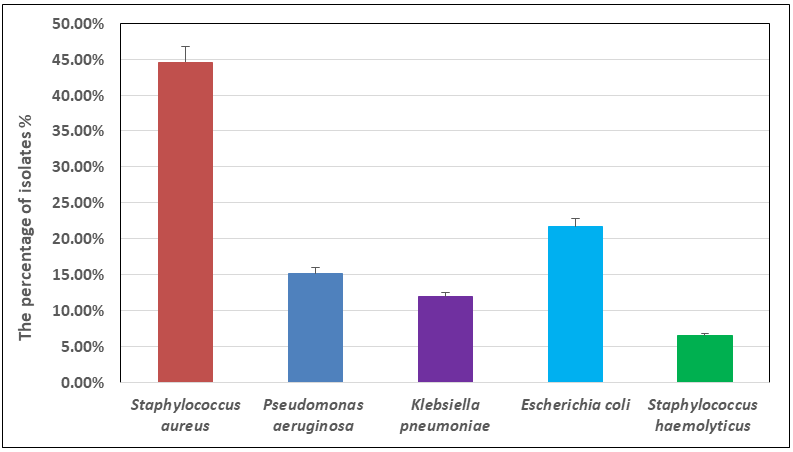
Among the 180 swaps and samples collected from patients of various age groups and genders, only 92 cases (51.11%) showed a positive bacterial culture which distributed as follows; 41 (44.56%) isolates matched with Staphylococcus aureus, 20 (21.73%) isolates matched with Escherichia coli, 14 isolates of Pseudomonas aeruginosa represent (15.21%), 11 isolates of Klebsiella pneumoniae which gave (11.95%) and only 6 isolates were correspond to Staphylococcus haemolyticus at (6.52%) as illustrated in Figure 2.
Evaluation of Antimicrobial Susceptibility
Table 1 presents the antimicrobial screening findings, there were 92 bacterial isolates tested for their susceptibility to 20 different antibiotics. The findings indicate variable resistance profiles for most of the isolates against the antibiotics used. More interesting findings that all isolates exhibited great sensitivity to the meropenem.
| Antibiotics | Bacterial species | |||||
|---|---|---|---|---|---|---|
| Name | Abbreviation | S. aureus | P. aeruginosa | K. pneumoniae | S. haemolyticus | E. coli |
| Meropenem | MER | S | S | S | S | S |
| Ampicillin | AMP | R | R | R | R | R |
| Cephalothin | CEP | R | R | R | R | R |
| Chloramphenicol | CHL | MR | MR | MR | MR | MR |
| Carbenicillin | CAR | R | R | R | R | R |
| Amoxicillin | AMX | R | R | R | R | R |
| Clindamycin | CLN | MR | MR | MR | MR | MR |
| Penicillin | PEN | R | R | R | R | R |
| Aztreonam | ATM | R | R | R | R | R |
| Tobramycin | TOB | R | R | R | R | R |
| Ceftazidime | CAZ | R | R | R | R | R |
| Tetracycline | TEY | MR | MR | MR | MR | MR |
| Neomycin | NYN | R | R | R | R | R |
| Bacitracin | BCN | R | R | R | R | R |
| Erythromycin | ERT | R | R | R | R | R |
| Metronidazole | MET | MR | MR | MR | MR | MR |
| Trimethoprim | TMP | R | R | R | R | R |
| Lincomycin | LIN | R | R | R | R | R |
| Oxacillin | OXA | R | R | R | R | R |
| Cloxacillin | CLX | R | R | R | R | R |
Table 1: The antibiotics sensitivity findings against several isolates obtained from different clinical samples. Sensitive = S; M
Determination of MIC and MBC
The antibacterial activity of the plant extract was assessed using the MIC and MBC values against isolated biofilm bacterium species. Since meropenem is frequently used to treat infections brought on by the examined bacteria, it was chosen as a positive control. The majority of plant extracts investigated in this study had a broad range of inhibitory activity and shown efficacy against both isolated Gram-positive and Gram-negative bacteria. When it comes to antibacterial agents, the minimum concentration (MIC) that greatly inhibits growth and the lowest concentration (MBC) that results in bacterial death are two distinct outcomes. The MIC and MBC values are shown in Table 2. The range of MBC values was 1.95 to 500 µg/mL, while the MIC concentrations for all examined extracts were 0.97 to 250 µg/mL. Utilising Meropenem as a positive control, the MIC ranged from 3.9 µg/mL to 62.5 µg/mL, whereas the MBCs varied from 7.8 to 125 µg/mL against all isolated species. Proskia extract exhibited significant antibacterial activity against each assessed species of bacteria, as evidenced by MIC values that varied from 0.97 µg/mL to 1.95 µg/mL and MBC that ranged from 1.95 µg/mL to 7.8 µg/mL.
