Comparative Pharmacokinetic Studies of Marketed Gel and Transdermal Patches Loaded with Diclofenac Diethylamine in Rabbits
Oral administration of the non-steroidal anti-inflammatory drug, Diclofenac diethylamine (DDEA) is often associated with gastrointestinal ulcers, extensive first-pass hepatic metabolism, and gastric bleeding. As an alternative to oral administration, a transdermal drug delivery system (TDDS) of DDEA was developed for topical administration, to quantify diclofenac diethylamine in plasma of rabbits for this, a sensitive Reverse Phase-high performance liquid chromatography (RP-HPLC) method was developed to compare DDEA in marketed gel and optimized formulation, using Carbamazepine as Internal standard (IS). DDEA provoke on Hypersil RP C18 column (250 mm × 4.6 mm 5 μm) using a mobile phase mixture of potassium dihydrogen buffer pH 2.5 and acetonitrile in the ratio of 30:70v/v at an isocratic flow rate of 1mL/min. The retention time of DDEA was found to be 5.3min. The calibration curve was linear over the concentration range from 50-750ng/mL of DDEA. This method was accurate for quantitative estimation of the drug in marketed gel and optimized formulation. The main aim of study is to compare Pharmacokinetic profile of diclofenac diethylamine in pharmaceutical dosage forms (Marketed gel & formulated transdermal patches) using WinNonlin software version 8.1.
Introduction
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) have been extensively used in the treatment of rheumatoid arthritis and other related conditions. However, they carry the risk of adverse systemic side effects and gastrointestinal irritation at the usual dose of oral administration [1]. Topical and transdermal products are vital classes of drug delivery systems and their use of therapy becoming more common as they offer many increased patient acceptability (non- invasiveness), avoidance of gastrointestinal disturbances, and first-pass metabolism of the drug. Diclofenac is a nonsteroidal anti-inflammatory agent, widely used in musculoskeletal disorders, arthritis, for symptomatic relief of pain and inflammation [2]. Diclofenac diethylamine (DDEA) is a novel NSAID of the aryl-acetic acid class. It is chemically 2-{2-[(2, 6-dichloro phenyl) amino] phenyl} acetic acid is a white crystalline powder, amphiphilic in nature, sparingly soluble in water and acetone, freely soluble in ethanol and methanol. Diclofenac diethylammonium inhibits cyclooxygenase (COX-1 and -2), which is responsible for production of prostaglandin and is used in the treatment of local pain, inflammation, soft tissue rheumatism, and degeneration of inflammatory lesions of the tendons, ligaments, and joints [3]. Due to oral administration of DDEA, it has increased risk of serious to fatal cardiovascular events, heart attack or stroke, ulcers and perforation in the stomach and intestine. It has analgesic and anti-inflammatory property and effective in relieving symptoms of muscle aches, backaches, dysmenorrhea, dental pain, menstrual cramps and sports injuries [4].
A few types of research are reported determination of DDEA concentration in rabbit study using the HPLC method. The present investigation by the author explains the pharmacokinetic profile of prepared diclofenac diethylamine patches in rabbit compared with marketed gel, this type of prepared dosage form by using design expert is suitable for its unique property of penetration into skin barriers to reach joints muscles and synovial fluid due to the presence of diethylammonium salts of diclofenac owing to its lipophilic nature as shown in Figure 1, topical application of patch is more suitable for geriatric patients with increased patients acceptability [5].
Material and Method
Diclofenac Diethylamine was a gift sample from Santa Cruz, Mumbai. India and Carbamazepine were obtained as a gift sample from Vasudha Pharma, Chem. Ltd., India. KH2PO4 (Potassium dihydrogen phosphate), Orthophosphoric acid (OPA) and Acetonitrile was procured from Merck, Mumbai. Water for HPLC was procured from Sigma-Aldrich Chem Pvt. Ltd., Bangalore. Animal Ethical Committee has approved the study, and the studies were piloted in accordance with standard institutional guidelines.
Surgical blade, cotton adsorbent, gauze needle, syringe, Gloves, 1.5 mL Eppendorf tubes, Whatman filter paper, Buffers pH 2.5, 5.0, C18 column, Triethanolamine (TEA), K3EDTA tubes, Cyclomixer (Remi Model cm101. LC software solutions 2.1 version. Marketed Gel (ALKEM Laboratories, Mumbai). Centrifuge (Model R-8C, Remi Elektrotechnik, and Vasai, India).
