Drug Therapy Problems among Patients with both Cardiovascular Diseases and Diabetes Mellitus in A Sub-Saharan African Referral Hospital
Background: Patients with both type 2 diabetes mellitus and cardiovascular disease receive multiple medications but there are limited studies on drug therapy problems among them in Sub-Saharan Africa. Objective: To determine the predictors of drug therapy problems among adult patients with both type 2 diabetes and cardiovascular diseases. Setting: Kenyatta National Hospital. Method: A cross-sectional study involving 180 adult patients with both comorbidities was conducted. Data collected included sociodemographic and clinical characteristics, medications prescribed and drug therapy problems. Data was analyzed using STATA v.13 at p72 months living with diabetes (p=0.007). Non-adherence was associated with the perception of disease control or cure (p
Introduction
Cardiovascular disease and Type 2 diabetes mellitus correlate closely as patients with T2DM are three to four times more likely to have CVD as well as high mortality [1]. Sub-Saharan Africa studies have indicated an increased burden of CVD and T2DM [2]. In Kenya, CVD and T2DM had an increasing mortality rate of 24% to 32% from the year 2009 to 2010, respectively [3]. According to National Diabetes Strategy (KNDS) [2010, 2011, 2012, 2013, 2014, 2015] statistics revealed that by 2030, 2 million people in Kenya will be living with diabetes if no preventive measures are put in place [3].
A DTP is an undesirable event in a patient that involves, or suspected to involve drug therapy and interferes with the health outcomes and requires a professional judgment to resolve [4]. Drug therapy problems pose great challenge to health professionals including affecting patients health outcomes and increased health care cost burden to patient as well as long hospitalisation, which result in morbidity [4, 5, 6, 7].
Use of multiple medicines particularly in patients with T2DM and CVD have resulted to increased chances of DTPs which are preventable [2, 6, 8, 9, 10, 11]. In Sub-Saharan Africa, studies have indicated that there are increased DTPs associated with chronic diseases [6, 12, 13, 14]. In Kenya, majority of patients with CVD and T2DM have risk of complications due to unmet glycaemic control and recommended blood pressures of ≤140/90 mmHg [15].
Several factors could contribute to DTPs. For instance, advanced age has an increased association with multiple conditions. Additionally, gender, poly-pharmacy, patient medication experiences, duration of chronic diseases, type of drugs, multiple medical conditions and renal impairment have all been implicated in DTPs [4, 9, 10]. As far as we are aware, there are limited published studies to investigate DTPs among T2DM patients with CVD in Kenya. The aim of the present study was to identify predictors of DTPs among patients with both T2DM and CVD before interventional program campaigns are structured.
Materials and Methods
Area of Study
This study was carried out in KNH at Diabetes and Endocrinology clinic (KNH DEOC), where most of the participants with both T2DM and CVD conditions are offered quality care. KNH is the national referral and teaching hospital whose DEOC clinic serves around 80 patients daily approximately 30 of whom have both T2DM and CVD.
Study Population
The study population consisted ofT2DM adult patients aged ≥18 years, diagnosed with any type of heart and blood vessel diseases including ischemic heart disease, stroke, cerebrovascular disease, hypertension, hypertensive heart disease, cardiomyopathy, valvular heart disease, rheumatic heart disease, aortic aneurysm, arrhythmias, endocarditis and pericarditis, and other circulatory diseases. Patients must have been undergoing long-term treatment and follow- up care in Kenyatta National Hospital OPDMEC during the study period.
Study Design
This was a hospital-based cross-sectional study.
Sample Size Determination
The study sample size was estimated using Cochrane’s formula [16]. There was previous study of assessment of DTPs in T2DM with CVD which estimated the prevalence of DTPs as 12.1% with an error margin of +/-10% [17]. Including these proportions at 95% confidence level, the minimum sample size was calculated as 163 participants. However, to allow for non-responders and data losses, a 10% was added to the calculated sample size to make total of 180 T2DM with CVD respondents.
Inclusion Criteria
These included male and female adult T2DM patients diagnosed with CVD and aged ≥18 years. In addition, they should be receiving at least one anti-diabetic and a CVD medication.
Data Collection
Data on social demographics characteristics, clinical characteristics and patient medication experiences and review of systems as well as the vital signs were abstracted into a predesigned data collection tool.