| Extracts | Bacterial Species(The MIC and MBC are reported in µg/mL) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Name | S. aureus | P. aeruginosa | K. pneumoniae | S. haemolyticus | E. coli | |||||
| MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | MIC | MBC | |
| Ferula asafoetida | 3.9 | 7.8 | 7.8 | 31.2 | 3.9 | 15.6 | 1.95 | 7.8 | 3.9 | 15.6 |
| Zumeria majda | 7.8 | 15.6 | 15.6 | 31.2 | 7.8 | 62.5 | 7.8 | 31.5 | 15.6 | 31.5 |
| Thymus migricus | 15.6 | 31.2 | 31.2 | 62.5 | 15.6 | 31.2 | 3.9 | 15.6 | 7.8 | 62.5 |
| Artemisia santolina | 7.8 | 62.5 | 15.6 | 125 | 7.8 | 31.2 | 15.6 | 62.5 | 31.2 | 62.5 |
| Sargassum | 15.6 | 31.2 | 31.2 | 62.5 | 31.2 | 125 | 31.2 | 62.5 | 15.6 | 125 |
| Proskia | 1.95 | 7.8 | 3.9 | 7.8 | 1.95 | 3.9 | 0.97 | 1.95 | 1.95 | 3.9 |
| Roots of Echinacea angustifolia | 31.2 | 62.5 | 15.6 | 62.5 | 7.8 | 62.5 | 15.6 | 31.2 | 31.2 | 62.5 |
| Echinophora platyloba | 15.6 | 125 | 31.2 | 250 | 15.6 | 125 | 31.2 | 62.5 | 7.8 | 125 |
| Pimpinella tragiodes | 125 | 500 | 250 | 500 | 62.5 | 250 | 31.2 | 125 | 62.2 | 250 |
| Phlomis bruguieri | 62.5 | 125 | 31.2 | 250 | 15.6 | 62.5 | 62.5 | 125 | 125 | 250 |
| Phlomis kurdica | 31.2 | 250 | 125 | 500 | 62.5 | 250 | 31.2 | 125 | 250 | 500 |
| Phlomis olivieri | 62.5 | 125 | 31.2 | 250 | 125 | 500 | 15.6 | 62.5 | 125 | 250 |
| Satureja khuzestanica | 7.8 | 15.6 | 7.8 | 31.2 | 15.6 | 31.2 | 3.9 | 15.6 | 7.8 | 62.5 |
| Satureja spicigera | 15.6 | 62.5 | 31.2 | 125 | 7.8 | 62.5 | 15.6 | 31.2 | 31.2 | 125 |
| Polysaccharide extract of pomegranate peel | 7.8 | 31.2 | 15.6 | 62.5 | 7.8 | 15.6 | 3.9 | 15.6 | 15.6 | 31.2 |
| Trametes hirsuta | 15.6 | 31.2 | 31.2 | 62.5 | 7.8 | 15.6 | 3.9 | 31.2 | 31.2 | 62.5 |
| Cicer arietinum proteins | 15.6 | 62.5 | 15.6 | 31.2 | 31.2 | 62.5 | 31.2 | 125 | 62.5 | 125 |
| Meropenem as positive control | 7.8 | 15.6 | 62.5 | 125 | 15.6 | 31.2 | 3.9 | 7.8 | 7.8 | 31.2 |
Table 2: The efficacy of a variety of plant extracts to inhibit the growth of multiple isolates obtained from clinical samples.
