Mechanistic Insights of Rutin against Metabolic Disorders
Rutin, a quercetin glycoside comes under the class flavonol. The aglycone part of rutin is known as quercetin. It is found in numerous fruits and plants, especially apricots, buckwheat, cherries, grapefruit, grapes, oranges, and plums. Rutin shows cardioprotective, neuroprotective, and nephroprotective effects mediated via its antioxidant mechanism. The neuroprotective effect of rutin is utilized in the treatment of Parkinson’s disease. It has been documented in the scientific literature that rutin improves obesity through brown fat activation, modulates DNA damage signaling in cancer cells, reduces inflammation by inhibiting eicosanoid biosynthesis, lipoxygenase, cyclooxygenase, and phospholipase A2 activities, enhances insulin release as well as decreases the expression of resistin along with increases the expression of PPAR γ in diabetic patients, increases total cholesterol, high-density lipoprotein and very low-density lipoprotein levels, whereas low-density lipoprotein level decreases resulting into antilipidemic activity, inhibits diabetic liver injury and diabetic cardiomyopathy. Repurposing of rutin was also done against SARS-CoV-2. Our study aims to survey the most recent progress with emphasis on how rutin adapts intracellular signaling cascades to treat different metabolic disorders. However, the precise cellular and molecular mechanisms of rutin are known and more clinical studies are required to provide a novel therapeutic approach for the treatment of metabolic disorders.
Introduction
The term “metabolic syndrome” (MetS) is used to describe a group of metabolic disorders that includes atherogenic dyslipidemia, insulin resistance, central obesity, and hypertension. Atherosclerotic cardiovascular disease is highly associated with metabolic syndrome (CVD). Both inherited and environmental variables contribute to the development of MetS and its associated pathophysiology, inflammation that ultimately results in CVD. As awareness of the worldwide obesity pandemic has grown, so too has that of MetS. Diagnosis at an early stage is essential for successful change of lifestyle and risk factors. metformin, statins, and Antihypertensives are examples of pharmaceuticals used in the treatment of MetS that target specific aspects of the disease. Some dietary components and natural chemicals, collectively referred to as nutritious food, have been found to be effective in the management of metabolic syndrome [1].
The metabolic syndrome (also known as insulin resistance syndrome, syndrome X, hypertriglyceridemia of the waist, and the fatal quartet) is now widely acknowledged as a significant risk factor for cardiovascular disease. The first universally accepted definition of MetS was developed in 1998 by the World Health Organization’s diabetes consultation group. Those with insulin resistance (either impaired fasting glucose, impaired glucose tolerance, or type 2 diabetes mellitus) and at least two other risk factors, including obesity (measured by a high waist-to-hip ratio or a high BMI), hyperlipidemia (low HDL cholesterol), or hypertension, were classified as having metabolic syndrome.
MetS incidence varies greatly from one region to another, and is generally directly proportional to the rate of obesity in that region. Age, gender, race/ethnicity, and diagnostic criteria all have a role in the widely varying estimates of prevalence. It is estimated that between 20 and 25 percent of the European population and at least 20 percent of the American population suffer with MetS. While the prevalence of MetS is lower in South-East Asia, it is quickly catching up to Western levels. Based on data from the National Health and Nutrition Examination Survey (NHANES), Beltrán-Sánchez and colleagues found that the age-adjusted prevalence of MetS in the United States decreased from 25% in 2000 to 22.9% in 1999/2000 and 2009/2010.
Medical professionals have been making use of Rutin, which was discovered in 1842 [2], to treat vascular problems because their discovery has been linked to capillary permeability and fragility. Numerous plants contain this quercetin glycoside, making it quite common. Rutin is a kind of flavonoid, which are plant secondary metabolites. Since rutin is a frequent quercetin glycoside, it is chemically comparable to these molecules, which are the most commonly dispersed flavonoids in herbal and plant foods. More than 6,000 unique plant pigments, called flavonoids, are classified into many categories based on their chemical structure, including flavan-3-ols, flavonols, flavonones, isoflavones, and 61 anthocyanidins [3, 4].
People get their supply of flavonoids from the plants they eat and the medicines they take. The typical human diet provides 1-2 g of flavonoids per day [4]; they are primarily obtained from vegetables, fruits, tea, and wine. Plants with flavonoids present are less likely to be eaten by insects and larger mammals that eat plants for food. Positive effects of these chemicals on a variety of human disorders, including cancer and cardiovascular disease, have been described. They were also found to be effective against free radicals, inflammation, tumors, and viruses [5]. In vitro and in vivo investigations have shown that flavonoids can cross the blood-brain barrier and have a wide range of effects on the neurological system. The antioxidant characteristics of flavonoids are mostly responsible for their biological activity [6]. However, flavonoids may also affect cell activity by acting selectively on several protein kinase and lipid kinase signaling pathways or by binding to the ATP-binding sites of many proteins. Behavioral effects in animal models of anxiety, sedation, and convulsions also suggested that they might be ligands for benzodiazepine binding sites of the -aminobutyric acid type A (GABAA) receptor.
It’s possible that flavonoids have an impact on the functioning of other neurotransmitter systems as well. Scientists found that quercetin can affect the activation of adenosine, serotonin, glycine, and acetylcholine receptors by up to 84 percent [7, 8, 9, 10]. In the present study, we aimed to investigate the effect of rutin on different metabolic disorder and also aimed to investigate different type of mechanism that how rutin work on different type of metabolic disorders like anti-aging, type 2 diabetes , and how rutin ameliorates obesity through brown fat activation.
Sources of Rutin
Numerous fruits and vegetables contain the flavonol rutin [11]. This substance was initially discovered in the plant Ruta graveolens L, after which it was named. Among fruits, vegetables, and grains, grapes and buckwheat are the two most important sources (Figure 1). Cereals and pseudocereals lack rutin, however, [12]. Extracts from the skin of many grape (Vitis vinifera L) cultivars have been discovered to contain rutin [13].
A wide range of values were discovered, from 1.592 mg/100 g dry weight in Montepulciano and Sangiovese to 89.3 mg/100 g in Merlot and Cabernet Sauvignon. The ruin in buckwheat is a very significant source. There are 15 annual and perennial species in this genus, but only three— Perennial buckwheat (Fagopyrum esculentum Moench.), Tatary buckwheat (Fagopyrum tataricum L. Gaertn.), and Fagopyrum esculentum Moench.—are of any commercial interest (Fagopyrum cymosum Meisn.). Researchers have discovered that the content varies among individuals of this species due to the effect of environmental factors on growth. In addition, its content varies across different plant sections, with the highest concentration in common buckwheat hulls (3.250 mg/100 g dry weight) and lower concentrations in the green parts of the plant (157 mg/100 g dry weight) [14]. Seeds from the Tatary variety of buckwheat contain more rutin than seeds from the more common buckwheat [15]. Rutin concentration may also be affected by environmental factors including ultraviolet (UV) radiation [16, 17].