Data Analysis
The data collected was entered into Microsoft Excel and analyzed using STATA version 13.0 at 95% confidence level.
Ethical Approval
Clearances from the University of Nairobi and Kenyatta National Hospital-Ethics and research Committee was obtained before carrying out the study.
Results
Participant Characteristics
A total of 180 participants with both Type 2 diabetes and CVD attending the KNH Endocrinology and Diabetic clinic from 23rd July 2018 to 31st August 2018, were included and interviewed. Table 1 summarizes the social demographic characteristics of the study participants.
| Frequency (N=180) | Percentage (%) | |
|---|---|---|
| Sex | ||
| Male | 61 | 33.9 |
| Female | 119 | 66.1 |
| Age Years | ||
| <35 | 2 | 1.1 |
| 36-65 | 107 | 59.4 |
| >65 | 71 | 39.4 |
| BMI | ||
| 0-18.5 | 1 | 0.6 |
| 18.6-24.9 | 33 | 18.3 |
| 25-29.9 | 76 | 42.2 |
| >30 | 70 | 38.9 |
| Marital Status | ||
| Single | 39 | 21.7 |
| Married | 141 | 78.3 |
| Religion | ||
| Christian | 176 | 97.8 |
| Muslim | 4 | 2.2 |
| Smoking status | ||
| Never smoked | 138 | 76.7 |
| Previous smoker | 36 | 20 |
| Current smoker | 6 | 3.3 |
| Alcohol intake status | ||
| Never drunk | 108 | 60 |
| Previously drinking | 62 | 34.4 |
| Currently drinking | 10 | 5.6 |
| Level of education | ||
| Primary | 74 | 41.1 |
| Secondary | 70 | 38.9 |
| College/university | 27 | 15 |
| Informal | 9 | 5 |
| Employment status | ||
| Self employed | 74 | 41.1 |
| Not employed | 54 | 30 |
| Formally employed | 52 | 28.9 |
| Monthly Income, KES | ||
| 57 | 32 | |
| 0-5000 | 53 | 29.8 |
| 5000-10000 | 29 | 16.3 |
| 10000-30000 | 24 | 13.5 |
| >30000 | 15 | 8.4 |
| More than two comorbidities with DM and CVD | 62 | 34.4 |
| Age (mean ±SD) Years | 61.6(±11.3) range 19-95 |
Table 1: Social-demographic characteristics of the study participants (N=180).
Out of a total of 180 patients, with both DM and CVD in the study, there were (61, 33.9%) males and (119, 66.1%) females. The mean age was 61.6(±11.3) years. More than 50% of the patients had reached secondary level of education
| Frequency (n) | Percentage (%) | |
|---|---|---|
| Biguanides | 155 | 86.1 |
| Metformin | 155 | 86.1 |
| Insulin | 106 | 58.9 |
| Insulin mixtard | 105 | 58.3 |
| Sulphonyl ureas | 46 | 25.6 |
| Gliclazide | 16 | 8.9 |
| Glimepiride | 19 | 10.6 |
| Glibenclamide | 11 | 6.1 |
| Thiazolidinedione | 9 | 5 |
| Pioglitazone | 9 | 5 |
| Gliptins | 5 | 2.8 |
| Sitagliptin | 5 | 2.8 |
Table 2: Types of anti-diabetic drugs prescribed among the study participants.
and >60% earned Ksh<5000 as a monthly income (table 1). Table 2 outlines the major medications types and classes used by the study participants.
Almost 60% of the patients were prescribed insulin mixtard and 90% on metformin in managing diabetes. Conversely, there was inadequate prescription on diabetic patients (5, 3%) using sitagliptin medication (Table 2).