Preparation of Optimized Formulation of DDEA Patch
Matrix type of Diclofenac Diethylamine transdermal patch was optimized (P3) by design expert software for its required flux to elicit Pharmacological action. The method involved in preparation of transdermal patch is by solvent diffusion technique, using 200mg of Hydroxy Propyl Methyl Cellulose E-15 (HPMC E-15) dissolved in solvent system containing 1:1 ratio of ethanol and dichloromethane, allowed to soak for 12hrs. Experiments was continued after the requested time under stirring with magnetic stirrer then the 500 mg of DDEA was added to the polymeric solution, with 10% v/w of plasticizer (PEG-400), followed by addition of 12% v/w permeation enhancer as Dimethyl sulphoxides (DMSO) and casted on anumbra Petri plates with surface area of 32.153 cm2. 500mg of DDEA is dispersed in 32.153cm2 area of patch, to this calculation desired radius of patch of 1.08cm was cut into pieces in which, each patch contains 58mg of DDEA, equivalent to 50 mg of diclofenac.
Preparation of Buffer and Internal Standard
10mM Potassium dihydrogen orthophosphate was prepared by taking 0.272 mg of KH2PO4 in 200 mL of HPLC water, sonication is required for complete dissolution of KH2PO4, and still, particles are removed by filtration through filter paper with a pore size of 0.45 µm (Spectrum laboratories). Further buffer is adjusted to pH 2.5 with orthophosphoric acid and triethanolamine [6]. Accurately weighed 10 mg of carbamazepine as Internal standard (IS) was transferred into 100 mL the volumetric flask containing 10mL of acetonitrile (HPLC grade) and sonicate for about 10 mins. The volume was made up to the mark with acetonitrile. The stock solution was further diluted with mobile phase to give the final concentration of 1000ng/mL of each [7].
Preparation of Mobile Phase
Mobile phase was prepared by mixing acetonitrile and freshly prepared 10 mM KH2PO4 by using distilled water in the ratio of 70:30 v/v, the mobile phase was filtered through 0.45 µm membrane filter and was degassed with the help of a bath sonicator [8] (Ultrasonic)
Detection of Peak
From the various trails of Internal standard and drug concentration, the optimized standard concentrations of Internal standard (carbamazepine) 1000 ng/mL and pure drug 100ng/mL was dissolved in a similar solvent and injected into HPLC to elute the peak, for identification of individual peaks of ACN, Carbamazepine (Internal standard), and DDEA (pure drug).
Chromatographic Conditions
The chromatographic system consists of a Shimadzu LC (Liquid chromatography)-20AD Toyoko Japan, solvent delivery pump equipped with a 20 µL loop and rheodyne sample injector, Hypersil RP-C18 column (250 mm x 4.6 mm) Purosphur Star, encapped (5µm particle size) Darmstadt, Germany. Thermo scientific-analytical the column was used. The detector used was SPD (Shimadzu prominence detector) 20-A, Toyoko Japan, dual-wavelength UV-Visible detector, and the eluate was measured at 276 nm, the sensitivity was set at 0.0001 AUFS, the isocratic flow rate was kept at 1 mL/min, the data were recorded using LC software solution version 2.1 (Liquid chromatography).
A 20 µL Hamilton injection syringe was used for sample injection [9]. The flow rate of mobile was increased gradually with maintained constant pressure Kilogram-force (Kgf) and finally flow rate was stabilized constant at 1mL/min, the column temperature was maintained at 25 ± 0.5°C, and the detection of the drug was carried out at 276 nm. HPLC grade Acetonitrile, water and analytical grade potassium dihydrogen phosphate of Merck Limited, Mumbai. India.
Construction of Calibration Curve
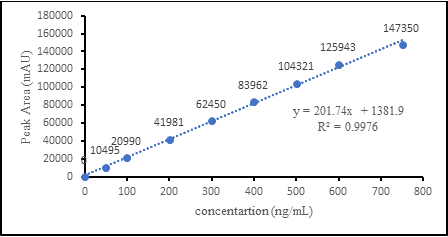
The column was equilibrating with the mobile phase for at least 30 min to the injection of serial concentrations of the drug. The linearity of the peak area response was determined by taking measurement at nine concentrations point including zero concentration, each concentration is measured in triplicate (n=3) Calibration curve was constructed in rabbit plasma, these involves various concentrations of DDEA (0, 50, 100, 200, 300, 400, 500, 600, 750 ng/mL as shown in Table 1) and a fixed concentration of carbamazepine (internal standard) were prepared by taking suitable samples of the working standard solution in different 2 mL Eppendorf tubes and dilution was made up to the mark with the mobile phase. 15 µL of the dilution sample was taken and injected into the column at a flow rate of 1 mL/min, each dilution was injected three times into the column. The drug eluates are monitored at 276 nm and the corresponding chromatograms were obtained. From these chromatograms mean peak area was calculated and a plot of concentration over the peak area was constructed. A linear relationship in the range was found to be 50-750 ng/mL the correlation coefficient R2= 0.9976 and y= 201.74x+1381.9 as shown in Figure 2, from the above equation concentration of drug was estimated and tabulated. The slope of the plot was determined by the method of least square regression analysis and was used to calculate the DDEA concentration in the unknown samples.