Discussion
In the current investigation, 180 swaps and samples were obtained from patients of both genders and with different ages. The results of isolation and identification revealed that only 92 cases (51.11%) had a positive bacterial culture. There were several bacterial species found, with the highest percentage (44.56%) related to Staphylococcus aureus, the next causative agent was Escherichia coli at (21.73%) Pseudomonas aeruginosa represented (15.21%), Klebsiella pneumoniae displayed (11.95%), and the lowest prevalence was related to Staphylococcus haemolyticus at (6.52%). The isolation results are consistent with previous published studies [16, 17, 18, 19, 20, 21, 22, 23], that found Staphylococcus aureus, Pseudomonas aeruginosa and Escherichia coli to be the most common bacteria isolated from urinary tract, burn and wound infections.
The majority of bacterial isolates showed higher resistance patterns, while some isolates demonstrated intermediate resistance, and all isolates were found to be meropenem sensitive. These findings in agreement with other published studies [24, 25, 26, 27] which confirmed that various levels of antibiotic resistance against the isolated bacterial species from urinary tract, burn, and wound infections. Meropenem is a carbapenem antibiotic with a broad spectrum. It works against both Gram-positive and Gram-negative bacteria. Meropenem kills bacteria by binding to penicillin-binding proteins (PBPs) in bacterial cell walls and disrupting the peptidoglycan cross-linking process that is involved in cell wall production which leads to cell death [28, 29, 30].
The beta-lactam antibiotics examined in this study, including ampicillin, amoxicillin, carbenicillin, penicillin, oxacillin, and cloxacillin, exhibited no activity against all tested bacterial species. These findings are in line with an earlier published studies [24, 31, 32] that found isolated Staphylococcus aureus, Pseudomonas aeruginosa, Escherichia coli and Klebsiella spp isolated from various sources to be resistant to oxacillin, amoxycillin, pencillin G, ampicillin, tetracycline and cloxacillin. PBPs are the principal targets of β-lactam agents. The β-lactam ring is thought to resemble the D-alanyl D-alanine component of the peptide chain that is ordinarily bound by PBP. The PBP interacts with the β-lactam ring and unavailable for peptidoglycan production. The bacterium is lysed when the peptidoglycan layer is disrupted [33].
The chloramphenicol, clindamycin, tetracycline, and metronidazole, demonstrated moderate activity against all strains that were evaluated. An in vitro study was conducted to test the efficacy of chloramphenicol and tetracycline on the biofilm formation of five isolates, including Klebsiella sp., Pseudomonas aeruginosa, Achromobacter sp., Klebsiella pneumoniae, and Bacillus pumilis. It was observed that the biofilm formation of all strains was affected in the existence of tetracycline or chloramphenicol [34]. The findings that have been reported are comparable with those of the current study that I am undertaking. Other antibiotics examined in this study, including cephalothin, aztreonam, tobramycin, ceftazidime, neomycin, bacitracin, erythromycin, trimethoprim, and lincomycin, were shown to be ineffective against all isolates. The obtained results are consistent with previous studies [19, 35] that found the stated antibiotics exhibited a resistance pattern towards Gram positive and Gram negative bacterial species. The rising resistance rates in this study are highly concerning, and they may be a result of patients and health professionals using and abusing prescribed medication extensively, as well as from medical doctors prescribing large amounts of antibiotics [36]. It is important to analyse the molecular basis of developing resistance in order to create new antibiotics which target specific resistance mechanisms in order to avoid and combat antibiotic resistance.
Remarkably interesting results of assessing the antibacterial effects of plant extracts on the inhibition and eradication of bacterial isolates obtained from various clinical sources. The current study data revealed that the MIC and MBC at lower concentrations for the antibacterial of most tested plant extracts on the isolates in comparison with the antibiotic meropenem that has been used as positive control. Among 17 different plant extracts, the proskia extract demonstrated excellent antibacterial activity against all investigated bacterial species, with MIC ranged from 0.97 to 3.9 µg/mL and MBC varied from 1.95 to 7.8 µg/mL. At various concentrations, the other examined plant extracts inhibited and killed all of the tested bacterial species, with MIC varied from 1.95 to 250 µg/mL and MBC ranged from 7.8 to 500 µg/mL. The findings are comparable to those of Rahman and co-workers [37], who evaluated the antibacterial activity of ferula assafoetida oil against Gram positive and Gram negative bacteria. Ferula assafoetida oil showed activity at 50 µg/mL and was elevated to 200 µg/mL against Vibrio cholerae.