The rutin content of Amaranthus species has also been reported [18]. The rutin content differs significantly according on the species, with Amaranthus hybrids and Amaranthus cruentus providing the highest levels. Seeds contain the highest concentration of rutin at 8 mg/100 g dry weight, whereas leaves have the lowest concentration at 2.450 mg/100 g dry weight. Asparagus’s rutin content can be improved by growing it in an open environment rather than hydroponically, therefore the culture circumstances are crucial. Asparagus cladophyls that are discarded contain significant quantities of rutin as well. Another African plant with medicinal uses, Gubeish (Guiera senegalensis), also contains rutin [19]. Capers, onions, green asparagus, and sea buckthorn are only some of the plants whose components all contain rutin. St. John’s wort leaves have a content of 2.400 mg/100 g, and caper leaves have a value of 2.750 mg/100 g.

Chemistry of Rutin
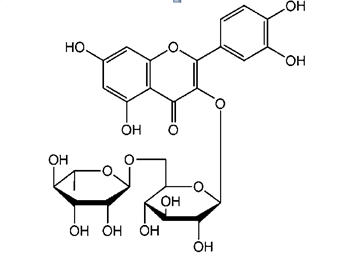
Flavonoids are naturally occurring polyphenolic chemicals found in a wide variety of fruits and plants [11]. The flavonol glycoside rutin (quercetin-3-O-rutinoside) is commonly known as vitamin P. Plants at a higher trophic level produce it to shield themselves from harmful UV rays and pathogens [20]. To make the molecule more water-soluble, the phenolic group has been chemically bonded to sugar, making it more hydrophilic (Figure 2). Intestinal microflora are capable of catalysing the enzymatic reaction that breaks down rutin into quercetin and rutinose. This is why quercetin and rutin often occur together [21]. Antioxidant activity, in the form of free-radical scavengers, is a feature shared by rutin and virtually all flavonoid classes [11, 22].
The presence of hydroxyl groups attached to aromatic rings in their structures accounts for this feature. In addition to its antioxidant effects, rutin has been shown to chelate metal ions, preventing peroxidations brought on by them [23]. High-performance, thin-layer chromatography [19] and high-performance liquid chromatography [13, 14] are the most common chromatographic techniques used for quantitative analysis of rutin.
Rutin can be reacted with by some polyphenols, such as anthocyanins, as well as metal ions such as Mg (II) and Fe. Changes in the antioxidant capacity of the complexes demonstrated a synergistic effect due to the presence of non- essential nutrients [24]. In a mildly alkaline water solution, Mg (II) and Ca (II) ions promote rutin oxidation [25]. Adding rutin to curcumin can increase the latter’s bioavailability by facilitating curcumin’s interaction with human serum albumin [26]. Drugs like the antiplatelet medication tricagrelor can interact with rutin and other flavonoids by increasing the free trigagrelor levels in the plasma [27].
Quercetin and Cyclodextrin inclusion complexes have been shown to increase rutin’s solubility in water [28]. Nanoemulsions containing rutin or tocopheryl polyethylene glycol 1000 succinate (TPGS) can be used to increase rutin solubility, which is otherwise quite low [29]. Because of its disaccharide-glycosylated composition, rutin is poorly absorbed by intestinal membranes. Because of its substantial metabolism in the colon, it is likely that quercetin-mediated pharmacological effects are due to quercetin or rutin metabolites in the large intestine [2]. Furthermore, a dose of 200 mg/kg of rutin has been shown to protect mice against stomach injury brought on by ethanol [30]. This is because rutin has powerful antioxidant and protective qualities, including the ability to boost the antioxidant enzyme GSH- px’s activity and decrease lipoperoxide levels.
Metabolic Disorders
A metabolic disorder occurs when abnormal chemical reactions in your body disrupt this process. Some metabolic disorders are shown below:
Diabetes Mellitus
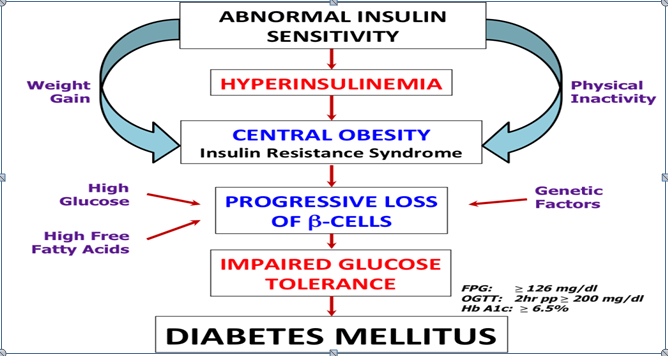
Diabetes mellitus is a term for a collection of diseases that affect glucose metabolism. For the cells that make up our muscles and tissues, glucose is a vital source of energy. It is also the primary fuel for the brain’s operations. Hyperglycemia during the fasting or postprandial phases is the diagnostic criteria for diabetes. Diabetes mellitus (DM) is characterised by persistent hyperglycemia, which is linked to damage, dysfunction, and failure in several end organs, such as the retina, kidney, neurons, heart, and blood vessels (Figure 3). There were 366 million people worldwide who had diabetes mellitus in 2011, according to the International Diabetes Federation (IDF), and that number is projected to climb to 552 million by the year 2030 [31].
A complete lack of insulin and an autoimmune response cause type 1 diabetes. Prior to the etiopathological categorization of diabetes mellitus, this condition was known as insulin-dependent diabetes mellitus (IDDM). The characteristic feature of the illness is the immune-mediated elimination of b cells, and hyperglycemia only occurs when 90% of b cells are lost [32].
Uncontrolled hyperglycemia can cause macro and micro vascular problems in the 4-7 years that type 2 DM patients go without a diagnosis. Fasting or random plasma glucose, as well as the DCCT-aligned HbA1c, are suitable screening assays. If there is any doubt, a 2-hour OGTT (oral glucose tolerance test) should be performed. In the presence of certain hematologic disorders, such as hemoglobinopathies, in which red blood cells are destroyed at an abnormally high rate, HbA1c should be avoided. The use of fasting plasma blood glucose or an oral glucose tolerance test (OGTT) can reduce the likelihood of a false-positive or false-negative result.
Wilson’s Disease
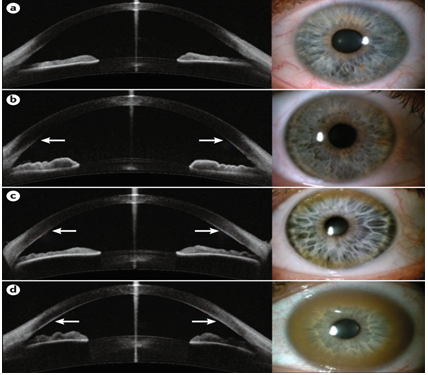
Wilson’s disease is a hereditary condition of copper metabolism that manifests in very severe hepatic and neurological symptoms (Figure 4). Kinnier Wilson first described the illness in 1912, and it affects between 30,000 and 1,000 people. Significant advancements have been made in the past two decades toward understanding the disease’s pathophysiology, cellular biology, and molecular genetics. Most people don’t start experiencing symptoms until their second or third decade. Because affected people excrete less copper through their bile, copper builds up in the liver. The most serious risk is that Wilson’s illness worsens over time, may go misdiagnosed, and is considered fatal if left untreated.