| Cardiovascular drugs | Frequency (n) | Percentage (%) |
| CCB | 90 | 50.1 |
| Amlodipine | 52 | 28.9 |
| Nifedipine | 37 | 20.6 |
| Nicardipine | 1 | 0.6 |
| Beta-blockers | 58 | 32.3 |
| Carvedilol | 29 | 16.1 |
| Atenolol | 21 | 11.7 |
| Nebivolol | 6 | 3.3 |
| Propanolol | 1 | 0.6 |
| Metoprolol | 1 | 0.6 |
| ACEI | 46 | 25.6 |
| Enalapril | 46 | 25.6 |
| ARBs | 104 | 57.8 |
| Losartan | 102 | 56.7 |
| Loop diuretics | 24 | 13.3 |
| Furosemide | 24 | 13.3 |
| Potassium sparing diuretics | 8 | 4.4 |
| Spironolactone | 8 | 4.4 |
| Thiazides | 76 | 42.2 |
| Hydroclorthiazide | 76 | 42.2 |
| Vasodilators | ||
| Hydralazine | 4 | 2.2 |
| Antiplatelet | ||
| Aspirin | 49 | 27.2 |
| Clopidogrel | 4 | 2.2 |
| Statins | ||
| Atorvastatin | 105 | 58.3 |
| Rosuvastatin | 5 | 2.8 |
| Others* | 16 | 10 |
Table 3: Types of cardiovascular drugs prescribed among the study participants.
The study also explored medication prescribed in management of CVD across all patients. Almost 50-60% of the patients were prescribed CCBs, statins and ARBs. Conversely, there was inadequate prescription of loop diuretics, potassium diuretics and vasodilators medications among this patients (Table 3).
Participants’ Clinical Characteristics
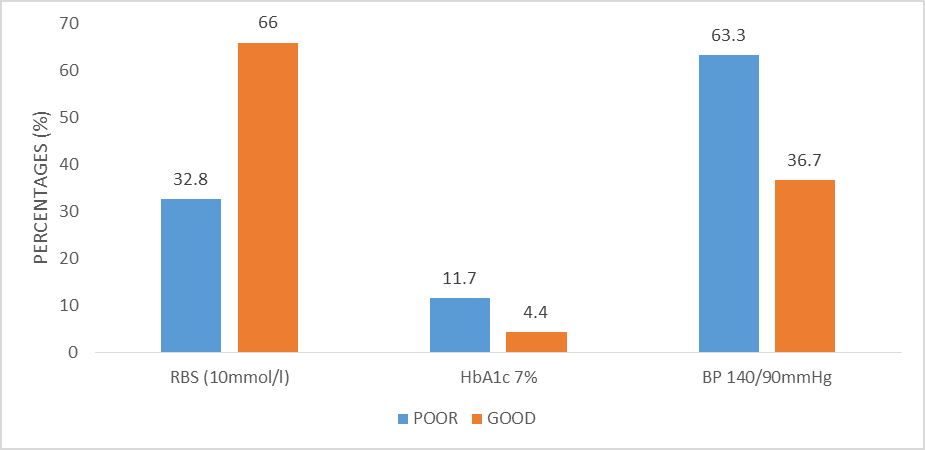
The participants mean duration of T2DM was 12 years ranging from 3 months to 45 years and mean duration of CVD was 11 years ranging from 3 months to 40 years. Over 70% of the participants had had both T2DM and CVD for more than 6 years. Sixty-two (34.4%) participants had more than two comorbidities. Arthritis was the most common comorbidities found in these patients (31, 17.2%).
In figure 1, at least a third of the participants (32.8%) had inadequate glycemic control. Additionally, more than half of the participants, (63%) had inadequate blood pressure control.
Frequency Of Drug Therapy Problems(DTPs)
As shown in figure 2, a total of 164 participants had at least one DTP. Needs additional drug was the most frequent DTP among these participants (87, 48.3%), followed by non- adherence at (71, 39.4%).
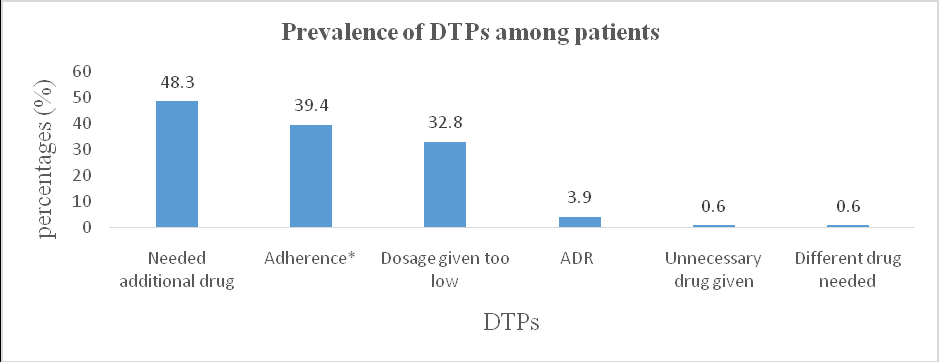
Key: ADR-adverse drug reaction, DTPs-drug therapy problems Figure 2: Prevalence of DTPs among patients.