| S. No | Concentration of DDEA (ng/mL) | Mean peak area (n=3) | |
|---|---|---|---|
| 1 | 0 | 0 | |
| 2 | 50 | 10495.3 | |
| 3 | 100 | 20990.6 | |
| 4 | 200 | 41981.2 | |
| 5 | 300 | 62450.4 | |
| 6 | 400 | 83962.3 | |
| 7 | 500 | 104321.9 | |
| 8 | 600 | 125943.2 | |
| 9 | 750 | 147350 |
Table 1: Calibration Curve of Diclofenac Diethylamine at 276nm Wavelength.
Preliminary Study
Two days before the study a 2×2cm area on the abdominal of each rabbit was trimmed using a scissors, one day before the study, a depilatory cream was applied for 15 min to the trimmed on the back and to both ears and then thoroughly washed off, to ensure complete removal of the hair in the respective areas [9, 10].
Skin Irritation Test
Skin irritation test was evaluated by the Draize method. Six healthy rabbits were used in this test. The rabbits were trimmed at abdominal skin both left and right side of the rabbit. An aqueous solution of sodium lauryl sulfate (SLS) of 10 %w/v was used as a standard irritant for the skin of the rabbit and its area was calculated according to the following formula. Area₌ ᴨr2. The desired amount of drug containing desired area of transdermal patch was applied on the right- side skin of the rabbit, standard irritant (10 % w/v SLS) was applied at the left side skin of the rabbit, then the patch was removed after a period of 24 hr, 48 hr, 72 hr [11]. Scores were graded after removal of patch from the skin and observed for the development of erythema or any sign of edema for each rabbit compared with standard irritant [12].
Sample Collection
Albino male rabbits of bearing weight 1.75 to 1.85 kg were used in the study. During in vivo pharmaceutical analysis rabbits were given for free access to food and normal water, until night, prior to dosing fasted for 10hrs, before the experiment weight of the rabbit was measured [13]. Any experiment involving the animal use of animals was conducted according to the principle of laboratory animal care and were approved by the institutional animal ethical committee. Vaagdevi institute of pharmaceutical science, Bollikunta. Warangal, India. Reg., No. 1663/PO/Re/S/2012/ CPCSEA.
The experiments were designed as a crossover trial [14]. This meant that the same rabbit was used twice in the experiments including marketed gel (Reference) and optimized transdermal patch (Test). Initially, rabbits were divided into the two groups, each group contains three rabbits. Group 1 (n=3) were subjected to the application of a Marketed gel of diclofenac diethylamine as the reference drug, at dorsal side of the body for the both the groups. Group 2 (n=3) was subjected to application of an optimized formulated transdermal patch for both the groups. Before the application of dosage form rabbits were trimmed using scissor and cleaned with normal saline. The skin of the rabbit was examined in case of any damage. Each rabbit in the group was received marketed gel and a transdermal patch containing DDEA 58 mg with washout period of 15 days. The sample collected points were 1, 2, 3, 4, 6, 8, 10, 12, 24, hrs. About 0.5mL of blood was collected from the marginal ear vein and placed in the K3EDTA tubes. Plasma samples were separated by centrifugation at 3000rpm for 10min at room temperature and stored at -20°C until analysis [15].
Preparation of Sample for Injection into HPLC
Blank plasma sample (rabbit which is not treated) preparation method was validated from taking 10 µL of internal standard (1000 ng/mL of carbamazepine) and 100 µL of acetonitrile was added into 10µL plasma sample in the centrifuge tube. the mixture was vortexed for 2mins and extracted with 0.5mL of supernatant was taken after centrifugation of the Eppendorf tube at 10,000rpm for 10min [16]. into another empty tube and 15µL of the sample were injected into the HPLC for the analysis as a blank.