Since Wilson’s disease is inherited in an autosomal recessive fashion, it is quite likely that the index case will have a sibling who also suffers from the condition [33]. Mutation identification is useful in family screening once a patient with a homozygous or compound heterozygous ATP7B mutation has been identified as the “index patient.” The presence of the same genotype in asymptomatic family members validates the diagnosis, paving the way for treatment before difficulties arise. In cases where a family member’s clinical and biochemical traits are inconclusive, demonstrating heterozygosity (carrier status) or a wild-type gene sequence can spare them from unnecessary medication.
Gaucher’s Disease
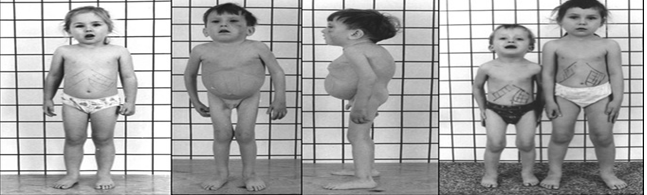
Gaucher’s disease is rare, obscure, and now incurable (Figure 5). It is a devastating condition. Jews have the highest prevalence of Gaucher’s disease in the general population. There is a high prevalence of Gaucher disease in India and elsewhere in the world. Any child or adult exhibiting the symptoms of splenomegaly, hepatic enlargement, and leukopenia (cytopenia) that are characteristic of the three forms of Gaucher disease should be evaluated for this condition. There are three different types of ALS: type 1 is the non-neuronopathic variant, and types 2 and 3 are neuronopathic varieties. Blood tests, including the glucocerebrosidase assay, provide a conclusive diagnosis. Bone marrow, liver, and spleen histology tests are not helpful in making a diagnosis of this disease. To confirm a diagnosis, check for the disease in family members, and predict the disease’s course, molecular investigations for mutations are extremely helpful. Only in cases where there is no other option, there is no response to enzyme replacement therapy, or a cure is unlikely, can a splenectomy be undertaken.
Gaucher disease often manifests in the skeleton and lungs, and splenectomy may make these conditions worse. Enzyme replacement therapy (ERT) has improved the outlook for individuals with this disease so much that it has become the gold standard of treatment. The best outcomes are reported in type 1 disease, with symptoms like splenomegaly, cytopenia, and bone pain all improving significantly. Care for the whole person is necessary while dealing with neurologic symptoms in type 3 disease. Growth, blood counts, liver and spleen size, and biomarkers like chitotriosidase that represent disease load are evaluated as part of monitoring patients on ERT. Although patients in India have thus far obtained the medicine through a philanthropic access programme, the government should make it easier for people to get therapy for this treatable illness. When the more expensive ERT is out of reach, bone marrow transplantation may be considered a last resort [34].
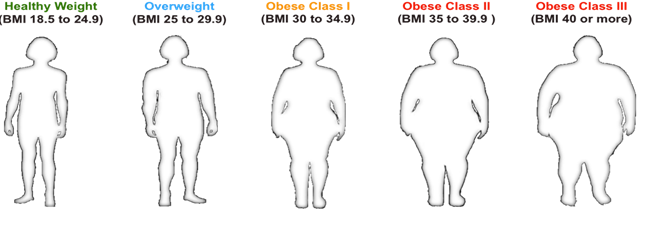
Obesity
The rising rates of obesity-related illnesses like diabetes, heart disease, hypertension, and cancer will strain health care systems if they aren’t addressed soon. The increased bulk of adipose tissue (Figure 6) and the enhanced production of pathogenetic products from larger fat cells are responsible for these consequences of obesity. The metabolic impacts of fat cells and the consequences of excess fat mass may be easily separated using this model of the pathophysiology of obesity as a disease. Social impairments caused by prejudice against those who are overweight, sleep apnea caused in part by extra fat in the parapharynx, and osteoarthritis brought on by the extra weight placed on one’s joints all fall into the latter category. The second group consists of metabolic processes linked to the far-reaching impacts of metabolites generated from larger fat cells. An increase in the release of fatty acids from fat cells and their subsequent storage in the liver or muscle may be responsible for the insulin-resistant condition that is prevalent in obesity. Diabetes occurs when the body’s insulin resistance is severe enough to overcome the pancreas’ ability to secrete insulin. The substantial link between increased fat, especially visceral fat, and diabetes makes this outcome particularly alarming for health care expenses. Excess fat cells may contribute to obesity’s proinflammatory condition by releasing cytokines like IL-6.
Along with changes in endothelial function, the procoagulant condition of obesity may contribute to the increased risk of cardiovascular disease and hypertension [35].
When the stromal mass is enlarged, it can produce estrogens, which may increase the risk of breast cancer. Increased cytokine release may have a role in different forms of proliferative proliferation. These pathogenetic effects of increasing fat deposits raise the likelihood that one’s life span will be reduced.
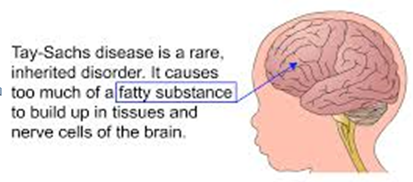
Tay-Sachs
Tay-Sachs disease is a type of lysosomal storage disorder that is passed down from parents to offspring in an autosomal recessive manner (Figure 7). Deficits in the enzyme hexosaminidase A (HexA) are the underlying cause of GM2-ganglioside buildup, most noticeably in the lysosomes of nerve cells. Mutations in the gene encoding the enzyme’s -subunit cause this deficiency. Acute neurodegeneration is a hallmark of Tay-Sachs, which is preceded by the activation of microglia, macrophages, and astrocytes, as well as the release of inflammatory mediators. The “infantile type” of the disease is typically diagnosed in infants, and it is one of the most severe forms of nervous system abnormalities. Also documented are the juvenile type, characterised by the development of symptoms during adolescence, and the rarest variant, characterised by the beginning of symptoms during adulthood.
Weak muscles, ataxia, trouble speaking, and mental disturbances are hallmarks of Tay-Sachs illness. The degree to which clinical symptoms persist is influenced by the remaining HexA enzymatic activity seen in some variants. Currently, Tay-Sachs disease treatment focuses on relieving symptoms and, for the late-onset variant, slowing the disease’s course. Clinical trials with miglustat plus bone marrow or hematopoietic stem cell transplantation as a substrate reduction treatment have also been reported.
There are now experimental gene therapy approaches for Tay-Sachs disease that involve the use of adeno- or adeno-associated viruses as vectors for the delivery of DNA encoding the and HexA subunit genes. Evaluation of this strategy is performed in the HexA subunit-deficient model mice or Jacob sheep, in which Tay-Sachs disease develops naturally and has the same clinical characteristics as in people. Possible new therapeutic approaches in Tay-Sachs disease therapy are discussed in this review with the goal of halting neurodegeneration and neuroinflammation [36].
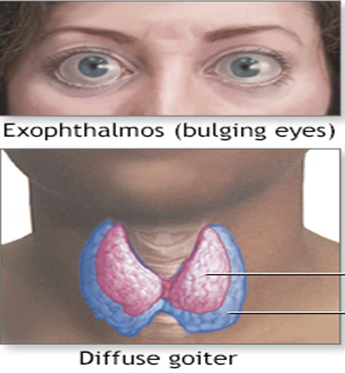
Hyperthyroidism
An overactive thyroid, also known as hyperthyroidism, arises when the thyroid gland generates an excessive amount of the hormone thyroxine. Hyperthyroidism speeds up the body’s metabolism, leading to unexpected weight loss and a fast or irregular heart rate (Figure 8).