Characterization of Drug Therapy Problems among the Participants
The seven drug therapy problems were adequately studied and five types of DTPs found, were categorized, reported, and characterized among the studied patients.
Unnecessary Drug Therapy: Out of five causes of unnecessary therapy given, the study reported only one (0.6%) sub-category DTP, whereby a patient had a non-drug therapy indicated rather than pharmacologic therapy.
Patient requiring additional drug therapy/ unmet need
The three sub-categories that characterize this DTP included preventive therapy required, identified untreated condition and synergistic therapy required. This study found out any patient who was not on antiplatelet, hypolipidemic drugs, failure to control blood pressure, pneumococcal vaccine, and failure to control blood glucose was considered to need an additional drug as patients have both CVD and T2DM.
Adverse Drug Reaction
There were seven sub-categories of this DTP. Only two causes were identified. These were undesirable effects and unsafe drug at (7, 3.9%) and (1, 0.6%), respectively.
Dosage too low
There were seven sub-categories of this DTP. The most frequent cause of dosage too low was among (43, 23.9%) patients taking ineffective dose. Twelve (6.7%) patients did not require altering doses but to further monitor their glycemic and blood pressure levels. The lowest dosage too low was among (4, 2.2%) patients who required dose frequency adjustment in their antihypertensive medications.
Adherence to Medications among the study participants
The rate of non-adherence, as a DTP, to the prescribed drugs among the study participants was at 71(39.1%). Thirty (16.7%) patients did not understand instructions given to them by the prescriber and therefore failed to take their medications. Additionally, 24 (13.3%) patients deliberately stopped the prescribed drug product. In addition, 13 (7.2%) patients failed to take their medications because of high cost of drug product.
Predictors of drug therapy problems
We constructed a bivariate logistic regression models consisting of associations between predictors and three DTP response variables. Table 5 shows a statistically significant association (p-value ≤ 0.05) between a specified predictors and an individual DTP category. For instance, we found that the occurrence of non-adherence was associated with medication experiences of a patient has. For example, for a unit increase in cost of drugs, the odds of non- adherence to medication increased by 0.52. For a unit increase in patient expectations of relief and not a cure, the odds of medication non-adherence increased by 0.21. The unit increased in coercing the patients to take medications, the odds of medication non-adherence increased by 0.31, and the unit increase of wrong belief that they could stop taking medications when the disease was under control, the odds of medication non-adherence increased by 7.74.
We also found out that the occurrence of needs additional drug was associated with clinical characteristics of a patient has. For example, the odds of getting an additional drug were 0.48 times among patients with more than 72 months of T2DM compared to those with less than 72 months of T2DM. Similarly, the odds of having a needs additional drug were 3.8 times higher among patients who took furosemide compared to those who did not.
Additionally, we found in this study that low dosage of medication was associated with clinical characteristics of patients. For example, the odds of under-dosage were 2 times higher in females as compared to male counterparts. In addition, the odds of under-dosage were 0.66 times higher in those who were earning less than shillings 5000 compared to those who earned higher than that. Similarly, the odds of under-dosage were higher among those who had poor controlled blood pressure compared to those who did not; while the odds of to low dosages were higher among those who had poor controlled glycemic levels using 2-hour postprandial test.
| Dependent variable | Predictor variable | COR (95%CI) | P-Value |
|---|---|---|---|
| Non-adherence | Cost of drugs | 0.52(0.29-0.96) | 0.037 |
| Patient expectations | 0.21(0.11-0.43) | <0.001 | |
| Compelled to take medications | 0.31(0.16-0.59) | <0.001 | |
| Stopping when condition is under control | 7.74(3.26-18.39) | <0.001 | |
| Needs additional drug | Duration of T2DM | 0.48(0.25-0.92) | 0.026* |
| Furosemide | 3.78(1.42-10.04) | 0.008* | |
| Dosage too low | Sex | 2.04(1.01-4.12) | 0.046 |
| Monthly income | 0.66(0.49-0.87) | 0.003* | |
| Poor blood pressure control | 2.42(1.20-4.88) | 0.013* | |
| 2-hours postprandial test | 5.21(2.65-10.24) | <0.0001* |
COR=Crude Odds Ratio; CI=Confidence Interval; *statistically significant result; T2DM=Type 2 Diabetes Mellitus. Table 3: Bivariate logistic regression for Different DTPs and various predictors.