10 µL of plasma was taken from the previously stored plasma sample (rabbit which is treated) which is subjected to drug analysis of that 10µL internal standard carbamazepine (1000 ng/mL) was added followed by the addition of 100µL of ACN. The entire mixture was mixed with Cyclomixer (Remi, cm101) and separation was done by centrifugation for 10min at 1000rpm [17], about 15 µL of supernatant was collected and injected into HPLC [18, 19] Table 2.
| Time (hrs) | Plasma concentration (ng/mL) | |
|---|---|---|
| Marketed gel | Transdermal Patch (TDDS) | |
| 0 | 0 | 0 |
| 1 | 89.63 | 77.082 |
| 2 | 220 | 138.22 |
| 3 | 340.08 | 194.245 |
| 4 | 241.94 | 259.574 |
| 6 | 177.32 | 112.887 |
| 8 | 107.29 | 168.052 |
| 10 | 55.22 | 139.286 |
| 12 | 6.1 | 98.311 |
| 24 | -nd- | 2.519 |
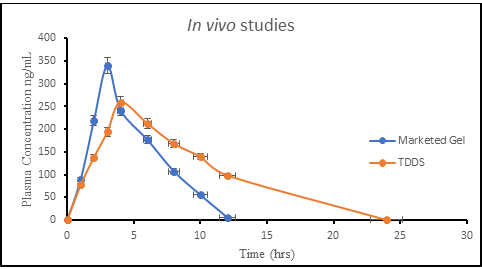
Table 2: Comparative in _vivo_ Plasma drug concentration.
| Concentration (ng/mL) | Intra day | Mean | S.D. | % RSD | ||
|---|---|---|---|---|---|---|
| 250 | 52296.5 | 52450.3 | 56421.32 | 53722.70667 | 2338.332537 | 4.35 |
| 350 | 73212 | 74545.23 | 69587.33 | 72448.18667 | 2565.687278 | 3.54 |
| 550 | 115052.33 | 121458.3 | 100032.65 | 112181.0933 | 10997.61881 | 9.8 |
| Concentration (ng/mL) | Interday | Mean | S.D. | % RSD | ||
| 250 | 54569.66 | 56206.75 | 51097.05 | 53957.82 | 2609.218209 | 4.83 |
| 350 | 75487.99 | 77752.63 | 70684.21 | 74641.61 | 3609.419573 | 4.83 |
| 550 | 121548.32 | 125194.77 | 113813.43 | 120185.5067 | 5811.76997 | 4.83 |
Table 3: Intra-day and Inter-day precision for quantification of DDEA.
| Limit of Detection (LOD) | 38.25 ng/mL |
| Limit of Quantification (LOQ) | 115.91 ng/mL |
Table 4: LOD and LOQ data for detection of DDEA.
Pharmacokinetic Analysis
Phoenix WinNonlin Version 8.1 (Certara USA, Inc.,
Princeton, NJ). Pharmacokinetic parameters of Diclofenac diethylamine was performed with comparison with Marketed gel to transdermal patch, plasma samples were estimated in each rabbit using a computer program, WinNonlin software. Non compartmental analysis with three terminal points were selected for calculation of pharmacokinetic parameters Cmax (ng/mL), Tmax (hrs), AUC (ng-hr/mL), AUMC (hr.hr ng/mL) [20, 21] etc.
| Parameters | Units | R1 | R2 | R3 | R4 | R5 | R6 | Avg | S.D. |
|---|---|---|---|---|---|---|---|---|---|
| Id | 1 | 2 | 3 | 4 | 5 | 6 | |||
| No of Samples | 9 | 9 | 9 | 9 | 9 | 9 | 9 | 0 | |
| Dose (50) | mg | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 0 |
| K E | 1/hr | 0.76996 | 0.731 | 0.5552 | 0.52151 | 0.66844 | 0.70498 | 0.65852 | 0.09938 |
| T 1/2 | hr | 0.90024 | 0.94821 | 1.24846 | 1.32912 | 1.03696 | 0.98322 | 1.07437 | 0.17387 |
| T lag | hr | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| T max | hr | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 0 |
| C max | ng/mL | 340.07 | 341.618 | 339.632 | 328.027 | 350.009 | 341.101 | 340.076 | 7.03518 |
| AUC (0-12hr) | hr*ng/mL | 1742.16 | 1717.54 | 1704.03 | 1683.4 | 1680.69 | 1662.33 | 1698.36 | 28.8184 |
| AUC (0-α) | hr*ng/mL | 1749.45 | 1725.89 | 1713.4 | 1695.94 | 1691.25 | 1670.98 | 1707.82 | 27.7973 |
| Vd | mL | 37119.2 | 39631.2 | 52560.3 | 56532.4 | 44228.3 | 42444.6 | 45419.3 | 7578.35 |
| Cl | mL/hr | 28580.4 | 28970.6 | 29181.7 | 29482.1 | 29563.9 | 29922.5 | 29283.5 | 475.201 |
| AUMC | hr*hr*ng/mL | 8447.67 | 8271.9 | 8263.46 | 8138.98 | 7943.24 | 7846.86 | 8152.02 | 224.09 |
| MRT | hr | 4.82875 | 4.79283 | 4.82283 | 4.79908 | 4.69666 | 4.69596 | 4.77269 | 0.06071 |
Table 5: Pharmacokinetic Profile of Marketed Gel.
