Gender-Specific Association of Oxidative Stress with Cardiovascular Risk Factors in Diabetic Patients of Central Punjab, Pakistan
Background: The present study aims to elucidate the gender-based association of oxidative- stress with cardiovascular risk factors in type II diabetes mellitus in the people of central Punjab, Pakistan. Methods: This study (case-control) was conducted on 200 subjects (100males and 100 females). Males and females; were categorized into control and diabetics. Each individual was subjected to clinical examination with a detailed history and fasting serum was collected to estimate total cholesterol (TC), triglycerides (TG), high- density lipoprotein-cholesterol (HDL-C), lowdensity lipoprotein-cholesterol (LDL-C), and oxidative stress markers (superoxide dismutase; SOD, reduced glutathione; GSH, malondialdehyde; MDA, catalase; CAT and nitric oxide; NO). Results: Male diabetics showed increased TC, TG, and LDL –C (P=0.001) with the reduction in HDL-C (p=0.000) compared to non-diabetic male subjects. Similarly, we found a marked increase in TC, TG, LDL-C (p=0.001) with the reduction in HDL-C (p=0.045) in females diabetics compared to non-diabetic female controls. Moreover, female diabetics were found to have augmented levels of TC, LDL-C (p=0.045), and TGs (p=0.001) than male diabetics. In addition to this, low levels of SOD, GSH, CAT, and NO (p= 0.001) in diabetic males and females was observed. However, MDA levels were found to be insignificant when compared with male diabetics with non-diabetic’s males. And, the increased MDA (p= 0.001) levels were found when diabetic females compared to non-diabetic females. When diabetic females compared to diabetic males, lower SOD (p=0.001) and GSH (p= 0.05) levels were seen with the increase in MDA levels (p=0.05). However, insignificant CAT and NOS levels were found when compared to diabetic males with diabetic females. Conclusion: It is concluded that women are more likely to develop cardiovascular complications than men and therefore the current study holds the evidence to put forward new insights towards the synthesis of more specific therapeutic targets.
Iffat Ara*, Ayesha Siddiqa and Amna Khatoon
Introduction
Diabetes mellitus is the most prevalent disease worldwide. The percentage of the chances of diabetes increases with age and initially, the prevalence has been recorded 5% worldwide which increases up to 20% in individuals of 80 years or above [1, 2]. This is due to the increasing level of fasting and postprandial glucose with age. These ratios indicate the link between the altered peripheral or hepatic insulin sensitivity and changes in the function of pancreatic insulin-producing cells. Type 2 diabetes mellitus is the most reported form of diabetes, which accounts for 85 to 90% of the total cases and is common among adults [2, 3].
Depending on the gender differences, the prevalence of type 2 diabetes mellitus is lower in women than in men [3, 4]. When the women reach menopause the risk of type 2 diabetes mellitus exceeds from 6 to 20%. Type 2 diabetes mellitus is caused by the combination of insulin resistance and the loss of the ability of pancreatic insulin-producing cells to produce insulin. In- vivo studies reported the strong influence of estradiol on glucose and insulin metabolism including the increased capacity of pancreatic insulin-producing cells, improvement in insulin sensitivity, hyperinsulinemia, pancreatic cell apoptosis, improvement in the lipid effect induced by insulin, and reduction in obesity [2, 5].
The stress-induced by the combination of high fat and high carbohydrate diet increases oxidative stress along with a spike in lipid peroxidation products, protein carbonylation, reduction in the antioxidant potential of the body, and low glutathione levels. These types of alterations have become the cause of obesity, cancer, diabetes, and cardiovascular diseases (CVDs). Atherosclerosis is the main risk factor of most of the diseases related to the heart. And oxidative stress and inflammation are responsible for atherosclerosis [6, 7].
At present, four diseases have become the cause of worldwide fatality and mortality including, cardiovascular diseases, Diabetes mellitus, Cancer, and Respiratory syndromes. But cardiovascular diseases are the leading cause of death [8, 9]. Oxidative stress plays a vital role in the development of CVDs. Prevalence can be seen in gender differences in the case of CVDs, therefore, there is a need to study the association between different genders and oxidative stress and the involvement of those factors that augment CVD risks.
Oxidative stress was higher reported in male rats than in female rats. In contrast, another study exhibited a higher incidence of biomarkers of oxidative stress in young males than in the females of a similar age group. It was also reported that the formation of reactive oxygen species was recorded more in men rather than women. There is a strong research- based analysis that indicates the greater antioxidant ability in women than in men. Many of the studies supporting the incidence of oxidative stress in women and men where females are less vulnerable to oxidative stress [2, 10, 11].