Hyperthyroidism has multiple therapeutic options. Anti- thyroid drugs and radioactive iodine are used by doctors to reduce the body’s synthesis of thyroid hormones. Surgery to remove all or part of the thyroid gland is occasionally recommended for patients with hyperthyroidism. Hyperthyroidism is a condition that can have catastrophic consequences if left untreated; however, once detected and treated, most people experience a favourable outcome.
By increasing the heart rate and the cardiac output, as well as reducing the systemic vascular resistance, hyperthyroidism raises systolic blood pressure. Atrial arrhythmias (particularly atrial fibrillation), pulmonary hypertension, left ventricular hypertrophy, and heart failure may all develop as a result of hyperthyroidism. Patients with hyperthyroidism have a higher risk of developing hypertension than euthyroid individuals. Whether or not hyperthyroid patients have a reduced nighttime drop in ambulatory blood pressure is more debatable. In patients receiving treatment, systolic blood pressure, heart rate, and cardiac output all decrease [37].
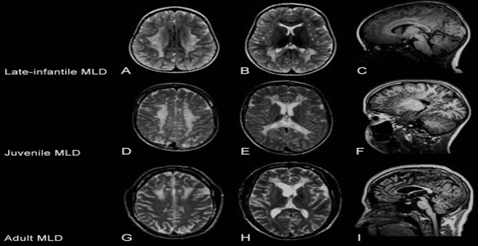
Metachromatic Leukodystrophy
Metachromatic leukodystrophy is an extremely rare genetic illness that leads to an accumulation of fatty substances (lipids) in cells, most notably those of the brain, spinal cord, and peripheral nerves (Figure 9). This accumulation is caused by a lack of the enzyme sulfatase, which aids in the breakdown of sulfatides, a type of lipid, as well as an inborn metabolic error caused by a lack of the enzyme arylsulfatase A (ASA). Sphingolipid 3-O-sulfogalactosylceramide (sulphatide) is the target of this enzyme, which catalyses the initial step in the sphingolipid’s breakdown process.
Some types of cells are the only ones that can express this membrane lipid. Myelin in the nervous system contains an especially high concentration of sulphatide—about 4% of all myelin lipids. Schwann cells in the periphery and oligodendrocytes in the CNS are responsible for myelin synthesis. Spirally wrapped around axons, myelin provides electrical insulation and facilitates rapid saltatory impulse conduction along the myelinated axon. Due to a lack of ASA, sulphate builds up in the body. In terms of functionality, this buildup is especially detrimental to the nervous system. Gall bladder epithelia and renal tubule storage cause minimal to no performance loss. Neurological symptoms are caused by demyelination, the clinical characteristic of the disease [38].
There are three distinct clinical presentations of the disease, each distinguished by the age at which symptoms first appear: the late-infantile form, in which symptoms appear between the ages of 2 and 3; the juvenile form, in which patients present between the ages of 3 and 16; and the adult-onset form, in which symptoms appear in patients aged 16 and up. Although this categorization is helpful in the clinic, it is arbitrary because there is a continuous range of disease severity. There is no cure for metachromatic leukodystrophy right now, but allogeneic bone marrow transplantation may help people who got the disease as a child or as an adult.
Maple Syrup Urine Disease (MSUD)
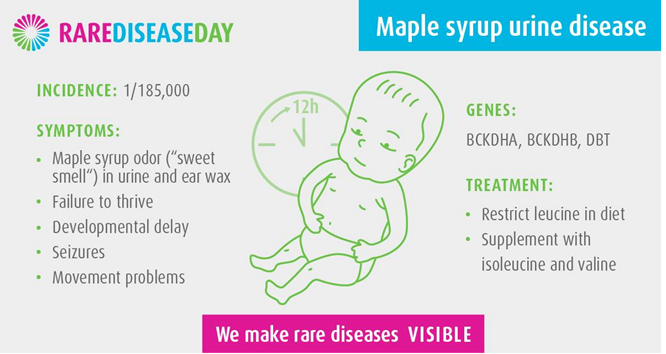
A disease characterized by urine that smells like maple syrup is called maple syrup urine disease (MSUD). Inability to metabolize specific amino acids (proteins’ “building blocks”) leads to potentially hazardous accumulations in the blood and urine (Figure 10).
Defects in the branched-chain ketoacidosis dehydrogenase complex are the underlying cause of maple syrup urine disease (MSUD), a metabolic disorder characterized by increased levels of branched-chain amino acids (BCAAs) in the blood and urine as well as the production of the pathognomonic disease marker, all isoleucine. There is no established link between genotype and the disorder’s five identified clinical variations, which span a wide range of symptoms and manifestations. Developmental delay, failure to thrive, feeding difficulties, and a maple syrup odor in the crewmen and urine are the hallmark newborn symptoms; if ignored, these symptoms can progress to stereotyped motions, metabolic decompensating, and death. Therapeutic measures include a reduction in dietary BCAA intake and careful monitoring of metabolic processes. If treatment is started quickly, it usually has a positive effect on the patient’s health. MSUD screening of newborns is increasingly standard and part of the Recommended Uniform Screening Panel in the United States (RUSP) [39].
Pharmacological Activities
Rutin has various pharmacological activities such as antiplatlet, Type 2 diabetes, obesity, anticarcinogenic, neuroprotective, skin aging as shown in (figure 11).
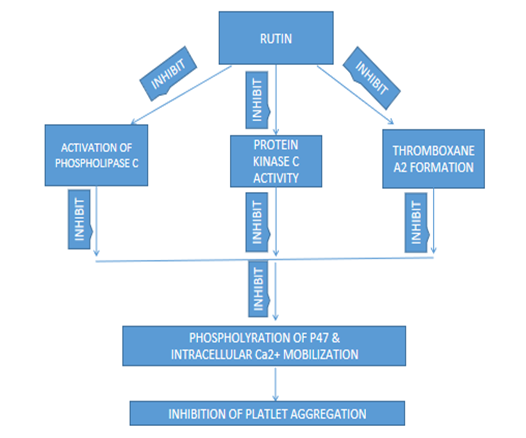
Mechanism of Rutin of Antiplatlet
Rutin concentration-dependently (250 and 290 µM) reduced platelet aggregation in human platelets triggered by agonists (i.e, collagen) (i.e, collagen). The binding of FITC-triflavin to the glycoprotein IIb/IIIa complex in human platelets was not significantly affected by rutin (250 and 290 M). When collagen activated human platelets, rutin (250 and 290 M) significantly suppressed intracellular Ca2+ mobilization and thromboxane A2 production. Collagen (1 g/mL) induced the rapid phosphorylation of Mr 47000 platelet protein (P47), a hallmark of protein kinase C activity. The addition of rutin (250 and 290 M) significantly reduced this phosphorylation [40]. Contrarily, platelet cyclic AMP and nitric oxide/cyclic GMP production were not noticeably impacted by rutin (250 and 290 M). In conclusion, our results imply that the antiplatelet action of rutin may entail the following pathways: Fig. a shows that rutin prevented platelet aggregation by blocking phospholipase C activation, which in turn blocked protein kinase C activity and thromboxane A2 production, which blocked phosphorylation of P47 and intracellular Ca2+ mobilization (Figure 12).