| Parameters | Units | R1 | R2 | R3 | R4 | R5 | R6 | Average | S.D. |
|---|---|---|---|---|---|---|---|---|---|
| Id | 7 | 8 | 9 | 10 | 11 | 12 | |||
| No of Samples | 10 | 10 | 10 | 10 | 10 | 10 | 10 | 0 | |
| Dose (mg) | mg | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 0 |
| K E | 1/hr | 0.30389 | 0.29968 | 0.27989 | 0.29897 | 0.28292 | 0.29597 | 0.29355 | 0.00979 |
| T 1/2 | hr | 2.28089 | 2.31295 | 2.4765 | 2.31847 | 2.44994 | 2.34198 | 2.28089 | 0.08014 |
| T lag | hr | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Table 6: Pharmacokinetic Profile of Marketed Gel.
- Tmax hr
- 4
- 4
- 4
- 4
- 4
- 4
- 4
- 0
- Cmax ng/mL
- 247.15
- 250.655
- 275.34
- 272.629
- 254.342
- 257.331
- 247.15
- 11.7074
- AUC(0-12hr) hr*ng/mL
- 2509.12
- 2740.4
- 2702.79
- 2541.6
- 2390.14
- 2371.83
- 2509.12
- 153.829
- AUC(0-α) hr*ng/mL
- 2516.22
- 2748.98
- 2713.85
- 2549.11
- 2399.82
- 2379.61
- 2516.22
- 154.375
- Vd mL
- 65388.4
- 60693
- 65825.9
- 65608.3
- 73641.3
- 70994.2
- 65388.4
- 4598.85
- Cl mL/hr
- 19871.1
- 18188.6
- 18424
- 19614.7
- 20834.9
- 21011.9
- 19871.1
- 1178.75
- AUMC hr*hr*ng/mL
- 19017.2
- 21435.3
- 20901.7
- 19203.2
- 17969.9
- 17752.8
- 19017.2
- 1505.92
- MRT hr
- 7.55786
- 7.79756
- 7.70186
- 7.53331
- 7.48802
- 7.46039
- 7.55786
- 0.13194
Table 7: Pharmacokinetic Profile of Formulated TDDS.
Results and Discussions
After 72 hrs of treated DDEA patches, animals show no skin irritation such as redness of skin or inflammation at the site of application, the selected formulation applied area was found to be free of any sign of irritation thus it is conducted that the formulation are safe for topical application of patch compared with standard irritant. The main aim of the study is to slow the release of drug into systemic circulation for longer period of time, rather than giving sudden increase in Cmax, since pain required prolonged therapy as they need to release medication continuously. The pharmacokinetic parameters obtained with diclofenac diethylamine transdermal patch were different from those obtained with marketed gel administration, this could be due to rapid absorption of drugs via gel, whereas drug in transdermal patch were slowly but continuously absorbed over prolonged period of time.