It is evident that the risk of atherosclerosis is lower in young females and the risk increases after menopause. But in men, the risk of heart diseases exceeds rapidly. For taking control of the increasing mortality rates due to heart diseases, it is very important to understand the pathogenesis of atherosclerosis and concerning gender differences [12]. Type 2 diabetes mellitus increases the risk of cardiovascular diseases more in women than in men. The research suggested that women have 27% more risk of stroke and 44% increased relative risk of cardiovascular diseases. The increased risk factor of diabetes and CVDs in women is related to more weight gain among females than in males. Thus, having a higher BMI which becomes the cause of diabetes [6, 13]. Therefore, depending on the medical conditions the differences in genders play a significant role when it comes to the selection of appropriate treatment and therapies.
The present study aims to evaluate the gender-related differences in oxidative stress which become the cause of developing cardiac risk factors in the presence of diabetes mellitus. Although not much research has been done in this area. Here we further analyze the linkage between oxidative stress in diabetes and gender differences in the development of cardiovascular diseases.
Material and Methods
Place of work
The present study was a case-control study, carried out from the year 2017-2018 in the department of Biochemistry, Minhaj University, Lahore, and approved by the ethical committee of Minhaj University, Lahore.
Subjects
The subjects in the present study included males (n= 100) and females (n=100), were taken written informed consent. Males and females both were categorized into control, n=30, and diabetics n=70, aged between 45 to 60 years. Each individual was subjected to written informed consent. Diabetic men and women who have not any other health complications and free from any type of medications and met the current WHO diagnostic criteria for diabetes i.e fasting plasma glucose level ≥ 7mmol/l (126mg/dl) or 2 hours plasma glucose ≥ 11mmol/l (200mg/dl) were included in the present study. And, individuals with HbA1c greater than 6.2% were considered.
Methods
Venous blood sampling was performed obtaining 10ml of blood by venipuncture in a vial containing no additives after overnight 12 hours fast. The serum was extracted from blood samples by centrifuging blood at 3000rpm for 15 minutes. The serum was preserved at --20°C for further analysis of lipid profile (cardiovascular markers) and antioxidants measurement.
Estimation of lipid profile parameters
Cardiovascular markers i-e serum TC, HDL-C, TG, and LDL-C were determined using a commercial assay kit (Randox® kit, Randox Laboratories, United Kingdom). LDL-C =Total cholesterol - Triglycerides - HDL-C
Estimation of Superoxide Dismutase Activity
SOD assay refers to the method established by Kakkar, et al. 1984. 0.5ml serum with 0.5ml trichloroacetic acid [ TCA,10%) was centrifuged at 13000 pm for 10minutes. After collecting the supernatant [ 15µl) into a separate tube, 120µl sodium pyrophosphate buffer [ pH 8.3, 0.052M), 12 µl phenazine methosulphate [ 186µM), and 36µl nitroblue tetrazolium [ 300µM) was added. To start the reaction, 24ul of NADH solution [ 780µM) was added and the reaction mixture was allowed to incubate at 37°C for 1.5 minutes. After incubation for 90sec, the reaction was terminated by adding 12ul of glacial acetic acid. To the mixture 400ul of n-butanol was added and the mixture was stirred vigorously. And, following incubation for ten minutes, the mixture was centrifuged at 2000rpm for 5 minutes at 25°C. The upper butanol layer was taken out and the color intensity of the chromogen extract in the n-butanol was measured at 560nm by spectrophotometer [14].
Estimation of Reduced Glutathione
Glutathione estimation employed the method of Beutler, et al., 1963. 0.5 ml TCA [ 10%) was added to 0.5ml serum and centrifuged for ten minutes. To the 40µl of supernatant, 150µl of disodium phosphate buffer [ 0.03M, pH=7.4) was added. Then, 25µl of 0.001M DTNB [ 5,5’-dithiobis [ 2-nitrobenzoic acid)/ Ellman’s Reagent, freshly prepared, dissolved in 1% sodium citrate) solution was added to the reaction mixture. The reduction of DTNB with GSH produced a yellow complex that was measured by a spectrophotometer at 412nm [15].
Estimation of Catalase
Catalase was estimated according to the method of Sinha, et al., 1972. 360µl phosphate buffer [ 10mM, pH 7.0) was added in 40 µl serum and allowed to centrifuge at 13000 rpm for 10 minutes at room temperature. 21µl of supernatant mixed with 180µl of phosphate buffer [10mM, pH 7.0). Afterward, 75 µl of 0.2M hydrogen peroxide [ freshly prepared) was added to initiate the reaction. Then 360µl of potassium dichromate acetic acid reagent was added to the reaction composite and was incubated for ten minutes in boiling water. Then allowed to stand for cooling and optical density was taken at 530nm [16].
