Complications after Surgical Treatment of the Peritoneal Vaginal Process in Children
Actuality: Despite the modern developments in surgery, postoperative complications and relapses in children with the pathology of peritoneal vaginal process (processus vaginalis peritonei) continue to occur in the practice of a pediatric surgeon. Purpose: To define causes of complications and relapses after surgical treatment of children with obliteration of the peritoneal vaginal process. Material and methods: The authors present surgical treatment outcomes of 1 818 children with the pathology of peritoneal vaginal process; 32 of these had postoperative complications and relapses. Two clinical observations of children aged 10 and 14 years who underwent surgery for the recurrence of inguinal hernia and hydrocele are described. Results: The rate of relapses or complications following surgical treatment of children with inguinal hernia, hydrocele and cryptorchidism at the Clinical and Research Institute of Emergency Pediatric Surgery and Trauma ranges from 1.5 % to 2.3%. Conclusion: The main reason for complications and relapses in the pathology discussed is the violation of surgical protocol.
Introduction
Despite the achievements of modern medicine and a widespread use of modern diagnostic and curative modalities, namely, laparoscopy and sonography, obliteration of the peritoneal vaginal process still remains relevant in terms of incidence, postoperative complications and relapses.
Pathologies such as inguinal hernia, hydrocele, a cyst of spermatic cord, cryptorchidism are among the most frequent causes for planned surgical treatment in pediatric practice.
The trials conducted at several clinics in the United States have demonstrated that the peritoneal vaginal process is not closed in 80-90% of children at birth; however, this pathology steadily declines by the age of two years, and it occurs only in 20% of children two years old and above [1, 2].
These studies from several clinics in the United States were conducted in 80,000 children aged 0 to 15 years. It has been found out that inguinal hernia occurs in 6.62% of the boys and 1% of the girls [3].
The cryptorchidism prevalence in the United States ranges from 3.7% at birth to 1.1% after one year of life to the adulthood. At the international level, the cryptorchidism prevalence ranges from 4.3 to 4.9% at birth to 1-1.5% at 3 months to 0.8-2.5% at 9 months [4, 5].
According to Russian authors, inguinal hernias occur in 1- 5%of children, while communicating hydrocele occurs in 10% of the newborns. Undescended testicles occur in 10-20% of premature and immature children and in 2-3% of one-year olds [6, 7, 8, 9, 10, 11].
Data in the foreign (United States and Italy) literature shows that the percentage of recurrence and complications after surgical treatment of this pathology ranges from 0 to 8% [12].
The most frequent postoperative complications in patients with the pathology of peritoneal vaginal process are [6, 7, 12, 13, 14]
- Relapse of inguinal hernia / hydrocele
- Secondary cryptorchidism
- Testicular atrophy
Material and Methods
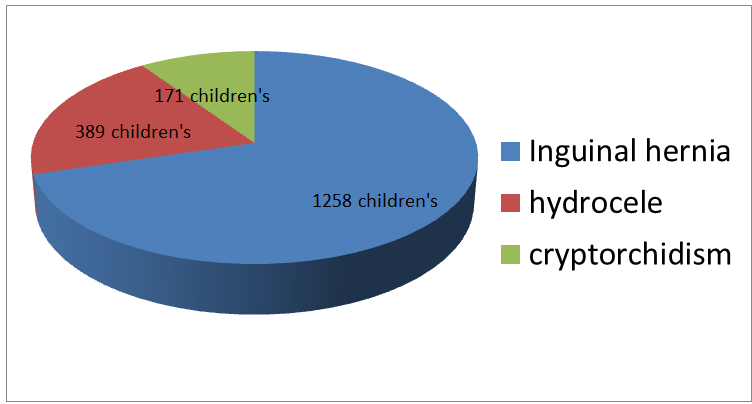
From 2007 till 2017, 1 818 children with the obliteration of peritoneo-vaginal process were treated at the Clinical and Research Institute of Emergency Pediatric Surgery and Trauma (CRIEPST) (Moscow). Among them, inguinal hernias were in 1 258 (69.2%) patients, edema of testicular membranes in 389 (21.4%) and cryptorchidism in 171 (9.4%) (Figure 1). Boys were 1364 child girl 454. Out of all admitted children, 32 had relapses and complications after surgical treatment: 17 children were initially operated in CRIEPST, while others 15 - at other medical centers (Russia, Ukraine). Among all children admitted with complications and relapses, the majority were children who underwent the surgical treatment for:
inguinal hernia - 22 children, hydrocele - 6 children, cryptorchidism - 4 children (Figure 2).