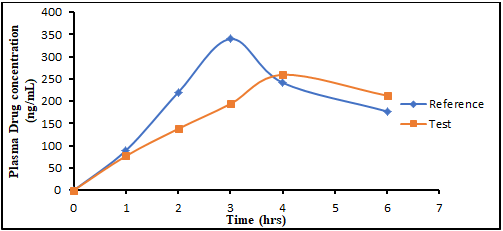
After transdermal application, presence of drug in plasma is quantitative determined by HPLC method and conclusion was scaled between plasma concentration (µg/mL) vs time (hr), The mean plasma concentration versus time profile of DDEA after marketed gel administration and transdermal patches were found as peak plasma concentration, Cmax after marketed gel was found average value of 340.0762 ±7.035 ng/mL and Tmax of 3±0 hr. In the case of transdermal system, the average Cmax and Tmax were 247.149±11.707 ng/mL and 4±0hrs respectively. The various pharmacokinetic parameters were calculated from the plasma concentration of the drug and recorded in Tables 5 & 6. Initially there was rapidly release of drug from transdermal patch which is equal to marketed gel this is due to dermal penetration of the drug containing diethylammonium salt. The same could be established in pharmacokinetic studies on human volunteers even the skin of rabbit and human are different in its penetration. In vivo drug release studies for the formulations patch shows the drug release equivalent to the marketed gel at the initial stages of the study and nearly complete release was achieved in 24 hrs.
In the pharmacokinetic study the rise in drug concentration was slower than marketed gel, the drug concentration in plasma remained steep for longer period with patch due to slow release of drug from the patch to systemic circulation. The release was observed for 24 hrs in transdermal patch. Whereas marketed gel found to complete release of drug up to 12 hrs only, the 12 hrs of release of marketed gel was due to its high protein bonding nature of drug.
The prolongation of the drug upto 24 hrs, in plasma by transdermal system indicates that the drug will remains in the body for longer period and thus it will show a sustained action by inhibiting inflammatory mediator compared with marketed gel. The elimination rate constant (KE) is 0.2935 hrs-1 was found less than marketed gel, and Mean residential time was found to be 7.557 hrs, which is more than marketed gel, Although the Cmax was significantly less with patch, the AUC values were found to be more compared with marketed gel.
Thus, results show that transdermal delivery of DDEA can have worthy potential applications in offering advantages in terms of lowering possible dose administration, reduced dosing frequency, improved patient compliance, reduced high fluctuation, non-invasive characteristic and easy termination of therapy. The patch having DMSO as permeation enhancer and polyethylene glycol used as plasticizer shown maximum amount of drug permeation through rabbit skin membrane. This study clearly shows that in vitro experiments is not purely reflects the in vivo, this clearly indicates that the transdermal patch releases the drug gradually over a prolonged period of time, and terminates upto 24 hrs. The results are represented as mean (± S.D).
Our aim is to overcome the short acting problems associated with DDEA of marketed gel so that our opinion is to fulfill study target, it was preferred to incorporate DDEA in the transdermal system. Since the pharmacokinetic parameter of the formulated transdermal patches were compared to marketed gel, the absence of high fluctuations reduces the side effects such as gastric irritation and bleeding. T1/2 usually showed longer than that marketed gel, this is due to lower elimination of the drug from the plasma and the complete drug release was achieved at 24 hrs whereas marketed gel terminates its action at 12 hrs this means that the transdermal application has much more superior in drug prolongation compare to the rapid release of DDEA in marketed gel.
Low Cmax and prolonged Tmax after transdermal patch administration to the skin leads to an early accumulation of drug in the skin and slower absorption may be the reason which shows clear shift in Tmax followed by its prolonged release into systemic circulation. The reservoir effect after removal of the transdermal patches is due to slow depletion of the drug accumulated in the skin tissue. The higher MRT value of transdermal delivery compared with the marketed gel may be due to the slow and continuous delivery of drug from the transdermal patches. The diclofenac IC50 was approximately 45-50 ng/mL. The topical NSAIDs are highly recommended in the treatment of knee Osteoarthritis. The use of single patch per a day is expected to the more convenient compared with frequent application of gel may leads to over dosing of diclofenac diethylamine.
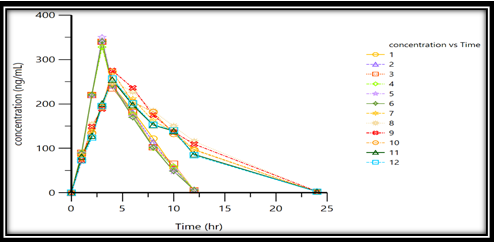
Prolonging release of drug from the patch shows pharmacologically effective range for longer period of time without entering into sub-therapeutic level upto 18 hrs, this conclusion was drawn from the graphical representation of the concentration verses time profile as shown in Table 2 and Figures 3 & 4. The prolonged action of the drug by transdermal patch is suitable for maintaining inflammatory mediator compared with marketed gel. The sensitivity of developed method for DDEA was proved by LOD and LOQ values were found to be 38.25 ng/mL and 115.91 ng/mL as given in Table 4. Percentage RSD was used to determine presence for intraday and Inter day precision for quantification of DDEA was found to be satisfactory in repeated results with very less values of % RSD as show in Table 3.