Estimation of Malondialdehyde
Estimation of malondialdehyde refers to the method of Ohkawa, et al., 1979. For this, 40µl serum was mixed with 360 µl phosphate buffers [10mM, pH 7.4). The mixture was centrifuged at 13000 rpm. for 10minutes at room temperature. 15µl of supernatant was mixed with 15µl SDS [ 8.1%), 96ul TBA [ 0.8%), 96ul acetic acid [ 20%), and 18ul distilled water. It was kept at 90°C for 60 minutes. Afterward, 60ul distilled water and 300ul n-butanol pyridine mixture [ 15:1) were added, and the mixture was stirred violently and centrifuged at 4000 rpm at 25°C for 10min. The upper butanol layer was separated, and absorbance was taken at 532nm [17].
Determination of Endothelial Nitric Oxide Synthase (NOS) Activity
This estimation is based on the conversion of L-arginine to L-citrulline and nitric oxide by nitric oxide synthase and then Nitric oxide was measured according to the method of Cortas, et al.,1990. For this, 100µl of blood was added into an incubation mixture containing 50 µl [50mM Tris- hydro chloric acid, pH 7.4), 80µl 5mM NADPH, 30µl 100mM arginine, and 20mM 50µl calcium `chloride. The reaction mixture was kept in a shaking water bath for 20 minutes. Afterward, nitric oxide was then measured by adding 500µl of NaOH [ 55mmol/L) and 400µl of 75mmol/L ZnSO4 to the reaction mixture. Following that, the reaction mixture was centrifuged at 3000rpm for 15 minutes. To the supernatant, ethylenediamine was added and the color intensity was measured at 540nm [18].
Statistical Analysis
Statistical analysis was performed using a two-way analysis of variance (ANOVA) followed by LSD (Least Significant Difference) with the help of Microsoft Office Excel 2010 and IBM SPSS statistics for Windows versions 23. The results were expressed in mean ± SEM and in all cases, the difference was considered significant when p < 0.05.
Results
Serum Lipid Profile in Diabetic and Non- Diabetic Males and Females
Figure 1 shows the lipid profile of diabetic males and females individuals. Statistical analysis of data by two- way ANOVA showed insignificant effects of gender on total cholesterol and LDL-C F= 3.084 (p = 0.084) and F= 1.502 (p = 0.223) respectively. However, HDL-C and TGs showed significant gender effects F= 11.6 (p= 0.001) and F= 8.156 (p= 0.005). Moreover, diabetes showed significant effects (p=0.000) on total cholesterol (F= 42.843), HDL-C (F= 50.65), LDL-C (F= 20.41) and on TGs (37.041). On the other hand, gender x disease interaction (GSD) showed a significant effect on HDL-C (F= 13.01, p= 0.000). However insignificant effects were observed in total cholesterol (F= 0.142, p= 0.624), LDL (F= 1.24, p= 0.268) and TGs (F= 0.392, p= 0.533).
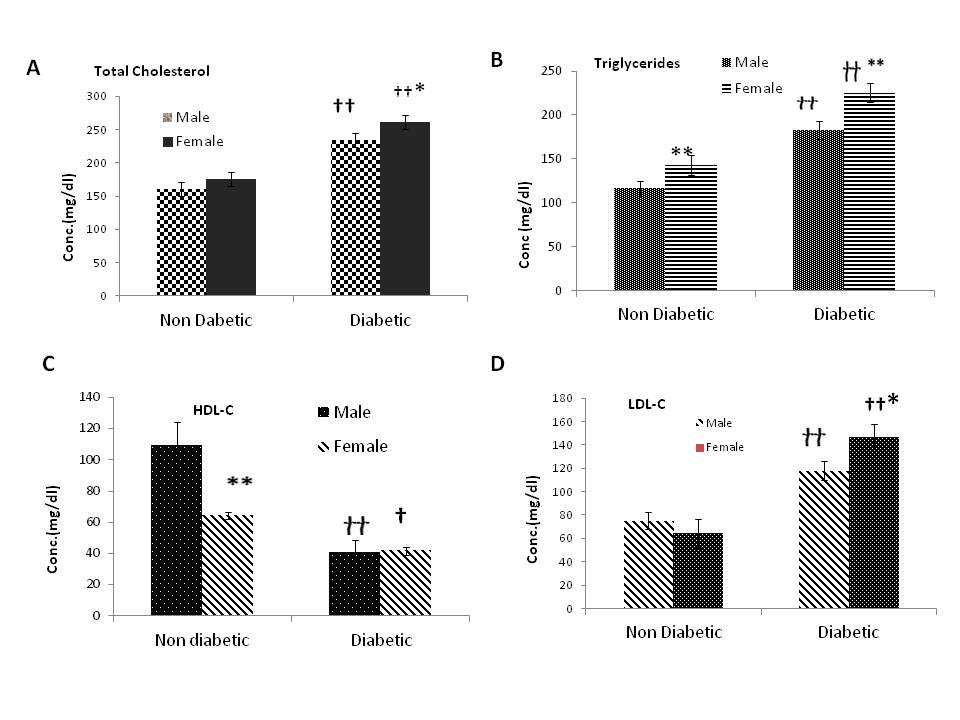
Figure 1: Evaluation of lipid profile in Diabetic and non- Diabetic male and female subjects. (A) Total Cholesterol (TC), (B) Triglycerides (TGs), (C) High-density lipoprotein cholesterol (HDL-C), (D) low-density lipoprotein- cholesterol (LDL-C). The results are expressed as the mean ± SEM. The results were analyzed by two-way ANOVA followed by LSD (least significant difference) test. The P-value < 0.05 was considered to be statistically significant. The significance of the difference is indicated by *P <0.05, p<0.01, *p<0.001 when non-diabetic and diabetic males were compared with respective diabetic and non- diabetic females. And †p<0.05, ††p<0.01, †††p<0.001 when the diabetic group was compared with respective non- diabetic controls.