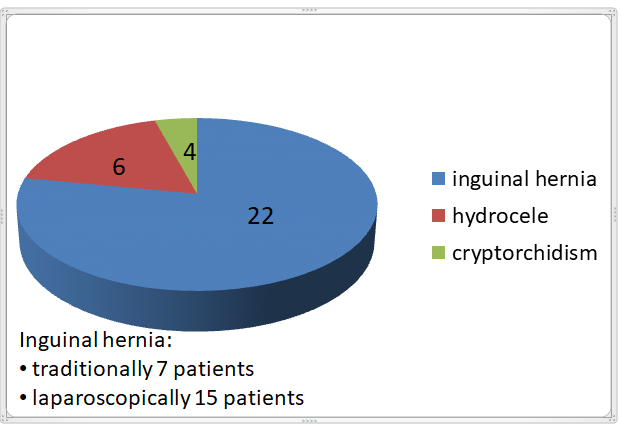
Within the treatment process of inguinal hernias, we used both traditional techniques of hernia repair by Duhamel, and the laparoscopic ones (laparoscopic suturing of the internal inguinal ring with purse-string suture, PIRS -percutaneous internal ring suture). In the communicating edema of testicular membranes, Ross surgery was performed; in cryptorchidism, the repair surgery was performed- orchiopexy by Schumacher-Petrivalsky. The undecended testicle was repaired laparoscopically or by the open surgery depending on its location.
Results
The frequency of relapses or complications after surgical treatment of children with inguinal hernias, hydrocele and cryptorchidism at our hospital ranged from 1.5% to 2.3% (Table 1).
| Complications and relapses after treatment of inguinal hernias | Number of patients |
| The failure of the purse-string suture after laparoscopic hernioraphy | 5 (0,27%) |
| Purulent-inflammatory complications | 2 (0,11%) [13-15] |
Table 1: Complications and relapses after treatment of inguinal hernias. Below are two clinical cases of the children operated on
Clinical Observations
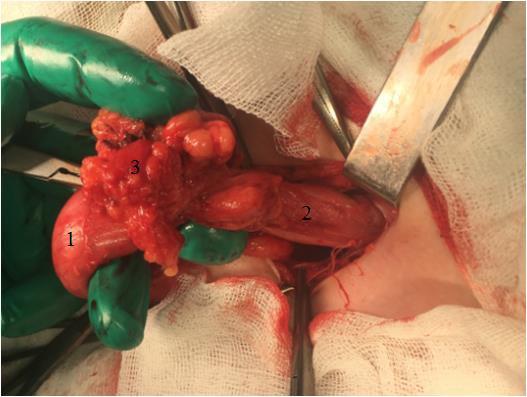
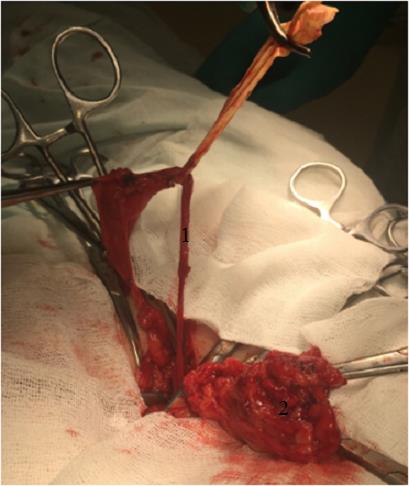
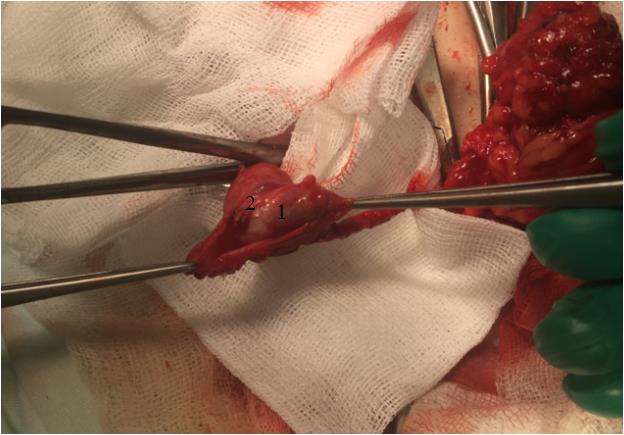
Patient V., 10 years old, was hospitalized to the surgical department in CRIEPST for a planned surgery on September 20, 2015, with the following diagnosis: non- palpable left testicle syndrome, secondary postoperative dystopia of the left testicle. Postoperative left-sided inguinal hernia. A child had hydrocele of the left testicle since his birth At the age of 5, he underwent surgery at one of surgical centers in Moscow. The left-sided Ross surgery was performed. In 2015, during the routine follow-up examination a surgeon did not detect the left testicle in the scrotum. The same year (2015), the child was hospitalized to our clinic for surgical treatment. The patient was examined by a surgeon; sonography was made too. The performed sonography revealed: right testicle of 23x13 mm was visualized in the scrotum, left testicle was smaller 14x8 mm and was visualized along the inguinal canal; hernial protrusion 25x10 mm was seen at the same place. Physical examination: The external genitalia are male- shaped, the left half of the scrotum is hypoplastic; in the left inguinal region there is a transverse normotrophic pale scar that does not protrude above the skin and has a form of 3 cm long strip. The right testicle in the scrotum is about 2.0 x 1.5cm. The left testicle is not detected in the scrotum; it is