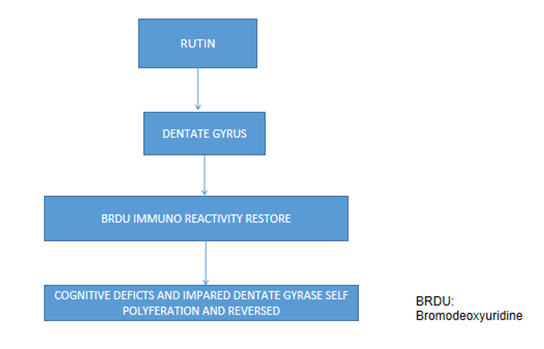
Mechanism of Rutin of Neuroprotective
Neuroprotective and memory-enhancing effects of okra (Abelmoschus esculentus Linn) extract and rutin derivatives in dexamethasone-treated rats. The Morris water maze test was used to assess the capacity of mice to learn and remember new information [41]. The results demonstrated that dexamethasone-treated mice spent less time in the correct quadrant of the water maze compared to mice pretreated with either rutin or okra extract. Pyramidal neurons in the dexamethasone group appeared to have undergone some morphological alterations. CA3 hippocampal neuron count was considerably reduced; pretreatment with, rutin, or okra mitigated this effect. Hippocampal NMDA receptor expression was modified after prolonged dexamethasone administration. To counteract this decrease in NMDA receptor expression, pretreatment with, rutin, or okra extract was necessary. Using the immunohistochemical method, the authors looked at the proliferation of cells in the dentate gyrus (DG) with the use of 5-bromo-2-deoxyuridine (BrdU). Compared to untreated mice, dexamethasone- treated mice had a marked decrease in the percentage of their cells that tested positive for the BrdU antigen. Rutin, when combined with okra extract, was found to restore BrdU-immunoreactivity in the dentate gyrus. It appears that rutin and okra extract treatments prevented morphological alterations in the CA3 region and improved cognitive deficits in dexamethasone-treated mice, specifically reduced dentate gyrus (DG) cell proliferation (Figure 13).
Mechanism of Rutin of Type 2 Diabetes.
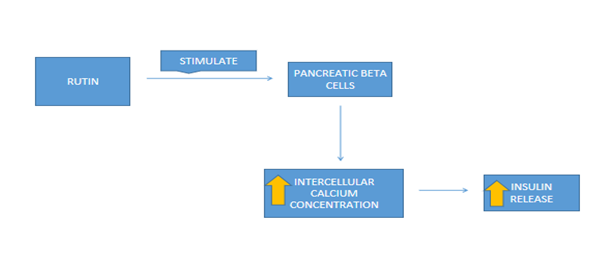
Potential mechanisms for rutin’s hypoglycemic effects are depicted in (Figure 14). The research shows that rutin inhibits the enzymes alpha-glucosidase and alpha-amylase, which are responsible for breaking down carbohydrates in the small intestine [42, 43, 44]. While rutin’s effect on isomaltase inhibition was more than that of acarbose, it was greater for maltase and glucoamylase. As a result of being able to slow down the intestinal absorption of glucose, post-meal blood sugar levels don’t spike as high. Reducing blood sugar levels can also be accomplished by boosting tissue glucose absorption and beta cell insulin release. Isolated rat pancreatic islets were treated with rutin, and the result was a dramatic rise in insulin output [45]. Rutin improved glucose-induced insulin production and maintained glucose sensing abilities in rat beta cells exposed to high glucose [46]. Insulin-mimetic effects of rutin were also observed in the soleus and diaphragm muscles of rats [47, 48]. Muscle glucose transport was increased because GLUT-4 production and translocation were promoted. As with insulin, rutin’s stimulatory action on tissue glucose uptake is the result of intracellular transduction involving phosphoinositide 3-kinase (PI3K), protein kinase C, and mitogen-activated protein kinase (MAPK) [49, 50].
Mechanism of Rutin of Skin Aging
Fine creases, thin and transparent skin, loss of underlying fat resulting in hollowed cheeks and eye sockets, dry and itchy skin, lack of sufficient sweat, hair greying, hair loss or hirsutism, and thinning of the nail plates are all clinical symptoms of ageing [51]. It is generally agreed that free radicals and reactive oxygen species (ROS) cause the majority of the damage to essential cellular macromolecules that contribute to intrinsic ageing. Both ROS production and the capacity of human skin cells to repair DNA damage decline significantly with age [52]. Free radical oxygen species (ROS) contribute significantly to skin ageing. About 1.5%-5% of the oxygen used by the skin is transformed into ROS by endogenous pathways [53]. Reactive oxygen species (ROS) are constantly created as byproducts of the electron transport chain of aerobic metabolism in the mitochondria and are thought to be the primary cause of intrinsic ageing [54]. Mitochondrial reactive oxygen species (ROS) are mostly produced by keratinocytes and fibroblasts in the skin.
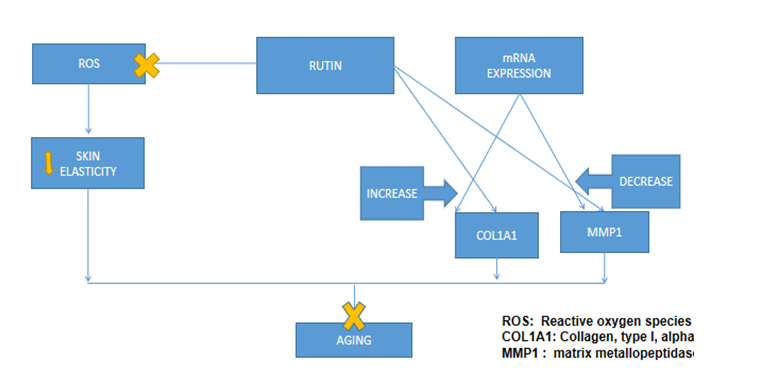
As can be seen in (Figure 15), rutin induced a rise in the mRNA expression of collagen type I alpha 1 (COL1A1) and a fall in the expression of matrix metalloproteinase 1 (MMP1) in HDFs. We found that rutin protected cells from oxidative stress and that it increased ROS scavenging activity in a dose-dependent way. Additionally, rutin improved skin suppleness and reduced wrinkle length, area, and quantity. Wrinkles, sagging, and loss of suppleness are some of the most noticeable signs of ageing in humans [55]. Overall, the results of this investigation showed that rutin has biological effects on ROS-induced skin ageing. This work provides more evidence that rutin slows the ageing process of skin by increasing dermal density and flexibility via modulation of enzymes in the extracellular matrix (ECM).
Mechanism of Rutin Ameliorates Obesity through Brown Fat Activation
Obesity has skyrocketed in prevalence over the past few decades, and is now a major health issue all across the world [56]. As previously mentioned, cardiovascular disease, type 2 diabetes mellitus, high blood pressure, cancer, and other connected disorders are all linked to obesity [57]. White adipose tissue (WAT) is where extra energy is deposited as triglycerides when caloric intake exceeds energy expenditure, leading to obesity [58]. Obesity is far from being adequately addressed by the current antiobesity treatments, which try to limit energy intake and absorption. Therefore, an alternative technique to boost energy expenditure in critical metabolic organs such brown adipose tissue (BAT) is urgently required [59].