Multivariate analysis conducted, identified key predictors of non-adherence, needs for an additional drug and dosage too low as shown in table 6. The study found out that there was no association between non-adherence and patients who perceived cost of medications because it lost significance on adjusting for confounding by patient’s expectations and being forced to take medications and stopping to take when condition is under control. However, the odds of having medication non-adherence among patients who had expectations of relief and not a cure were 0.24 times (AOR=0.11-0.56; 95% CI: p=<0.001) compared to those with expectations of cure. Moreover, patients compelled to take medications had 0.28 times the odds (AOR=0.12-0.67; 95% CI: p=<0.001) of being non-adherent compared to those not compelled. Also the odds (AOR=2.64-18.51; 95% CI: p=<0.001) of non-adherence amongst those who believed that they could stop taking medications when the disease was under control was 6.99 times the odds of non-adherence amongst patients who believed that they needed to take their medicines in the absence of any symptoms. Similarly, the odds of getting an additional drug were 0.48 times among patients with more than 72 months of T2DM compared to those with less than 72 months of T2DM.
Additionally, patients taking furosemide had 4.71 times the odds (AOR=1.72-12.89; CI: P=< 0.003) of being prescribed an additional drug compared to those who had none. Based on this analysis, patients with no income had 0.64 times the odds (AOR=0.47-0.89; 95% CI: P=<0.007) of receiving dosage too low as compared to those who were earning. Similarly, for a unit increase in poorly controlled blood pressure, the odds of under-dosing increased by 2.76 (95% CI 1.26-6.09, p=0.012). Additionally, for a unit increase in poorly controlled blood sugars using 2 hours’ postprandial test, the odds of under-dosing increased by 4.78 (95% CI 2.19-9.52, p=< 0.001).
| Predictor variable | AOR (95%CI) | P-Value | |
|---|---|---|---|
| Non-adherence | Patient expectations | 0.24 (0.11-0.56) | 0.001* |
| Non-adherence | Compelled to take medications | 0.28 (0.12-0.67) | <0.001* |
| Non-adherence | Stopping when condition is under control | 6.99 (2.64-18.51) | <0.001* |
| Needs additional drug | Duration of T2DM | 0.39 (0.19-0.78) | 0.007* |
| Needs additional drug | Furosemide | 4.71 (1.72-12.89) | 0.003* |
| Dosage too low | Monthly income | 0.64 (0.47-0.89) | 0.007* |
| Dosage too low | Poor blood pressure control | 2.76 (1.26-6.09) | 0.012* |
| Dosage too low | 2-hours postprandial test | 4.57 (2.19-9.52) | <0.0001* |
Table 6: Multivariate analysis of independent predictors and DTPs in the study population.
AOR=Adjusted Odds Ratio: CI=Confidence Interval; *statistically significant result; T2DM=Type 2 Diabetes Mellitus; Table 4: Multivariate analysis of independent predictors and DTPs in the study population.
Discussion
The goal of the study was to describe the characteristics and predictor factors of DTPs in patients with both T2DM and CVD followed up at KNH in Sub-Saharan Africa. These findings revealed that review of systems and complete physical examination was important to identify any drug- related adverse events, untreated and poorly managed cardiovascular and diabetic complications, which were classified as a prescriber-related DTPs. In this study, ninety two (51%) participants had severe daytime malaise which is one of the signs of chronic uncontrolled DM especially in patients with obesity [18]. Chronic malaise is not usually recognized as a key problem amongst patients with both T2DM and CVD.
Almost a half (44.4%) of the patients complained of weight gain, which could have been an adverse drug reaction of sulphonyl-ureas, thiazolidinediones and insulin. This finding showed similar results with a study done in USA [19]. This study also reported bladder dysfunction secondary to poor glycemic control in at least a third (36.1%) of our patients which correlated with studies done in USA [18, 19].
In our study it was revealed that HbA1c were rarely monitored which correlated with the studies done in KNH and yet the relationship between HbA1c and microvascular complications are well established [20]. Under-dosing of antidiabetic as revealed in our study, which contributed to poorly controlled diabetes, was due to lack of pocket reference guidelines among KNH clinicians. A study by Professor English found that in many settings in Kenya, clinicians do not have access to treatment guidelines [21].