The results are in line with earlier findings from Shafiei Z, et al. [38], who examined the plant extracts mixture and its individual component plant extracts (Psidium sp., Mangifera sp., Mentha sp.) on the production of biofilms containing Streptococcus sanguinis and Streptococcus mutans. According to the authors of the cited study, the plant extract mixture had a synergistic impact and displayed the lowest MIC for S. sanguinis (3.81mg/mL) and S. mutans (1.91mg/mL) when compared to each of its individual constituent plants. The MBC was demonstrated against S. sanguinis and S. mutans, respectively, by the mixture of Psidium sp. (15.24 mg/mL) and plant extracts and Psidium sp. (30.48 mg/mL). Additionally, Azizi A, et al. [39] looked into the effect of zingiber officinale extract on the development of S. mutans and S. sanguinis, and the results showed that the MIC values for these two strains were (0.02 mg/mL) for S. mutans and (0.3 mg/mL), respectively. The MBC for S. mutans was (0.04mg/mL) and for S. sanguinis was (0.6mg/mL), and these data are in accord with those of the present study [40, 41, 42].
Conclusion
According to the findings of this investigation, Staphylococcus aureus demonstrated the highest proportion of isolated bacteria from virous clinical sources in this research which represented (44.56%), whereas Staphylococcus haemolyticus have had lowest percentage at (6.52%). Most of the isolates had different resistance patterns to the antibiotics utilised, but that all isolates had extremely high meropenem sensitivity. The proskia extract exhibited significant antibacterial effect against all tested bacterial species, with MIC ranged from 0.97 to 3.9 µg/mL and MBCs varied from 1.95 to 7.8 µg/mL. The MBC values for the other plant extracts tend to range from 1.95 to 500 µg/mL, while the MIC values were from 0.97 to 250 µg/ mL. To that end, this is the first study to show that new plant extracts have efficacy against virous bacterial strains isolated from urine, burn, and wound infections. Based on the current study findings, the antibacterial efficiency of the assessed plant extracts is superior to the antibiotics utilised in the treatment regimen.
Declarations
Competing interests: The author declare that they have no competing interests Funding: This research received no external funding.
Acknowledgement
The author is grateful to University of Fallujah, College of Veterinary Medicine in Iraq – Al Anbar. Also, I would like to thank the staff who working in Al-Ramadi teaching hospital at Al-Anbar Province for their help in collecting the samples.
References
-
Song X, Xia YX, He ZD, Zhang HJ (2018) A review of natural products with anti-biofilm activity. Current Organic Chemistry 22(8): 789-817.
-
Høiby N, Bjarnsholt T, Givskov M, Molin S, Ciofu O (2010) Antibiotic resistance of bacterial biofilms. Int J Antimicrob Agents 35(4): 322-332.
-
Flemming HC, Wuertz S (2019) Bacteria and archaea on Earth and their abundance in biofilms. Nat Rev Microbiol 17(4): 247-260.
-
Hall-Stoodley L, Costerton JW, Stoodley P (2004) Bacterial biofilms: from the natural environment to infectious diseases. Nat Rev Microbiol 2(2): 95-108.
-
Carrascosa C, Raheem D, Ramos F, Saraiva A, Raposo A (2021) Microbial biofilms in the food industry—A comprehensive review. Int J Environ Res Public Health 18(4): 2014.
-
Percival SL, Suleman L, Vuotto C, Donelli G (2015) Healthcare-associated infections, medical devices and biofilms: risk, tolerance and control. J Med Microbiol 64(Pt 4): 323-334.
-
Galie S, García-Gutiérrez C, Miguélez EM, Villar CJ, Lombó F (2018) Biofilms in the food industry: health aspects and control methods. Front Microbiol 9: 898.
-
Muhammad MH, Idris AL, Fan X, Guo Y, Yu Y, et al. (2020) Beyond risk: bacterial biofilms and their regulating approaches. Front Microbiol 11: 928.
-
Romulo A, Zuhud EAM, Rondevaldova J, Kokoska L (2018) Screening of in vitro antimicrobial activity of plants used in traditional Indonesian medicine. Pharm Biol 56(1): 287-293.