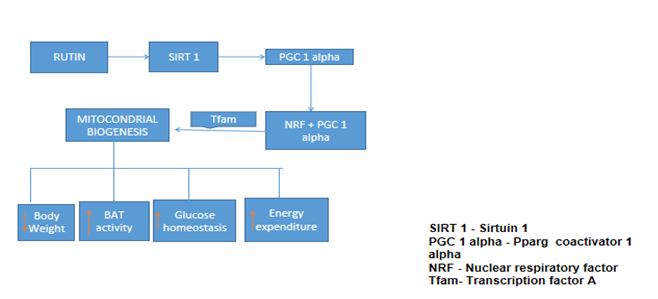
Brown adipose tissue (BAT) activation, which leads to increased energy expenditure, is an important strategy for combating obesity and 2 types of diabetes. In this research, rutin, a chemical derived from the mulberry fruit that has been safely used in the clinic for decades to strengthen blood vessels, regulated systemic energy metabolism by increasing BAT activity. Diet-induced obesity (DIO) mice and genetically obese (Db/Db) mice both benefited from rutin therapy, which dramatically decreased adiposity, increased energy expenditure, and improved glucose homeostasis. Subcutaneous adipose tissue in both obesity mouse models showed increased numbers of brown adipocytes (beige) after treatment with rutin. As for the mechanism, we discovered that rutin directly bound to and stabilized SIRT1, which in turn hypo acetylated peroxisome proliferator-activated receptor g coactivator-1a protein, which in turn stimulated Tfam transactivation and, ultimately, increased the number of mitochondria and UCP1 (mitochondrial uncoupling protein 1) activity in BAT [60]. These results demonstrate that rutin is an unusual tiny chemical that activates BAT and suggests a potential new therapeutic approach for treating metabolic diseases (Figure 16).
Mechanism of Rutin of Carcinogenic
The term “cancer” refers to a group of diseases characterized by the uncontrolled proliferation of aberrant cells that may invade neighboring tissues or metastasize to other parts of the body. Overexpression of oncogenes, loss of genomic stability, mutations (genetic or epigenetic), the tumor microenvironment, intracellular signaling cascades, and the absence of apoptosis are only some of the mechanisms that have been the focus of intensive study recently [61, 62].
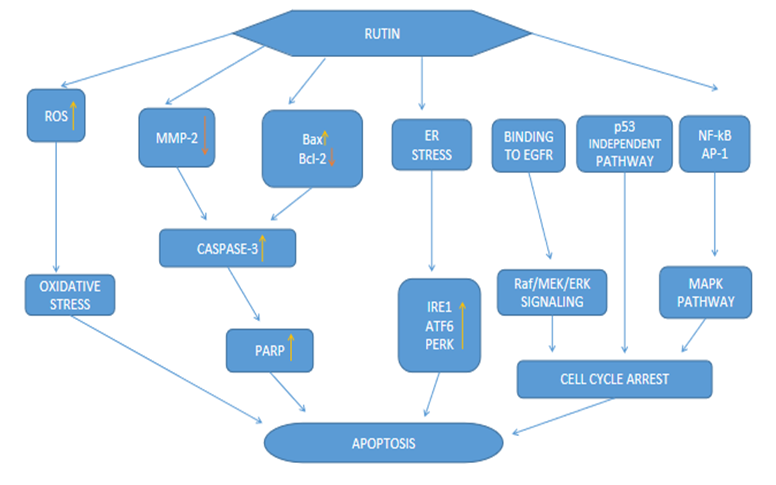
Recent studies have shown that rutin can regulate the molecular mechanisms that lead to the death of cancer cells. Evidence in the field of rutin can be broken down into three categories: in vitro research, in vivo studies, and clinical investigations, each of which contributes to the state of the art. While rutin’s efficacy against cancer has been well- documented, how it stacks up against other natural agents has not. Further research into the benefits of rutin over other natural compounds with anticancer activity including curcumin, zerumbone, thymoquinone, honokiol, escin, pinitol, tocotreinols, isorhamnetin, etc, was recommended [63, 64, 65, 66, 67, 68, 69, 70] (Figure 17), depicts the molecular mechanism and the mode of action of rutin’s anticancer impact.
Significant anti-cancer activity against MDA-MB-231 cells is attributed to rutin [71]. The DNA of human hepatocellular carcinoma (HTC) cells has been found to be protected by rutin against exposure to pro-carcinogens [72]. Modulation of Wnt, JAK- STAT, and EGF signaling by rutin, as well as AP-1, NF- B, and Akt, are just a few of the topics that might be explored in this context. In addition, the mechanism of rutin that initiates the ER stress-induced reaction is studied in detail in order to learn how apoptosis is generated in malignant cells.
Conclusion
The present study was designed to investigate the effects of rutin on different metabolic disorders. Rutin was found active against obesity, antiplatelet, skin aging type 2diabetes / prediabetes, carcinogenic, neuroprotective. However, the precise cellular mechanisms leading to curative effects of rutin on many other metabolic disorders like liver diseases such as nonalcoholic steatohepatitis, kidney diseases , are unknown , so more studies are required if those mechanism are to be identified.
Refrences
1. Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL (2017) Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Ther Adv Cardiovasc Dis 11(8): 215-225.
2. Frutos MJ, Rincon-Frutos L, Valero-Cases E (2019) Rutin.s Nonvitamin and Nonmineral Nutritional Supplements. Elsevier pp: 111-117.
3. Nieoczym D, Socala K, Raszewski G, Wlaz P (2014) Effect of quercetin and rutin in some acute seizure models in mice. Progress in Neuro-Psychopharmacology and Biological Psychiatry 54: 50-58.
4. Havsteen BH (2002) The biochemistry and medical significance of the flavonoids. Pharmacol Ther 96(2-3): 67-202.
5. Fernandez SP, Wasowski C, Loscalzo LM, Granger RE, Johnston GAR, et al. (2006) Central nervous system depressant action of flavonoid glycosides. Eur J Pharmacol 539(3): 168-176.
6. Dajas F, Andres AC, Felicia CE (2013) Neuroprotective actions of flavones and flavonols: mechanisms and relationship to flavonoid structural features. Cent Nerv Syst Agents Med Chem 13(1): 30-35.
7. Lee BH, Hwang SH, Choi SH, Shin TJ, Kang J, et al. (2011) Quercetin inhibits alpha3beta4 Nicotinic acetylcholine receptor-mediated ion currents expressed in Xenopus oocytes. Korean J Physiol Pharmacol 15(1): 17-22.
8. Nassiri-Asl M, Shariati-Rad S, Zamansoltani F (2008) Anticonvulsive effects of intracerebroventricular administration of rutin in rats. Prog Neuropsychopharmacol Biol Psychiatry 720: 989-993
9. Cheng H, Ye XP Y, Jiang Z, Zhou P (2007) Quercetin subunit specifically reduces GlyR- mediated current in rat hippocampal neurons. Neuroscience 148(2): 548- 559.