An unexpected finding was a high prevalence (44.5%) and symptoms of upper respiratory tract complains such as nasal congestion (14, 7.8%), and throat problems (5, 5.6%) and coughing (30, 16.7%) and shortness of breath (29, 16.1%). A possible explanation was the cold climate over the month of June and July under which the study was conducted. The high prevalence of higher respiratory complains highlight the need for prophylaxis with influenza and pneumococcal vaccines among elderly patients [22, 23, 24].
Serious unmet medication needs were, need for pneumococcal vaccinz, lack of antiplatelet therapy and hypolipidemic agents, and need for additional medication for better control of hypertension and diabetes [2, 9, 24, 25, 26, 27, 28]. These include SGLT2 inhibitors, which have a novel insulin- independent mechanism and are preferred to lower elevated plasma glucose level. Poorly controlled hypertension was unmet need in our study. Limitation of existing guidelines in our settings is that they are based on Caucasian populations who tend to respond better to existing antihypertensive drugs such as ACEI [29].
Local guidelines need to be developed to identify combinations that are effective in African populations [30]. Dosages were considered too low if glycemic or cardiovascular goals were not attained. The high prevalence of under-dosage in the study site could be due to lack of published dosing guidelines and inter-patient variation in drug response, which was beyond the scope of the present study. The key reasons for non-adherence provided by the patient was failure to understand the instructions (30, 16.7%). This showed that patients never received adequate counseling on the use of their medication [9]. The other cause of non-adherence was patients preferring not to take medications (24, 13.3%) because they simply disliked them. In many settings all-over the world, patients view medication taking as ‘interruptive, discouraging, frustrating, confusing, and tiring [4]. These findings highlight the need for medication management as a solution to non-adherence.
Our observation, after logistic regression was done, is that, patient expectations, coercion to take medications, and belief that stopping to take medications when the condition is under control, were significant predictor of non-adherence. Similarly, duration of T2DM and furosemide were significant predictors of needs for an additional drug. Additionally, monthly income, poor blood pressure control, and 2 hours’ postprandial test were significant predictors of dosage too low. The greater the expectation for a cure, the greater they misunderstood their illness and the greater the chance for non-adherence [31, 32]. Additionally, the greater the coercion to take medications from relatives, the greater the patients could adhere to their medications. This observation adds support to the concept of DOT (Directly Observed Therapy) in TB program [32]. Furthermore, the greater the belief of stopping to take mediations when the condition is under control the higher the patients would get non-adherent. To improve adherence among these patients, the pharmacist should provide reassurance and information to patients and thus improve adherence [3, 33].
Our findings also observed that the greater the duration of illness (more than 72 months), the greater the developed self-care skills in a patient and the lesser the need for an additional drug [33]. Additionally, patients with T2DM and CVD using furosemide as an antihypertensive, may need an additional drug to manage hypertension because of its short duration of action [34, 35]. Our findings on the associations between too low dosage and the presence of increased 2-hour post prandial test, poor blood pressure control and lack of income corroborate findings reported by other researchers [35, 36, 37, 38].
Our study had several limitations. First, cross sectional design cannot be used to determine the causal relationships. For future research, our study should be seen as exploratory to benchmark interesting hypothesis [39, 40, 41, 42, 43, 44, 45]. Secondly, the data collection tool was not well designed to capture data on all possible types of ADRs. Thirdly, there were inadequate documentation of other types of CVD other than hypertension in the study site. Therefore, most patients captured were hypertensive patients. Lastly, the study was limited to T2DM and CVD patients only and therefore, the findings may not be generalizable to other chronic conditions. Our study concluded that
- Patients with both comorbidities were most likely to be non-adherent,
- Patients require an additional drug, and receive dosage too low.
- This current study will assist pharmacy and health care workers in not only early patient’s beliefs and perceptions identification, but also guide in drug therapy problems identification, prevention, and management of patients with both comorbidities.
Acknowledgements
I would like to thank the patients at KNH DEOC for voluntarily agreeing to participate in the study. I also thank the staff at Diabetic clinic (KNH) for their support.
References
-
Nathan DM, Meigs J, Singer DE (1997) The epidemiology of cardiovascular disease in type 2 diabetes mellitus: how sweet it is ... or is it?. Lancet 350(1): S4-S9.