palpable in the inguinal region, size 1.0 x 0.8 cm, not descended into the scrotum. To the left, the external inguinal ring of 1.5x1 cm is expended without hernial protrusion; when straining, hernial protrusion is not reliably palpable (an over-nutritional child with pronounced subcutaneous fatty tissue). On October 1, 2015, the planned surgery was made. The testicle was descended; Schumacher-Petrivalsky orchopexy. Intraoperatively: With the groin access on the left, an old scar was incised in layers with technical difficulties caused by a pronounced scar-adhesive process; in the area of external inguinal ring the left testicle in membranes and in a conglomerate of scar and cellular tissues was exposed. The testicle was found to be fused to the aponeurosis of the external oblique abdominal muscle in the area of external inguinal ring. During mobilisation, a hernial sac with contents of yellow colour, when examined against the light, was found; the bottom of this sac was fused to testicular membranes with scarred fiber bands. The entire conglomerate was separated and mobilized from the external inguinal ring. The front wall of inguinal canal was cut, the hernial sac was separated from sperma cord elements and testicular membranes and opened. A strand of the greater omentum about 10x15 cm in size partially fused to the wall of hernia sac without visually obvious ischemia was found inside (Figures 3 & 4). Resection of the greater omentum within free tissues was made; the stump was easily placed back into the abdominal cavity. The hernial sac was sutured at the cervix, tied and clipped and sent for histological examination together with a resected fragment of the greater omentum. Testiclular membranes were separated from scar tissues, opened. The testicle was in cicatricial coarse adhesions which were fused with the albugine membrane almost over the entire area. This testicle was separated from adhesions as much as possible. Visually, the testicle (about 17x8 mm in size) was deformed (round, with impressions from scars of different shapes and areas, difficult to differentiate from the epididymis), flabby (Figure 5). The blunt tunneling was performed distally to the scrotum. The testicle was sewed through membranes, descended without tension and fixed to the bottom of the scrotum. The ligature was punctured from the cavity of the scrotum on the skin and fixed on a cotton roller. The wound was sutured in layers. Stitches were removed on the 7th day after the surgery, the wound healed by primary intention. The patient was discharged home in a satisfactory state.