Serum Oxidative Stress Markers in Diabetic and Non-Diabetic Males and Females
Fig 2 shows significant effects of gender on SOD (F= 63.86, p=0.000), GSH (F= 234.7, p= 0.000), MDA (F= 106.487, p=0.000) NOS (F= 4.280, p= 0.041, however, insignificant effect on catalase (F= 0.188, p= 0.666) was observed. Effects of disease were shown to be significant on SOD (F=105.909, p=0.000), GSH (F= 552.46, p=0.000), MDA (F= 21.19, p=0.000), catalase (F= 902.7,p=0.000) and NOS (166.72, p=0.000). Interaction between G X D (gender x disease) showed significant effects on SOD (F= 5.02 ,p= 0.027) and MDA (F= 15.75 ,p= 0.000 ) and non-significant effects were observed in GSH, catalase and NOS (F= 0.733 , p= 0.394 ), (F= 0.188 ,p= 0.665 ) and F= 0.127, p= 0.722 ) respectively
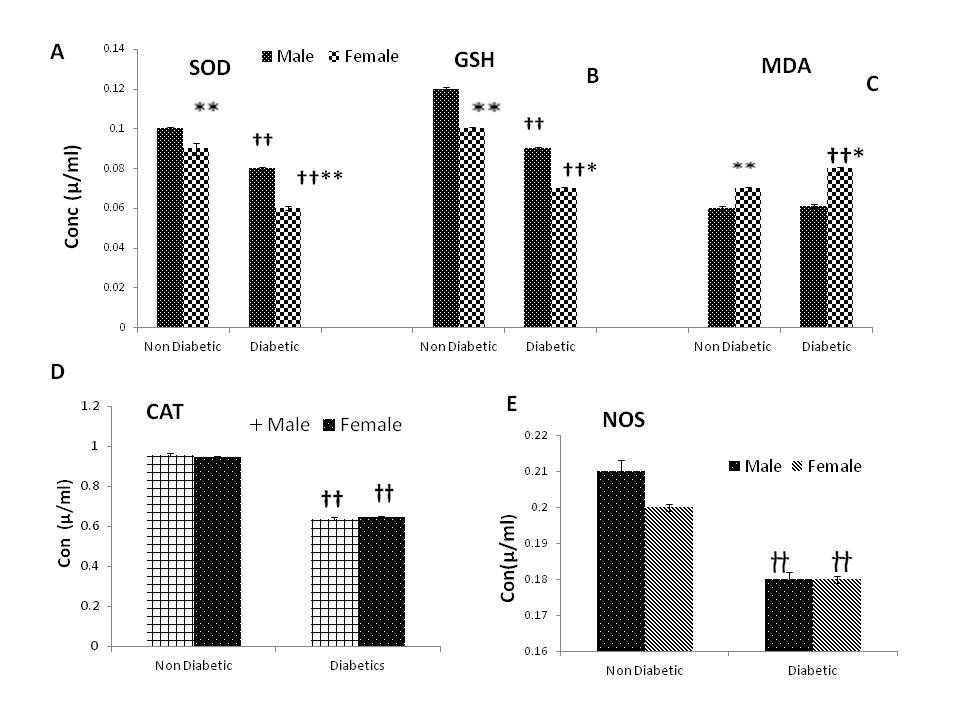
Figure 2: Evaluation of oxidative stress in diabetic and non-diabetic male and female subjects. (A) SOD, (B) GSH, (C) MDA, (D) CAT, (E) NOS. The results are expressed as the mean ± SEM. The results were analyzed by two-way ANOVA followed by LSD (least significant difference) test. The P-value < 0.05 was considered to be statistically significant. The significance of the difference is indicated by *P <0.05, p<0.01, *p<0.001 when non-diabetic and diabetic males were compared with respective diabetic and non-diabetic females. And †p<0.05, ††p<0.01, †††p<0.001 when the diabetic group was compared with respective non- diabetic controls
Discussion
Antioxidants in plasma and cells are free radical scavenging molecules and enzymes that can prevent the cells from deleterious effects of free radicals [10, 19]. It is confirmed by several studies that oxidative stress is associated with hyperlipidemia and hyperglycemia that deals with the complications in diabetes mellitus [20, 21]. However, the gender-based and oxidative stress-related complications in type II diabetes in the progression of cardiovascular diseases is still questionable. To the best of our knowledge, the present study was conducted for the first time on Pakistani males and females of central Punjab to investigate the gender-based changes in diabetes mellitus that lead to cardiovascular complications. The results of the present study indicate the increased oxidative stress in diabetic males and females compared to non-diabetic controls, which is represented by the marked reduction in superoxide dismutase and reduced glutathione in diabetic females. These results show a similarity with the experiments reported that the reduced activity of SOD is associated with the ROS-induced compensatory efforts in the subjects exposed to the oxidative stress [1, 22, 23].