10. Williams RJ, Spencer JP, Evans CR (2004) Flavonoids: antioxidants or signalling molecules? Free Radic Biol Med 36: 838-849.
11. Marin FR, Frutos MJ, Alvarez JAP, Sanchez FM, Rio JAD (2002) Flavonoids as nutraceuticals: Structural related antioxidant properties and their role on ascorbic acid preservation. Studies in natural Products 26: 741-778.
12. Kreft I, Fabjan N, Yasumoto K (2006) Rutin content in buckwheat (Fagopyrum esculentum Moench) food materials and products. Food Chem 98(3): 508-512.
13. Iacopini P, Baldi M, Storchi P, Sebastiani L (2008) Catechin, epicatechin, quercetin, rutin and resveratrol in red grape: Content, in vitro antioxidant activity and interactions. J Food Compost Anal 21(8): 589-598.
14. Glavac NK, Stojilkovski K, Kreft S, Park CH, Kreft I (2017) Determination of fagopyrins, rutin, and quercetin in Tartary buckwheat products. Lebenson Wiss Technol 79: 423-427.
15. Fabjan N, Rode J, Kosir IJ, Wang Z, Zhang Z, et al. (2003) Tartary buckwheat (Fagopyrum tataricum Gaertn.) as a source of dietary rutin and quercitrin. J Agric Food Chem 51(22): 6452-6455.
16. Kreft I, Skrabanja V (2002) Nutritional properties of starch in buckwheat noodles. J Nutr Sci Vitaminol (Tokyo) 48(1): 47-50.
17. Motoki S, Kitazawa H, Maeda T, Suzuki T, Chiji H, Nishihara E, et al. (2012) Effects of various asparagus production methods on rutin and protodioscin contents in spears and cladophylls. Biosci Biotechnol Biochem 76(5): 1047-1450.
18. Kalinova J, Dadakova E (2009) Rutin and total quercetin content in amaranth (Amaranthus spp.). Plant Foods Hum Nutr 64(1): 68-74.
19. Alam P, Parvez MK, Arbab AH, Al-Dosari MS (2017) Quantitative analysis of rutin, quercetin, naringenin, and gallic acid by validated RP- and NP-HPTLC methods for quality control of anti-HBV active extract of Guiera senegalensis. Pharm Biol 55(1): 1317-1323.
20. Rozema J, Bjorn LO, Bornman JF, Gaberscik A, Hader DP, et al. (2002) The role of UV-B radiation in aquatic and terrestrial ecosystems--an experimental and functional analysis of the evolution of UV-absorbing compounds. J Photochem Photobiol B 66(1): 2-12.
21. Shen SC, Lee WR, Lin HY, Huang HC, Ko CH, et al. (2002) In vitro and in vivo inhibitory activities of rutin, wogonin, and quercetin on lipopolysaccharide-induced nitric oxide and prostaglandin E2 production. Eur J Pharmacol 446(1-3): 187-94.
22. Tapas AR, Sakarkar DM, Kakde RB (2008) Flavonoids as Nutraceuticals: A Review. Trop J Pharm Res 7(3): 1089- 1099.
23. Lue BM, Nielsen NS, Jacobsen C, Hellgren L, Guo Z, et al. (2010) Antioxidant properties of modified rutin esters by DPPH, reducing power, iron chelation and human low density lipoprotein assays. Food Chem 123(2): 221-230.
24. Qian BJ, Wu CF, Lu MM, Xu W, Jing P (2017) Effect of complexes of cyanidin-3-diglucoside-5-glucoside with rutin and metal ions on their antioxidant activities. Food Chem 232: 545-551.
25. Zivanovic SC, Nikolic RS, Nikolic GM (2016) The influence of Mg(II) and Ca(II) ions on rutin autoxidation in weakly alkaline aqueous solutions. Acta Fac medicae Naissensis 33(3): 163-171.
26. Liu BM, Zhang J, Hao AJ, Xu L, Wang D, et al. (2016) The increased binding affinity of curcumin with human serum albumin in the presence of rutin and baicalin: A potential for drug delivery system. Spectrochim Acta A Mol Biomol Spectrosc 155: 88-94.
27. Liu BM, Zhang J, Bai CL, Wang X, Qiu XZ, et al. (2015) Spectroscopic study on flavonoid–drug interactions: Competitive binding for human serum albumin between three flavonoid compounds and ticagrelor, a new antiplatelet drug. J Lumin 168: 69-76.
28. Sri KV, Kondaiah A, Ratna JV, Annapurna A (2007) Preparation and characterization of quercetin and rutin cyclodextrin inclusion complexes. Drug Dev Ind Pharm 33(3): 245-53.
29. Macedo AS, Quelhas S, Silva AM, Souto EB (2014) Nanoemulsions for delivery of flavonoids: formulation and in vitro release of rutin as model drug. Pharm Dev Technol 19(6): 677-680.
30. Casa CL, Villegas I, Lastra CADL, Motilva V, Calero MJM (2000) Evidence for protective and antioxidant properties of rutin, a natural flavone, against ethanol induced gastric lesions. J Ethnopharmacol 71(1-2): 45- 53.
31. Whiting DR, Guariguata L, Weil C, Shaw J (2011) IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract 94(3): 311-321.
32. Alam U, Asghar O, Azmi S, Malik RA (2014) General aspects of diabetes mellitus. Handb Clin Neurol 126: 211-222.
33. Ala A, Walker AP, Ashkan K, Dooley JS, Schilsky ML (2007) Wilson’s disease. Lancet 369(9559): 397-408.
34. Nagral A (2014) Gaucher disease. J Clin Exp Hepatol 4(1): 37-50.
35. Bray GA (2004) Medical consequences of obesity. J Clin Endocrinol Metab 89(6): 2583-2589.
36. Solovyeva VV, Shaimardanova AA, Chulpanova DS, Kitaeva KV, Chakrabarti L, et al. (2018) New approaches to Tay-Sachs disease therapy. Front Physiol 9: 1663.
37. Prisant LM, Gujral JS, Mulloy AL (2006) Hyperthyroidism: a secondary cause of isolated systolic hypertension. J Clin Hypertens (Greenwich) 8(8): 596-599.
38. Gieselmann V (2008) Metachromatic leukodystrophy: genetics, pathogenesis and therapeutic options. Acta Paediatr 97(457): 15-21.
39. Blackburn P, Gass J, Vairo FPE, Farnham K, Atwal H, et al. (2017) Maple syrup urine disease: mechanisms and management. Appl Clin Genet 10: 57-66.
40. Sheu JR, Hsiao G, Chou PH, Shen MY, Chou DS (2004) Mechanisms involved in the antiplatelet activity of rutin, a glycoside of the flavonol quercetin, in human platelets. J Agric Food Chem 52(14): 4414-4418.
41. Tongjaroenbuangam W, Ruksee N, Chantiratikul P, Pakdeenarong N, Kongbuntad W, et al. (2011) Neuroprotective effects of quercetin, rutin and okra (Abelmoschus esculentus Linn.) in dexamethasone- treated mice. Neurochem Int 59(5): 677-685.
42. Jadhav R, Puchchakayala G (2012) Hypoglycemic and antidiabetic activity of flavonoids: boswellic acid, ellagic acid, quercetin, rutin on streptozotocin-nicotinamide induced type 2 diabetic rats. Int J Pharm Pharm Sci 4(2): 251-256.