The control sonographic examination of scrotum organs before the patient’s discharge showed that the right testicle was 20x15 mm with homogeneous echostructure and satisfactory blood flow. The size of the right epididymis - 7x7 mm. The left testicle was 14x13mm with unhomogeneous echostructure and weakened blood flow. The epididymis was not visualized.
Catamnesis 2 years 6 months after discharge. At the examination, external genitalia are male-shaped, normal. Testicles in the scrotum. Visual examination and palpation revealed hypotrophy of the left testicle. Sonography of the scrotum: right testicle is 46x19 mm with homogeneous echostructure and satisfactory blood flow. Right epididymis - 9x9 mm. The size of the left testicle - 21x14mm with unhomogeneous echostructure and satisfactory blood flow. Epididymis of the left testicle is 4x4 mm (Figure 6). Signs of left-sided orchopathy compared to the contralateral side are still seen; however, size of the left testicle has increased after the surgery.
In the presented clinical observation, postoperative complications after primary surgical interventions, in our opinion, were most likely related to not quite careful separation of the peritoneal vaginal process or due to the retraction of the testicle by scar tissue.
Second Observation
Patient G, 14 years old. The patient was admitted to the Clinical and Research Institute of Emergency Pediatric Surgery and Trauma (CRIEPST at the first surgical department on October 6, 2015, with the relapse of strangulated inguinal hernia on the left. State after repeated laparoscopic herniorraphies on the left in 2006 and 2009. Incision and drainage of a ligature fistula on the left in 2013. Isolated hydrocele of left testicle membranes. According to his mother, in 2006 the left-sided inguinal hernia was diagnosed by a surgeon at the dispensary examination at their pediatric outpatient unit. The same year, the child was operated on in one of Moscow hospitals - laparoscopic hernia repair was made. In 2009, patient’s mother again noticed hernial protrusion in the left inguinal region. The performed sonography revealed recurrent inguinal hernia on the left. In 2009, the child was hospitalized for re-operative treatment in the same hospital, left laparoscopic herniorraphy was made. In 2013, swelling and hyperemia of the postoperative scar in the groin on the left were seen. The patients were examined at the same center where he was operated on. A ligature fistula was diagnosed. The abscess was opened and fistulous tract was incised; the ligature was removed. At the follow-up examination in 2015, edema of the left testicle was found.
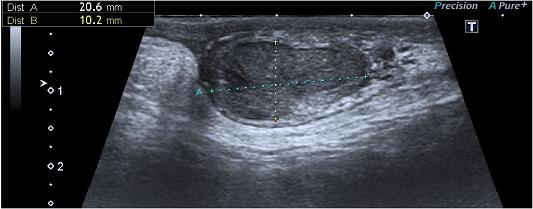
In 2015, the child was admitted to CRIEPST at the first surgical department for a planned surgery. In the department, the child was examined by a surgeon. Sonography was made. At the sonographic examination of the left inguinal canal, hernial protrusion sized about 24x10 mm was seen in the upper third; blood flow was not disturbed. Right inguinal canal without features. A moderate amount of homogeneous effusion in membranes of the left testicle. Size of testicles: right - 29x17 mm, left - 24x17 mm (Figure 7).