-
Kayode OO, Odukoya O, Oluwarotimi O, Olopade OB, Fasanmade OA (2015) Pattern of complications and comorbidities among diabetic patients in a tertiary healthcare center in Nigeria. J Clin Sci 12(1): 29-35.
-
Kainga MKS (2011) Barriers in preventing long-term complications among patients with type 2 diabetes mellitus at the Kenyatta national hospital.
-
Robert J C, Strand L, Morley P (2012) Pharmaceutical Care Practice: the patient centered approch to medication management. 3rd (Edn.), Robert Cipole, linda M Strand PM, (Eds.), Mc Graw Hill, pp: 1-697.
-
Al-Arifi M, Abu-Hashem H, Al-Meziny M, Said R, Aljadhey H (2014) Emergency department visits and admissions due to drug related problems at Riyadh military hospital (RMH), Saudi Arabia. Saudi Pharm J 22(1): 17-25.
-
Kanagala V, Anusha A, Rao B, Challa S, Nalla K, et al. (2016) A study of medication-related problems in stroke patients: A need for pharmaceutical care. J Res Pharm Pract 5(3): 222-225.
-
Shareef J, Sandeep B, Shastry CS (2014) Assessment of Drug Related Problems in Patients with Cardiovascular Diseases in a Tertiary Care Teaching Hospital. J Pharm Care 2(2): 70-76.
-
Al-Taani GM, Al-Azzam SI, Alzoubi KH, Darwish Elhajji FW, Scott MG (2017) Prediction of drug-related problems in diabetic outpatients in a number of hospitals , using a modeling approach. Drug Healthcare Patient Saf 9: 65- 70.
-
Huri HZ, Wee HF (2013) Drug related problems in type 2 diabetes patients with hypertension : a cross-sectional retrospective study. BMC Endocr Disord 13: 2.
-
Huri HZ, Ling LC (2013) Drug-related problems in type 2 diabetes mellitus patients with dyslipidemia. BMC Public Health 13: 1192.
-
Vilar L, Canadas V, Arruda MJ, Arahata C, Agra R, et al. (2010) Comparison of metformin, gliclazide MR and rosiglitazone in monotherapy and in combination for type 2 diabetes. Arq Bras Endocrinol Metabol 54(3): 311-318.
-
Njeri LW (2016) Assessment of Medication related problems among patients with chronic kidney disease in Kenyatta National Hospital. Int J Clin Pharm 1: 1-8.
-
Okerosi EK, Okalebo FA, Opanga SA, Guantai AN (2017) Prevalence and Risk Factors for Medication Discrepancies on Admission of Elderly Diabetics at Kenyatta National Hospital, Kenya. African J Pharmacol Ther 6(1): 54-63.
-
Degu A, Njogu P, Weru I, Karimi P (2017) Assessment of drug therapy problems among patients with cervical cancer at Kenyatta National Hospital, Kenya. Gynecol Oncol Res Pract 4: 15.
-
Ministry of Health, Kenyan National Bureau of Statistics WHO (2015) Kenya STEPwise Survey for Non Communicable Diseases Risk Factors 2015 Report 1: 71- 80.
-
Kasiulevičius V, Šapoka V, Filipavičiūtė R (2006) Sample size calculation in epidemiological studies. Gerontologija 7(4): 225-231.
-
Hamid A Al, Aslanpour Z, Aljadhey H, Ghaleb M (2016) Hospitalisation Resulting from Medicine-Related Problems in Adult Patients with Cardiovascular Diseases and Diabetes in the United Kingdom and Saudi Arabia. Int J Environ Res Public Health 13(5): 479.
-
Large DM, Routledge A, Cowley ML, Mustchin CP, Gibson GJ (2003) Chronic malaise in uncontrolled type 2 diabetes due to obstructive sleep apnoea. Pract Diabetes Int 20(8): 297-299.
-
Provilus A, Mcfarlane SI, Marie Abdallah (2011) Weight gain associated with antidiabetic medications. Therapy 8(2): 113-120.
-
Matheka DM, Kilonzo JM, Munguti CM, Mwangi PW (2013) Pattern, knowledge and practices of HbA1C testing among diabetic patients in a Kenyan tertiary referral hospital. Global Health 9: 55.
-
Pacchioni G (2016) Magnetic influence. Nat Rev Mater 1: 2016.