-
Ribeiro ICDO, Mariano EGA, Careli RT, Morais-Costa F, Sant’Anna FMD, et al. (2018) Plants of the Cerrado with antimicrobial effects against Staphylococcus spp. and Escherichia coli from cattle. BMC Vet Res 14(1): 32.
-
Ogbole O, Segun PA, Fasinu PS (2018) Antimicrobial and antiprotozoal activities of twenty-four Nigerian medicinal plant extracts. South African Journal of Botany 117: 240-246.
-
D’Abrosca B, Buommino E, D’Angelo G, Coretti L, Scognamiglio M, et al. (2013) Spectroscopic identification and anti-biofilm properties of polar metabolites from the medicinal plant Helichrysum italicum against Pseudomonas aeruginosa. Bioorg Med Chem 21(22): 7038-7046.
-
Hengge R (2019) Targeting bacterial biofilms by the green tea polyphenol EGCG. Molecules 24(13): 2403.
-
Silva LN, Zimmer KR, Macedo AJ, Trentin DS (2016) Plant natural products targeting bacterial virulence factors. Chem Rev 116(16): 9162-9236.
-
Lin MH, Chang FR, Hua MY, Wu YC, Liu ST (2011) Inhibitory effects of 1, 2, 3, 4, 6-penta-O-galloyl-β-D- glucopyranose on biofilm formation by Staphylococcus aureus. Antimicrob Agents Chemother 55(3): 1021- 1027.
-
Kassam NA, Damian DJ, Kajeguka D, Nyombi B, Kibiki GS (2017) Spectrum and antibiogram of bacteria isolated from patients presenting with infected wounds in a Tertiary Hospital, northern Tanzania. BMC Res Notes 10(1): 757.
-
Bitew A, Molalign T, Chanie M (2017) Species distribution and antibiotic susceptibility profile of bacterial uropathogens among patients complaining urinary tract infections. BMC Infect Dis 17(1): 654.
-
Upreti N, Rayamajhee B, Sherchan SP, Choudhari MK, Banjara MR (2018) Prevalence of methicillin resistant Staphylococcus aureus, multidrug resistant and extended spectrum β-lactamase producing gram negative bacilli causing wound infections at a tertiary care hospital of Nepal. Antimicrob Resist Infect Control 7: 121.
-
Al-Naqshbandi AA, Chawsheen MA, Abdulqader HH (2019) Prevalence and antimicrobial susceptibility of bacterial pathogens isolated from urine specimens received in rizgary hospital—Erbil. J Infect Public Health 12(3): 330-336.
-
Puca V, Marulli RZ, Grande R, Vitale I, Niro A, et al. (2021) Microbial species isolated from infected wounds and antimicrobial resistance analysis: Data emerging from a three-years retrospective study. Antibiotics (Basel) 10(10): 1162.
-
Shahab NW, Ali CIAD, Salih SM (2017) Isolation and Identification of bacteria causing urinary tract infections in children in Kirkuk city. Tikrit Journal of Pure Science 22(2): 8-12.
-
Saeed A, Hamid SA, Bayoumi M, Shanan S, Alouffi S, et al. (2017) Elevated antibiotic resistance of Sudanese urinary tract infection bacteria. EXCLI J 16: 1073-1080.
-
Latifi NA, Karimi H (2017) Correlation of occurrence of infection in burn patients. Ann Burns Fire Disasters 30(3): 172-176.
-
Mohammed A, Seid ME, Gebrecherkos T, Tiruneh M, Moges F (2017) Bacterial isolates and their antimicrobial susceptibility patterns of wound infections among inpatients and outpatients attending the University of Gondar Referral Hospital, Northwest Ethiopia. Int J Microbiol 2017: 8953829.
-
Mahdi B, Khudhur HB, Abdul-Hussein MM (2020) Bacterial isolates of urine and their susceptibility to antimicrobials. Open Access Macedonian Journal of Medical Sciences 8(A): 84-88.
-
Alwan MJ, Lafta IJ, Hamzah AM (2011) Bacterial isolation from burn wound infections and studying their antimicrobial susceptibility. Kufa J Vet Med Sci 2(1).
-
Uddin MN, Jabeen B, khan Q, Naeem S, Khan W (2018) Characterization of isolated bacteria from burn patients and its susceptibility against different antibiotics in district Swat. PAB 7(1): 121-132.