These conformational changes in SOD could result from intermolecular and intra-molecular cross-linking of proteins that may accumulate H2O2 and favors lipid peroxidation and ultimately leads to atherosclerosis and cardiovascular complications [24]. Additionally, diabetic females were shown to have low SOD activity and reduced glutathione levels than diabetic male subjects. Similar to our finding’s other investigations on Arabs of Kuwait population reported higher levels of reactive oxygen species in females than males. Chen, et al., [ 2011] reported higher SOD in the brain and lung of female mice but non-significant changes in kidneys and heart of female and male mice [25]. One study had reported no gender-based relationship between. n mRNA expressions of SOD2 [26, 27]. This suggests that there is no uniform consensus exists in SOD levels of males and females. In line with oxidative stress, present results show increased TC in diabetic males and females compared to non- diabetic controls. However, female diabetic subjects showed a comparative increase in TC than diabetic male subjects. Other studies reported that the increase in circulating lipids and oxidation products of proteins can be used as a marker of developing complications in poorly controlled type 2 diabetes mellitus [28, 29]. Also, the increased TGs in controls and diabetic females compared to their respective controls in the present study reflects a close association between increased oxidative stress in females compared to males. These results confirm that women are at high risk of developing cardiovascular complications as a result of an increase in lipid oxidation products in the presence of diabetes mellitus than men. These results are consistent with findings reported earlier that increased oxidative stress is associated with an increased risk of developing cardiovascular diseases more in women than men [30, 31]. Paradoxically, clinical and preclinical studies conducted earlier had reported higher oxidative stress in men than in women [32, 33]. According to another study, vascular cells from males were found to have higher ROS compared to the cells obtained from females [10]. These gender-related discrepancies may also pinpoint the role of the immune response in the progression of atherogenic events and growing evidence suggests that women are at increased risk of autoimmune and inflammatory diseases [34, 35, 36].
The data shows increased LDL cholesterol in diabetic females compared to male diabetics. Further, LDL and HDL-C showed a marked increase and decrease [respectively] in diabetic males and females compared to controls (males and females). Several studies have reported the incidence of insulin resistance hypertriglyceridemia and low plasma HDL in diabetes as the major risk factors in the etiology of coronary heart diseases [37, 38]. A study on the Asian population of Pakistan has shown increased LDL-C and low HDL-C in women than men. It was suggested that abdominal obesity is associated with cardiac heart disease [39]. Another study conducted earlier on the urban population of India has reported that the LDL-C did not, but the levels of HDL-C and TC increased in premenopause women than men of similar age. High levels of TGs and lipoproteins have been considered as the major risk factors in women than men [40, 41].
Moreover, additional data in the current study on malondialdehyde showed a significant increase in diabetic females compared to non-diabetic females. Similar studies reported diabetic females with complications had increased MDA levels compared to male patients associated with acute myocardial infarction [42, 43, 44]. An increase in lipid peroxidation in obesity is related to mitochondrial and electron transport chain dysfunction in diabetes mellitus that is considered as the major cause of cardiovascular complications [45, 46]. Also, for females, the endocrine system follows an oscillating and complex profile therefore there exists a typical gender difference in fats accumulation, lipolysis, and other metabolic oxidation-reduction pathways. Honour, [ 2018] reported that the age-related differences in glutathione and malondialdehyde [MDA] levels in females could be due to menopause that is associated with the reduction in estrogen levels and the increased gonadotrophins and other hormones [47]. Evidence proved that at high concentration estrogen had antioxidant properties but generated pro-oxidant characteristics at low concentration due to its catechol effects [48]. According to underlying causes, women are at high risk of developing cardiovascular complications. This indicates the development of multiple feedback mechanisms to overcome such uncertain metabolic status in women.