43. Ghorbani A (2013) Phytotherapy for diabetic dyslipidemia: evidence from clinical trials. Clin Lipidol 8(3): 311-319.
44. Li YQ, Zhou FC, Gao F, Bian JS, Shan F (2009) Comparative evaluation of quercetin, isoquercetin and rutin as inhibitors of alpha-glucosidase. J Agric Food Chem 57(24): 11463-11468.
45. Esmaeili MA, Zohari F, Sadeghi H (2009) Antioxidant and protective effects of major flavonoids from Teucrium polium on beta-cell destruction in a model of streptozotocin-induced diabetes. Planta Med 75(13): 1418-1420.
46. Cai EP, Lin JK (2009) Epigallocatechin gallate (EGCG) and rutin suppress the glucotoxicity through activating IRS2 and AMPK signaling in rat pancreatic beta cells. J Agric Food Chem 57(20): 9817-9827.
47. Ahmed OM, Moneim AA, Yazid IA, Mahmoud AM (2010) Antihyperglycemic, antihyperlipidemic and antioxidant effects and the probable mechanisms of action of Ruta graveolens infusion and rutin in nicotinamide- streptozotocin-induced diabetic rats. Diabetol Croat 39(1): 15-35.
48. Kappel VD, Cazarolli LH, Pereira DF, Postal BG, Zamoner A, et al. (2013) Involvement of GLUT-4 in the stimulatory effect of rutin on glucose uptake in rat soleus muscle. J Pharm Pharmacol 65(8): 1179-1186.
49. Khan AH, Pessin JE (2002) Insulin regulation of glucose uptake: a complex interplay of intracellular signalling pathways. Diabetologia 45(11): 1475-1483.
50. Ghorbani A (2017) Mechanisms of antidiabetic effects of flavonoid rutin. Biomed Pharmacother 96: 305-312.
51. Zouboulis CC, Makrantonaki E (2011) Clinical aspects and molecular diagnostics of skin aging. Clin Dermatol 29(1): 3-14.
52. Pons B, Belmont AS, Genteuil GM, Chapuis V, Oddos T, et al. (2010) Age-associated modifications of Base Excision Repair activities in human skin fibroblast extracts. Mech Ageing Dev 131(11-12): 661-665.
53. Poljsak B, Dahmane RG, Godic A (2012) Intrinsic skin aging: the role of oxidative stress. Acta Dermatovenerol Alp Panonica Adriat 21(2): 33-36.
54. Farage MA, Miller KW, Elsner P, Maibach HI (2008) Intrinsic and extrinsic factors in skin ageing: a review.
Int J Cosmet Sci 30(2): 87-95.
55. Choi SJ, Lee SN, Kim K, Joo DH, Shin S, et al. (2016) Biological effects of rutin on skin aging. Int J Mol Med 38(1): 357-363.
56. Bray GA (2004) Medical consequences of obesity. J Clin Endocrinol Metab 89(6): 2583-2589.
57. Jin W, Patti ME (2009) Genetic determinants and molecular pathways in the pathogenesis of Type 2 diabetes. Clin Sci (Lond) 116(2): 99-111.
58. Lowell BB, Spiegelman BM (2000) Towards a molecular understanding of adaptive thermogenesis. Nature 404(6778): 652-660.
59. Ravussin E, Galgani JE (2011) The implication of brown adipose tissue for humans. Annu Rev Nutr 31(1): 33-47.
60. Yuan X, Wei G, You Y, Huang Y, Lee HJ, et al. (2017) Rutin ameliorates obesity through brown fat activation. FASEB J 31(1): 333-345.
61. Kim K, Hu W, Audenet F, Almassi N, Hanrahan AJ, et al. (2020) Modeling biological and genetic diversity in upper tract urothelial carcinoma with patient derived xenografts. Nat Commun 11(1): 1975.
62. Teh BT, Fearon ER (2020) Genetic and Epigenetic Alterations in Cancer. In: Abeloff’s Clinical Oncology. Elsevier 2020: 209-224.e2.
63. Mirzaie V, Ansari M, Mahani SNN, Nasery MM, Karimi B, et al. (2020) Nano-graphene oxide-supported APTES- spermine, as gene delivery system, for transfection of pEGFP-p53 into breast cancer cell lines. Drug Des Devel Ther 14: 3087-3097.
64. Prasannan R, Kalesh KA, Shanmugam MK, Nachiyappan A, Ramachandran L, et al. (2012) Key cell signaling pathways modulated by zerumbone: role in the prevention and treatment of cancer. Biochem Pharmacol 84(10): 1268-1276.
65. Rajendran P, Li F, Shanmugam MK, Vali S, Abbasi T, et al. (2012) Honokiol inhibits signal transducer and activator of transcription-3 signaling, proliferation, and survival of hepatocellular carcinoma cells via the protein tyrosine phosphatase SHP-1. J Cell Physiol 227(5): 2184-2195.
66. Ramachandran L, Manu KA, Shanmugam MK, Li F, Siveen KS, et al. (2012) Isorhamnetin inhibits proliferation and invasion and induces apoptosis through the modulation of peroxisome proliferator-activated receptor γ activation pathway in gastric cancer. J Biol Chem 287(45): 38028-38040.
67. Sethi G, Ahn KS, Sung B, Aggarwal BB (2008) Pinitol targets nuclear factor-κB activation pathway leading to inhibition of gene products associated with proliferation, apoptosis, invasion, and angiogenesis. Molecular Cancer Therapeutics 7(6): 1604-1161.
68. Tan SML, Li F, Rajendran P, Kumar AP, Hui KM, et al. (2010) Identification of β-escin as a novel inhibitor of signal transducer and activator of transcription 3/Janus- activated kinase 2 signaling pathway that suppresses proliferation and induces apoptosis in human hepatocellular carcinoma cells. Journal of Pharmacology and Experimental Therapeutics 334(1): 285-293.
69. Siveen KS, Ahn KS, Ong TH, Shanmugam MK, Li F, et al. (2014) Y-tocotrienol inhibits angiogenesis-dependent growth of human hepatocellular carcinoma through abrogation of AKT/mTOR pathway in an orthotopic mouse model. Oncotarget 5(7): 1897-1911.
70. Siveen KS, Mustafa N, Li F, Kannaiyan R, Ahn KS, et al. (2014) Thymoquinone overcomes chemoresistance and enhances the anticancer effects of bortezomib through abrogation of NF-κB regulated gene products in multiple myeloma xenograft mouse model. Oncotarget 5(3): 634- 648.
71. Ghasemzadeh A, Jaafar HZ, Rahmat A, Devarajan T (2014) Evaluation of bioactive compounds, pharmaceutical quality, and anticancer activity of curry leaf (Murraya koenigii L.). Evid Based Complement Alternat Med 2014: 873803.
72. Marcarini JC, Tsuboy MSF, Luiz RC, Ribeiro LR, Campo CBH, et al. (2011) Investigation of cytotoxic, apoptosis- inducing, genotoxic and protective effects of the flavonoid rutin in HTC hepatic cells. Exp Toxicol Pathol 63(5): 459-465.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State