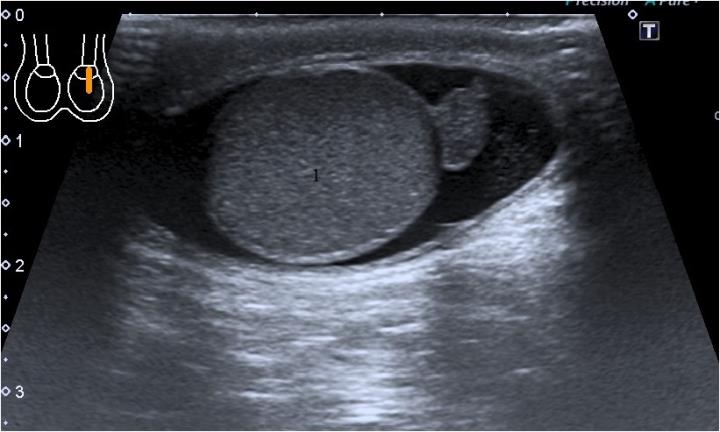
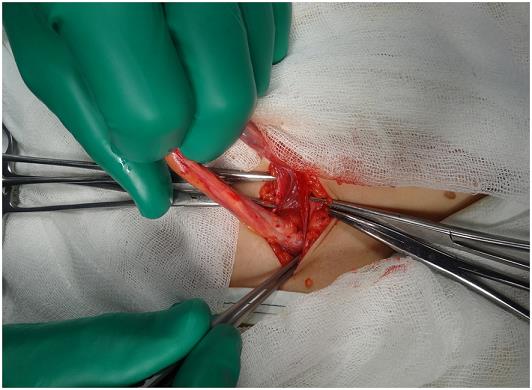
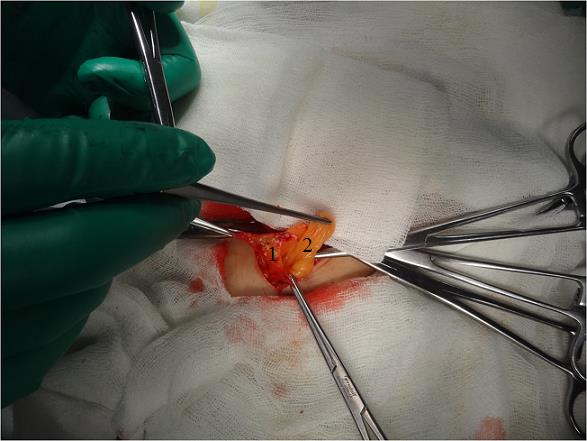
Figure 7: Sonographic picture before surgery. 1- left testicle, 2- serous fluid in the scrotum cavity. Physical examination: External genitalia are male- shaped, normal; testicles in the scrotum, of equal size (about 2.5 x 1.2 cm). There is an expansion (up to 1.5 cm) of the left external inguinal ring with hernial protrusion of 2.0 x 2.0 cm, soft-elastic consistency which is freely and painlessly set into the abdominal cavity. A symptom of cough push is positive. On the left, a moderate fluid accumulation in membranes of the left testicle is palpable (volume decreases with compression). There is no hernial protrusion on the right; the external ring of the inguinal canal is not extended. Postoperative scars on the anterior abdominal wall are normotrophic, pale, there is no inflammation. Intraoperatively: The front wall of inguinal canal was exposed and opened by skin incision in layers in the left inguinal region at the projection of inguinal canal. As soon as the spermatic cord did separated, surgeons immediately paid attention to the fatty tissue in the spermatic cord resemble the large omentum. During mobilization of the spermatic cord, a rough cicatricial- adhesive process was revealed in the internal inguinal ring. When the adipose tissue was separated, a strand of large omentum about 10x15 cm in size was found; it was fused to the peritoneum by circular cicatricial bands in the projection of internal inguinal ring (Figures 8 & 9). Elements of the spermatic cord (spermatic cord and testicular vessels) were separated. Resection of the greater omentum was made within the margins of free tissues (a resected part was sent for histological examination), the remaining part was placed back into the abdominal cavity. A purse string was put on the peritoneum of internal inguinal ring. A “window” was made in testicular membranes, and clear liquid of about 3.0 ml was obtained; the testicle was put into the scrotum. Hemostasis during surgery. Plasty of the inguinal canal by Martynov, sutures in layers, iodine, aseptic adhesive bandage.
Stitches were removed on the 7th day after the surgery; the wound healed by primary intention. Sonographic control examination of the scrotum performed on the 7th day after the surgery revealed no complications. The child was discharged home in a satisfactory state.