In addition to this, gene expression of SOD and glutathione peroxidase had been proposed to be estrogen- dependent whereas catalase did not [10, 27]. These reports support present results showing a reduction in catalase activity in diabetic males and females compared to the non- diabetic controls, but changes remained insignificant when diabetic males were compared to diabetic females. Our findings show a similarity with other studies, reported by Barp J, et al [32, 33]. Moreover, one study reported no change in catalase activity in the brain, heart, and lungs but higher in the kidneys of females [25].
Our present study shows a remarkable reduction in nitric oxide synthase levels in diabetic males and females compared to non-diabetic controls. Experimental evidence confirmed an intact vascular endothelium inhibits atherosclerosis under physiological conditions and prediabetic rats were reported to have incomplete vascular endothelium and broken internal elastic fibers [49, 50]. Further, NOS expression was induced by lipopolysaccharides and cytokines that increased NO production in large amounts [51, 52]. Experimental studies on animal models have reported that the nitric oxide synthase inhibitors reduced inflammation by altering its expression patterns [53, 54]. Moreover, ROS oxidizes tetrahydrobiopterin which is a cofactor of NOS that leads to the uncoupling of eNOS and starts to produce free radicals instead of NO and elevates endothelial dysfunction [55].
It is worth mentioning that the diabetic women of the Pakistani population might be at a major risk of developing cardiovascular complications than men but the estrogen levels and other endocrinological changes in premenopause women might have some protective role. There may be an additional role of the gender-specific differences in the immune system that attributes to play a major role in diabetes-induced cardiac complications. Although the present study lacks the gender-based risk factors associated with hormonal changes and the immune system involving in the progression of diabetes-induced cardiac complications. The study may contribute to the first step towards the unveiling of gender-specific ROS-mediated changes in diabetes mellitus in the progression of cardiovascular risks in the Pakistani population. Further, the present study may contribute to the development of more specific targeted therapies.
Conclusion
It is concluded that diabetic women are more susceptible to develop cardiovascular complications than diabetic men. However, the present study holds evidence to put forward the new insights towards the synthesis of more specific therapeutic targets.
References
-
D’Oria R, Schipani R, Leonardini A, Natalicchio A, Perrini S, et al. (2020) The Role of Oxidative Stress in Cardiac Disease: From Physiological Response to Injury Factor. Oxidative Medicine and Cellular Longevity 2020: 5732956.
-
Díaz A, López-Grueso R, Gambini J, Monleón D, Mas- Bargues C, et al. (2019) Sex differences in age-associated type 2 diabetes in rats—Role of estrogens and oxidative stress. Oxidative Medicine and Cellular Longevity 2019.
-
Basanta-Alario ML, Ferri J, Civera M, Martínez-Hervás S, Ascaso JF, et al. (2016) Differences in clinical and biological characteristics and prevalence of chronic complications related to aging in patients with type 2 diabetes. Endocrinología y Nutrición 63(2): 79-86.
-
Bu S, Ruan D, Yang Z, Xing X, Zhao W, et al. (2015) Sex- specific prevalence of diabetes and cardiovascular risk factors in the middle-aged population of China: a subgroup analysis of the 2007–2008 China national diabetes and metabolic disorders study. PloS one 10(9): e0139039.
-
Ali F, Naqvi SAS, Bismillah M, Wajid N (2016) Comparative analysis of biochemical parameters in diabetic a;nd non- diabetic acute myocardial infarction patients. Indian heart journal 68(3): 325-331.
-
Rani V, Deep G, Singh RK, Palle K, Yadav UC (2016) Oxidative stress and metabolic disorders: Pathogenesis and therapeutic strategies. Life sciences 148: 183-193.
-
Zhonga S, Lia L, Shenab X, Lic Q, Xud W, et al. (2019) An update on lipid oxidation and inflammation in cardiovascular diseases. Free Radical Biology and Medicine 144: 66-278.
-
(2010) Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390(10100): 1151-1210.
-
Joseph P, Leong D, McKee M, Anand SS, Schwalm JD, et al. (2017) Reducing the global burden of cardiovascular disease, Part 1: the epidemiology and risk factors. Circ Res 121(6): 677-694.
-
Kander MC, Cui Y, Liu Z (2017) Gender difference in oxidative stress: a new look at the mechanisms for cardiovascular diseases. Journal of cellular and molecular medicine 21(5): 1024-1032.
-
Czubryt MP, Espira L, Lamoureux L, Abrenica B (2006) The role of sex in cardiac function and disease. Canadian journal of physiology and pharmacology 84(1): 93-109.