Finally, the similarity factor was applied between marketed gel and transdermal patches was found to be dissimilarity due to the values obtained as f2= 7.752287 and f1=43.06162 respectively as shown in Figure 5.
Conclusion
In the present study, with respect to the in vivo studies conducted transdermal patch administration of Diclofenac diethylamine produces better improvement compared to topically applied marketed gel. This could be due to slow and continuous supply of Diclofenac diethylamine at a desirable rate into systemic circulation, slower and sustained release of the drug from the transdermal system might reduce the release of inflammatory mediators. The present study shows that topical application of DDEA transdermal patch exhibits better control of pain more effectively for 24 hours, when compared with marketed gel for 12hrs. Inflammation is the prolonged process, for a better therapeutic action 24 hours of treatment is required with less possible dose and side effects [22, 23, 24, 25, 26, 27].
Conflict of Interest
There is no conflict of interest in publishing this article
Acknowledgment
The author would like to thank Dr. Yamsani Madhusudan Rao Director of Vaagdevi group of colleges for this continuous support in building this article and Mr. A. Phaniendra for his help in conducting the experiment. The author gives special thanks to Dr Rajan. M S from Manipal College of Pharmaceutical Sciences for this technical support to analyse the study by WinNonlin software.
References
-
Yamsani SK, Adukondalu D, Bhargavilatha A, Yamsani VV, Gannu R, et al. (2011) Effect of Pomegranate pretreatment on the oral bioavailability of buspirone in male albino rabbits. DARU 19(4): 266-269.
-
Mutalik S, Udupa N (2005) Formulation development, _In vitro_ and _In viv_o evaluation of membrane controlled transdermal system of glibenclamide. J Pharm Pharmaceut Sci 8(1): 26-38.
-
Ikuko Y, Ossuka N, Matsushita I, Miho K, Ichimaro Y, et al. (2016) Plasma Pharmacokinetic and synovial concentrations of S-flurbiprofen 3. plaster in humans. Eur J Clin pharmacol 72(1): 53-59.
-
Sha Sha L, Guo Feng L, Liu L, Jiang X, Bin Z, et al. (2013) Evaluation of paeonol skin target delivery from its microsponges formulation; _In vitro_ skin permeation and _In Vivo_ microdialysis. PLOS One 8(11): 1-8.
-
Chinnala KM, Meka L, Veerareddy PR, Vobalaboina V, Yamsani MR (2008) Development of nitrendipine controlled release formulation based on SLN and NLC for topical delivery: _In vitro_ and _Ex vivo_ characterization. Dru Dev Indu Phar 34(7): 719-725.
-
Mohd A, Asgar A, Yasmin S, Dubey Kiran, Najmi AK, Pillai KK (2006) _In vivo_ Characterization of monolithic matrix type transdermal drug delivery system of pinacidil monohydrate: A technical note. AAPS Pharm Sci Tech 7(1): E1-E5.
-
Chaudhary H, Kohli K, Amin S, Arora S, Vikash K, et al (2012) Development and validation of RP-HPLC method for simultaneous estimation of Diclofenac diethylamine and curcumin in transdermal gels. Journal of Liquid Chromatography & Related Technologies 35(1): 174- 187.
-
Chao L, Liang F (2015) Drug in adhesive patch of zolmitriptan: formulation and _In vitro/In vivo_ correation, AAPS Pharm Sci Tech 16(6): 1245-1253.
-
Naresh K, Naresh T, Balaji K, Sushma G (2012) Design and evaluation of chitosan containing mucoadhesive buccal patch of fluoxetine. International journal of scientific research publications 2(6): 1-5.
-
Naresh K, Srilatha M, Senthil K, Sravan A (2013) Formulation and evaluation of naratriptan orodispersible tablets using superdisintergants by direct compression method. International journal of pharmaceutical research scholar 2(2): 268-278.
-
Setyawan E, Setyowati EP, Rohman A, Nugroho AK (2020) Simultaneous Determination of Epigallocatechin Gallate, Catechin, and Caffeine from Green Tea Leaves (Camellia sinensis L) Extract by RP-HPLC. Research J. Pharm. and Tech 13(3): 1489-1494.
-
Swetha Sri R, Bhavya Sri K, Mounika ChA (2020) Review on Comparative study of HPLC and UPLC. Research J. Pharm. and Tech 13(3): 1570-1574.