-
Visser MR, Hoepelman IM, Beumer H, Rozenberg-Arska M, Verhoef J (1989) Comparative in vitro antibacterial activity of the new carbapenem meropenem (SM-7338). Eur J Clin Microbiol Infect Dis 8(12): 1061-1064.
-
Hecker SJ, Reddy KR, Totrov M, Hirst GC, Lomovskaya O, et al. (2015) Discovery of a cyclic boronic acid β-lactamase inhibitor (RPX7009) with utility vs class A serine carbapenemases. J Med Chem 58(9): 3682-3692.
-
Lomovskaya O, Sun D, Rubio-Aparicio D, Nelson K, Tsivkovski R, et al. (2017) Vaborbactam: spectrum of beta-lactamase inhibition and impact of resistance mechanisms on activity in Enterobacteriaceae. Antimicrob Agents Chemother 61(11): e01443-e01517.
-
Muluye D, Wondimeneh Y, Ferede G, Nega T, Adane K, et al. (2014) Bacterial isolates and their antibiotic susceptibility patterns among patients with pus and/or wound discharge at Gondar university hospital. BMC Res Notes 7: 649.
-
Ameer FA (2013) Effect of some antibiotics on aerobic pathogenic bacteria in operation theaters in AL- Manathera general hospital: A comparative study. Kufa Med J 16(2): 24-29.
-
Džidić S, Šušković J, Kos B (2008) Antibiotic resistance mechanisms in bacteria: biochemical and genetic aspects. Food Technology & Biotechnology 46(1): 11-21.
-
Liaqat I, Sumbal F, Sabri AN (2009) Tetracycline and chloramphenicol efficiency against selected biofilm forming bacteria. Curr Microbiol 59(2): 212-220.
-
Hewitt JS, Allbaugh RA, Kenne DE, Sebbag L (2020) Prevalence and antibiotic susceptibility of bacterial isolates from dogs with ulcerative keratitis in Midwestern United States. Front Vet Sci 7: 583965.
-
Hallsworth M, Chadborn T, Sallis A, Sanders M, Berry D, et al. (2016) Provision of social norm feedback to high prescribers of antibiotics in general practice: a pragmatic national randomised controlled trial. Lancet 387(10029): 1743-1752.
-
Rahman MU, Gul S, Odhano EA (2008) Antimicrobial activities of Ferula assafoetida oil against gram positive and gram negative bacteria. Am-Euras J Agric Environ Sci 4(2): 203-206.
-
Shafiei Z, Rahim ZHA, Philip K, Thurairajah N (2016) Antibacterial and anti-adherence effects of a plant extract mixture (PEM) and its individual constituent extracts (Psidium sp., Mangifera sp., and Mentha sp.) on single-and dual-species biofilms. Peer J 4: e2519.
-
Azizi A, Aghayan S, Zaker S, Shakeri M, Entezari N, et al. (2015) In vitro effect of zingiber officinale extract on growth of Streptococcus mutans and Streptococcus sanguinis. Int J Dent 2015:489842.
-
Bauer AW, Kirby WM, Sherris JC, Turck M (1966) Antibiotic susceptibility testing by a standardized single disk method. Am J Clin Pathol 45(4): 493-496.
-
Standards NCoCL (2002) M100: Performance Standards for Antimicrobial Susceptibility Testing. 30th(Ed.), Clinical Laboratory Standards Institue 40(1): 1-13.
-
Patel JB, Cockerill F, Bradford PA (2015) Performance standards for antimicrobial susceptibility testing: twenty-fifth informational supplement.
- Antifungal Activity of New Acetophenone Derivatives
- Interconnected Microbiomes Human Health Within an Environmental Framework
- Silkworm-Based Vaccine Production for H5N1: A One Health Approach to Pandemic Preparedness
- Microbial Diversity and Lipolytic Activity of Bacteria and Fungi from Oil-Contaminated Sites in Makurdi Metroplois
- Antibiotic Resistance Profile of Bacteria Isolated at the Central Laboratory of the National Hospital Center of Nouakchott
- Epidemiology and Sensitivity to Antibiotics of Germs Isolated from Blood Cultures in the Laboratory of the National Hospital Center of Nouakchott-Mauritania