Catamnesis of the patient from the second observation in 2 years 6 months after the surgical treatment: clinically, external genitalia are of male- type form, regular, testicles in the scrotum. Postoperative scars normotrophic, no inflammation. Sonographic examination of the scrotum revealed no pathology.
The relapse of the disease in this patient, to our mind, was caused by purulent-inflammatory complications.
Discussion and Conclusion
Obliteration of the peritoneal vaginal process is one of the most frequent reasons for hospitalizing pediatric patients to have a planned surgery. Despite of the developments in modern surgery and in laparoscopic techniques for treating the discussed pathology, postoperative complications and relapses are still occur in surgical practice.
In the presented clinical observations, postoperative complications and relapses after primary surgical interventions, in our opinion, were most likely due to the fact that the testicle in the scrotum was not fixed, the vaginal process of the peritoneum was not carefully isolated to its base, the outer ring of the inguinal canal was not narrowed when it expanded. The testicle could have caught up with the scars. In the second clinical observation, the relapse was associated with purulent - inflammatory complications.
The analysis performed has shown that the main requirement for the prevention of relapses and complications is to strictly follow the existing surgical protocols both for traditional surgical interventions and for laparoscopic ones.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgments
The study had no sponsorship
References
-
Ortenberg J, RothCC (2016) Pediatric hydrocele and hernia surgery.
-
C Parke J (2017) Hydrocele.
-
Hebra A (2016) Pediatric hernias.
-
Sumfest JM (2017) Cryptorchidism.
-
Perez-Brayfield M (20017) Pediatric cryptorchidism surgery.
-
Isakov Yu F, Dronov AF (2009) Pathology of the vaginal process of the peritoneum. In: Pediatric surgery: National Guidelines"[Detskaya hirurgia: nacionalnoe rukovodstvo]. Moscow, GEOTAR, Media.
-
Podoluzhny VI, Krasnov OA, Kotov MS, Starchyonkov SB (2015) Inguinal and femoral hernias [Pahovaya i bedrennaya griji]. Monography, Kemerovo pp: 148.
-
Mirsky V Ye, Rishchuk SV (2012) Occurence structure, level of andrological morbidity among children and adolescents, and ongoing therapy. In: Diseases of the reproductive system in children and adolescents (andrological aspects): a Guide for physicians [Zabolevaniya reproduktivnoy sistemi u detey i podrostkov (andrologicheskie aspekti): rukovodstvo dlya vrachey. St. Petersburg: SpecLit.
-
Kadyrov ZA, Murodov AI (2017) Hernia of the anterior abdominal wall and andrological diseases. Interrelation, some epidemiological issues, etiology and simultaneous surgeries (a literature review). Andrologiya i genitalnaya hirurgiya 18(2): 10-14.
-
Tikhomirova VD (2011) Pediatric Surgery: A practical guide [Detskaya operativnaya hirurgia: practicheskoe rukovodstvo]. St. Petersburg: Information and publishing agency "LIC".
-
Yatsik SP (2013) Diseases of the reproductive organs in boys and young men [Bolezni organov reproduktivnoy sferi u malchikov i yunoshey]. Moscow, Pediatr.
-
Esposito C, St Peter SD, Escolino M, Juang D, Settimi A (2014) Laparoscopic and open hernial plasty in children: a systematic review. J Laparoendosc Adv Surg Tech A 24(11): 811-818.
-
Lapshin VI, Razin MP, Smirnov AV, Baturov MA (2017) Congenital inguinal hernia in a child. Detskaya hirurgia 21(1): 52-53.
-
Dvorakevich AO, Pereyaslov AA (2016) Mini-invasive treatment of recurrent inguinal hernias in children. Detskaya hirurgia 20(3): 140-143.
-
Dronov AF, Kozlov Yu A, Mokrushina OG, Morozov DA, Novozhilov VA, et al. (2013) Strangulated inguinal hernias in children. Rossiyskiy vestnik detskoy hirurgii, anesteziologii I reanimatologii 3(3): 87-97.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?