-
Sharma DB, Aphale P, Gandhi V, Chitlange SS, Thomas A (2020) Qualitative Analysis of Calendula officinalis Homeopathic Mother Tincture with the help of high Performance Thin Layer Chromatography. Research J Pharm and Tech 13(3): 1113-1116.
-
Khairi MS, Fahelelbom, Altabakha MMM, Eissa NAM, Obaid DEE, et al. (2020) Development and Validation of an RP-HPLC Analytical Method for Determination of Lisinopril in Full and Split Tablets. Research J Pharm and Tech 13(6): 2647-2652.
-
Chakraborty T, Gupta S, Saini V (2020) In vivo Study of Insulin-loaded Microemulsion Topical gel with Aloe vera for the Treatment of Dermatologic Manifestation of Diabetes. Research J Pharm and Tech 13(9): 4115-4124.
-
Chaudhari B, Kartika D (2020) A Validated RP-HPLC Method for Simultaneous Estimation of Tizanidine and Nimesulide in Bulk and Pharmaceutical Formulation. Research J Pharm and Tech 13(9): 4207-4212.
-
Kudupudi C, Manikandan A (2020) A New RP-HPLC Method Development and Validation of Paracetamol and Aceclofenac in Tablets by separating Diclofenac. Research J Pharm and Tech 13(9): 4334-4338.
-
Umamaheswari R, Kothai S (2020) Effectiveness of Copper nanoparticles loaded microsponges on Drug release study, Cytotoxicity and Wound healing activity. Research J Pharm and Tech 13(9): 4357-4360.
-
Maruthi R, Chandan RS, Barath M, Datta GN, Dsilva M, et al. (2020) Analytical Method development and Validation of Teneligliptin by RP-UFLC. Research J Pharm and Tech 13(9): 4035-4040.
-
Satyanarayana L, Naidu SV, Narasimha Rao M, Ayyanna C, Kumar A (2011) The Estimation of Raltigravir in Tablet dosage form by RP-HPLC. Asian J Pharm Ana 1(3): 56-58.
-
Haque A, Shahriar M, Parvin MN, Ashraful Islam SM (2011) Validated RP-HPLC Method for Estimation of Ranitidine Hydrochloride, Domperidone and Naproxen in Solid Dosage Form. Asian J Pharm Ana 1(3): 59-63.
-
Sebaiy MM, Abdullah AES, Sobhy MEA, Lobna MAA, Hisham AH (2011) Rapid RP-HPLC Method for Simultaneous Estimation of Norfloxacin and Tinidazole in Tablet Dosage Form. Asian J Pharm Ana 1(4): 79-84.
-
TandelJinal N, Dilipkumar AP, Payal PC, Samir KS (2018) An Isocratic RP-HPLC Method for Simultaneous Analysis of IlaprazoleAnd Domperidone in Pharmaceutical Formulation. Asian J Pharm Res 8(1): 01-05.
-
Naresh K, Goverdhan P, Balamurugan K (2019) Formulation and characterization of flurbiprofen loaded microsponge based gel for sustained drug delivery. Int J Res Pharm Sci 10(4): 2765-2776.
-
Naresh K, Gurinder BS, Patibandla S, Goverdhan P, Sudha KS, Krishna M (2019) Boini Nicotine instigates Podocytes injury via NLRP3 Inflammasome activation. Aging 11(24): 12810-12821.
-
Naresh K, Goverdhan P, Balamurugan K (2020) Formulation and Evaluation of Diclofenac Diethylamine Loaded Microsponges containing gel as Novel drug delivery system. Int J Pharma Res 12(2).
-
Naresh K, Goverdhan, Balamurugan K (2021) Comparative Pharmacokinetic Studies of Diclofenac Diethylamine marketed and Microsponges Gel in Rabbits. Research J pharm and tech 14(12): 6385-6391.
- Hydrogen Peroxide Scavenging by Methanolic Extracts of Coriander: An In Vitro Antioxidant Study
- Aromatherapy in Palliative Care: A Fragrant Quest for Relief
- Empowering Women, Securing Futures: Contraception’s Role in Socioeconomic Progress in India
- Effect of Crospovidone, Croscaramellose Sodium in Combination on the Drug Release of Anti diabetic Medication in Tablet Form
- Knowledge, Attitudes, Anxiety, and Preventive Behaviors Regarding Covid-19 Affliction among Healthcare Workers in Pakistan
- “Competitive Landscape and Brand Equivalents: Implications for ANDA (Abbreviated New Drug Application) Approval”