-
Mathur P, Ostadal B, Romeo F, Mehta JL (2015) Gender- related differences in atherosclerosis. Cardiovascular drugs and therapy 29(4): 319-327.
-
Peters SA, Huxley RR, Sattar N, Woodward M (2015) Sex differences in the excess risk of cardiovascular diseases associated with type 2 diabetes: potential explanations and clinical implications. Current Cardiovascular Risk Reports 9(7): 36.
-
Kakkar P, Das B, Viswanathan PN (1984) A modified spectrophotometric assay of superoxide dismutase. Indian J Biochem Biophys 21(2):130-132.
-
Beutler E, Duron O, Kelly BM (1963) Improved method for the determination of blood glutathione. J lab clin Med 61: 882-888.
-
Sinha AK (1972) Colorimetric assay of catalase. Analytical biochemistry 47(2): 389-394.
-
Ohkawa H, Ohishi N, Yagi K (1979) Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Analytical biochemistry 95(2): 351-358.
-
Cortas NK, Wakid NW (1990) Determination of inorganic nitrate in serum and urine by a kinetic cadmium- reduction method. Clinical chemistry 36(8): 1440-1443.
-
Saeed SA, Waqar MA, Zubairi AJ, Bhurgri H, Khan A, et al. (2005) Myocardial ischaemia and reperfusion injury: reactive oxygen species and the role of neutrophil. Journal-college of physicians and surgeons of Pakistan 15(8): 507-514.
-
Haidara MA, Yassin HZ, Rateb M, Ammar H, Zorkani MA (2006) Role of oxidative stress in development of cardiovascular complications in diabetes mellitus. Current vascular pharmacology 4(3): 215-227.
-
Singh U, Jialal I (2006) Oxidative stress and atherosclerosis. Pathophysiology 13(3): 129-142.
-
Brigelius-Flohe R, Wingler K, Muller C (2002) Estimation of individual types of glutathione peroxidases. Methods in enzymology 347: 101-112.
-
Brigelius-Flohé R (1999) Tissue-specific functions of individual glutathione peroxidases. Free Radical Biology and Medicine 27(9-10): 951-965.
-
Kairamkonda SR, Suryakar AN, Katkam RV, Ankush RD (2005) Oxidative stress in acute myocardial infarction. Solapur Med J 2: 42-46.
-
Chen Y, Ji LL, Liu TY, Wang ZT (2011) Evaluation of gender-related differences in various oxidative stress enzymes in mice. Chinese J Physiol 54(6): 385-390.
-
Rodford JL, Torrens C, Siow RC, Mann GE, Hanson MA, et al. (2008) Endothelial dysfunction and reduced antioxidant protection in an animal model of the developmental origins of cardiovascular disease. The Journal of physiology 586(19): 4709-4720.
-
Bellanti F, Matteo M, Rollo T, De Rosario F, Greco P, et al. (2013) Sex hormones modulate circulating antioxidant enzymes: impact of estrogen therapy. Redox biology 1(1): 340-346.
-
Bigagli E, Raimondi L, Mannucci E, Colombi C, Bardini G, et al. (2012) Lipid and protein oxidation products, antioxidant status and vascular complications in poorly controlled type 2 diabetes. The British Journal of Diabetes & Vascular Disease 12(1): 33-39.
-
Brownlee M (2001) Biochemistry and molecular cell biology of diabetic complications. Nature 414(6865): 813-820.
-
Khadir A, Tiss A, Kavalakatt S, Behbehani K, Dehbi M, et al. (2015) Gender-specific association of oxidative stress and inflammation with cardiovascular risk factors in Arab population. Mediators of Inflammation 2015: 512603.
-
Farooq A, Knez WL, Knez K, Al-Noaimi A, Grantham J, et al. (2013) Gender differences in fat distribution and inflammatory markers among Arabs. Mediators of Inflammation 2013.
-
Barp J, Araújo ASDR, Fernandes TRG, Rigatto KV, Llesuy S, et al. (2002) Myocardial antioxidant and oxidative stress changes due to sex hormones. Brazilian Journal of Medical and Biological Research 35(9): 1075-1081.
-
Ide T, Tsutsui H, Ohashi N, Hayashidani S, Suematsu N, et al. (2002) Greater oxidative stress in healthy young men compared with premenopausal women. Arteriosclerosis, Thrombosis, and Vascular Biology 22(3): 438-442.
-
Zwaka TP, Hombach V, Torzewski J (2001) C-reactive protein–mediated low density lipoprotein uptake by macrophages: implications for atherosclerosis. Circulation 103(9): 1194-1197.
-
Pirillo A, Norata GD, Catapano AL (2013) LOX-1, OxLDL, and atherosclerosis. Mediators of inflammation 2013.