-
Robillard R (1960) Pulmonary infections and diabetes mellitus. Diabetol Croat 89: 1135-40.
-
Ciljakova M, Vojtkova J, Durdik P, Turcan T, Petrikova M, et al. (2009) Cough reflex sensitivity in adolescents with diabetic autonomic neuropathy. Eur J Med Res 4(4): 45- 48.
-
Song WJ, Morice AH, Kim MH, Lee SE, Jo EJ, et al. (2013) Cough in the Elderly Population: Relationships with Multiple Comorbidity. PLoS One 8(10): e78081.
-
Breu F, Guggenbichler S, Wollmann J (2008) Journal of the Malta College of Pharmacy Practice. Vasa.
-
De Boer IH, Bangalore S, Benetos A, Davis AM, Michos ED, et al. (2017) Diabetes and hypertension: A position statement by the American diabetes association. Diabetes Care 40(9): 1273-1284.
-
Manley HJ, Drayer DK, Muther RS (2003) Medication- related problem type and appearance rate in ambulatory hemodialysis patients. BMC Nephrol 4: 10.
-
(2014) ACC/AHA Release Updated Guideline on the Treatment of Blood Cholesterol to Reduce ASCVD Risk. Am Fam Physician 90(4): 260-265.
-
Khan JM, Beevers DG (2005) Management of hypertension in ethnic minorities. Heart 91(8): 1105- 1109.
-
Flack JM (2007) Epidemiology and Unmet Needs in Hypertension. J Manag Care Pharm 13(8): 2-8.
-
Mann CJ (2003) Observational research methods. Research design II: cohort, cross sectional, and case- control studies. Emerg Med J 20(1): 54-60.
-
Program C (2003) Tuberculosis Prevention and Control Program. Minnesota Dep Heal 1: 2-3.
-
Barker I, Steventon A, Williamson R, Deeny SR (2018) Self-management capability in patients with long- term conditions is associated with reduced healthcare utilisation across a whole health economy: Cross- sectional analysis of electronic health records. BMJ Qual Saf 27: 989-999.
-
Sica DA, Carter B, Cushman W, Hamm L (2011) Thiazide and loop diuretics. J Clin Hypertens 13(9): 639-43.
-
Aliyi O, Hussien M, Kefale B (2015) Problems of using Hydrochlorothiazide Diuretic in Adult Diabeti c Patient in Diabetic Clinic of Adama Hospital Medical College, East Shoa Zone, Oromia Regional State, Ethiopia. Clin Pharmacol Biopharm 4: 134.
-
Hamaker EL, van Hattum P, Kuiper RM, Hoijtink H. Model Selection Based on Information Criteria in Multilevel Modeling. Handb Adv Multilevel Anal pp: 231-255.
-
Novello MF, Rosa MLG, Ferreira RT, Nunes IG, Jorge AJL, et al. (2017) Compliance with the Prescription of Antihypertensive Medications and Blood Pressure Control in Primary Care. Arq Bras Cardiol 108(2): 135- 142.
-
García-Pérez LE, Álvarez M, Dilla T, Gil-Guillén V, Orozco- Beltrán D (2013) Adherence to therapies in patients with type 2 diabetes. Diabetes Ther 4(2): 175-194.
-
Brown JS, Wessells H, Chancellor MB, Howards SS, Stamm WE, et al. (2005) Urologic complications of diabetes. Diabetes Care 28(1): 177-185.
-
Brown JS, Vary KTM (2008) Sexual and Urologic Problems of Diabetes. Natl Inst Diabetes Dig kidney Dis 9: 1-8.
-
(2018) Introduction: Standards of Medical Care in Diabetes—2018. Diabetes Care 41(1): S1-S2.
-
32. Medications BP, Changes M (2014) Treatment of Hypertension: JNC 8 and More. Res Cent 3120: 209-472.
-
Jones JK, Gorkin L, Lian JF, Staffa JA, Fletcher AP (1995) Discontinuation of and changes in treatment after start of new courses of antihypertensive drugs: a study of a United Kingdom population. Br Med J 311(7000): 293- 295.
-
GMC (2013) Good practice in prescribing and managing medicines and devices. pp: 1-11.
-
Agarwal R (2018) Thiazides versus loop diuretics in the treatment of hypertension. 1: 1-5.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State