-
Leuzzi C, Sangiorgi GM, Modena MG (2010) Gender‐ specific aspects in the clinical presentation of cardiovascular disease. Fundamental & clinical pharmacology 24(6): 711-717.
-
McKeigue PM, Shah B, Marmot MG (1991) Relation of central obesity and insulin resistance with high diabetes prevalence and cardiovascular risk in South Asians. The Lancet 337(8738): 382-386.
-
Giorda CB, Ozzello A, Gentile S, Aglialoro A, Chiambretti A, et al. (2015) Incidence and risk factors for severe and symptomatic hypoglycemia in type 1 diabetes. Results of the HYPOS-1 study. Acta diabetologica 52(5): 845-853.
-
Sarfraz M, Sajid S, Ashraf MA (2016) Prevalence and pattern of dyslipidemia in hyperglycemic patients and its associated factors among Pakistani population. Saudi Journal of Biological Sciences 23(6): 761-766.
-
Mercuro G, Deidda M, Bina A, Manconi E, Rosano GMC (2011) Gender-specific aspects in primary and secondary prevention of cardiovascular disease. Current pharmaceutical design 17(11): 1082-1089.
-
Tappia PS, Dhalla NS (2012) Modifiable factors for reducing the gender difference in lipid control. Clinical Lipidology 7(4): 379-387.
-
Madole MB, Bachewar NP, Aiyar CM (2015) Study of oxidants and antioxidants in patients of acute myocardial infarction. Advanced biomedical research 4: 241.
-
Lodovici M, Bigagli E, Luceri C, Mannucci E, Rotella CM, et al. (2015) Gender-related drug effect on several markers of oxidation stress in diabetes patients with and without complications. European journal of pharmacology 766: 86-90.
-
Patil N, Chavan V, Karnik ND (2007) Antioxidant status in patients with acute myocardial infarction. Indian Journal of Clinical Biochemistry 22(1): 45-51.
-
Montaigne D, Marechal X, Coisne A, Debry N, Modine T, et al. (2014) Myocardial contractile dysfunction is associated with impaired mitochondrial function and dynamics in type 2 diabetic but not in obese patients. Circulation 130(7): 554-564.
-
Niemann B, Rohrbach S, Miller MR, Newby DE, Fuster V, et al. (2017) Oxidative stress and cardiovascular risk: obesity, diabetes, smoking, and pollution: part 3 of a 3-part series. Journal of the American college of cardiology 70(2): 230-251.
-
Honour JW (2018) Biochemistry of the menopause. Annals of clinical biochemistry 55(1): 18- 33.
-
Pinchuk I, Weber D, Kochlik B, Stuetz W, Toussaint O, et al. (2019) Gender-and age-dependencies of oxidative stress, as detected based on the steady state concentrations of different biomarkers in the MARK-AGE study. Redox biology 24: 101204.
-
Wang S, Li J, Zhang C, Xu G, Tang Z, et al. (2019) Effects of aerobic exercise on the expressions and activities of nitric oxide synthases in the blood vessel endothelium in prediabetes mellitus. Experimental and therapeutic medicine 17(5): 4205-4212.
-
Westerterp M, van der Hoogt CC, de Haan W, Offerman EH, Dallinga-Thie GM, et al. (2006) Cholesteryl ester transfer protein decreases high-density lipoprotein and severely aggravates atherosclerosis in APOE* 3-Leiden mice. Arteriosclerosis, thrombosis, and vascular biology 26(11): 2552-2559.
-
Guo Z, Tan J, Zhuo C, Wang C, Xiang B, et al. (2014) Abscisic acid, H2O2 and nitric oxide interactions mediated cold‐ induced S‐adenosylmethionine synthetase in Medicago sativa sub sp. falcata that confers cold tolerance through up‐regulating polyamine oxidation. Plant Biotechnology Journal 12(5): 601-612.
-
Hossain M, Qadri SM, Liu L (2012) Inhibition of nitric oxide synthesis enhances leukocyte rolling and adhesion in human microvasculature. Journal of Inflammation 9: 28.
-
Asakura H, Kitahora T (2018) Antioxidants and polyphenols in inflammatory bowel disease: ulcerative colitis and Crohn disease. In Polyphenols: Prevention and treatment of human disease (pp. 279-292). Academic Press.
-
Trifilieff A, Fujitani Y, Mentz F, Dugas B, Fuentes M, et al. (2000) Inducible nitric oxide synthase inhibitors suppress airway inflammation in mice through down- regulation of chemokine expression. The Journal of Immunology 165(3): 1526-1533.
-
Mehta JL, Rasouli N, Sinha AK, Molavi B (2006) Oxidative stress in diabetes: a mechanistic overview of its effects on atherogenesis and myocardial dysfunction. The international journal of biochemistry & cell biology 38(5-6): 794-803.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State