Guillian- Barre Syndrome and Sensorineural Deafness – A Case Report
Guillian- Barre syndrome is a rare disorder in which your body immune system attacks your nerves. Guillian- Barre syndrome is a demyelinating disease where the myelin sheaths of neurons are damaged. This article includes a case of Guillian - Barre syndrome in an 8 years old girl from Dandeli, a Town in the north Karnataka region of India. A detailed speech language and hearing profile based on systematic evaluation has been highlighted in the present study.
Introduction
Guillian–Barre syndrome (GBS) is a rare disorder in which your body’s immune system attacks your nerves .weakness and tingling in your extremities are usually the first symptoms [1]. Patients usually presents with rapidly evolving ascending weakness, mild sensory loss Hyporeflexia or areflexia [2]. Most patients complain of paresthesias, numbness, or similar sensory changes. Sensory symptoms often precede the weakness [3]. The MRI findings include spinal nerve root enhancement with gadolinium is a non-specific feature seen in inflammatory conditions and is caused by disruption of the blood nerve barrier. Selective anterior nerve root enhancement appears to be strongly suggestive of GBS [4] .
Hearing Impairment is the most frequent sensory deficit in human populations, affecting more than 250 million people in the world. Consequences of hearing impairment include inability to interpret speech sounds, often producing a reduced ability to communicate [5].
Few studies show an association with GBS and Sensorineural deafness. A Study showed a connection of hearing impairment and GBS. They elicited auditory brainstem responses from two individuals with GBS where one patient was acutely deaf with total absence of BAEP waveforms indicative of acoustic nerve conduction block and second patient had bilaterally prolonged wave I latencies. These ABR findings suggest that acoustic nerve conduction abnormalities from demyelination may occur in GBS [6].
Another study showed that Brainstem auditory evoked potentials were abnormal in five of six patients with Guillain-Barré syndrome. The abnormalities imply focal demyelination in the extramedullary portion of the auditory nerve [7].
Previous studies do not discuss in detail the speech language and hearing characteristics of children with GBS which has been included in the present study and also there are no studies or case reports from India reporting Hearing impairment associated with GBS. The present study defines the speech, language, communication and hearing aspects of GBS in detail which gives insight to the communication deficit associated with GBS.
Case Presentation
The patient aged 8 years old female, a resident of Dandeli, a village in north Karnataka region of India approached JSS Institute Of Speech And Hearing, Dharwad with the complaint of unclear speech and reduced hearing sensitivity.
Medical History
The Child was diagnosed as having acute onset motor predominant quadreparesis secondary to Guillian–Barre syndrome. History of moderate grade fever not associated with chills and rigors since 6 months. The child also reported pain in lower limbs, acute in onset, progressive and intermittent. History of weakness of bilateral upper and lower limbs since six months, acute in on set, initially started in lower limb and later progressed to upper limbs over 4 days. The parents report betterment in the condition after treatment.
Acetyl choline receptor binding antibody serum test was conducted to differentially diagnose between Myasthenia Gravis and GBS. The results indicated negative findings for Myasthenia gravis. Whole spine screening and Brain screening tests were conducted and there were no significant findings in the above tests. Nerve conduction study was conducted to confirm GBS. The results showed reduced conduction velocities, conduction blocks at non-entrapment sites, temporal dispersion and prolonged F wave latencies, hence confirming the diagnosis of GBS.
Speech and Language Evaluation
Detailed case history included a structured interview with the parents, clinical interaction with the patient and physical examination. Parents complained of unclear speech reduced hearing sensitivity. Parents were first cousins indicating second degree consanguinity. Pedigree analysis was carried out where it was found to be an autosomal recessive disorder (Figure 1).
The child was born after full term of pregnancy. Parents reported history of high fever at the age of 8 years and the child was admitted to hospital for 10 days. Developmental history revealed normal motor and Speech and language milestones development [8]. Adequate self-help skills and no unusual behaviors were observed. Gait disturbances were noticed.
Language and Communication
Detailed Speech and Language assessment was carried out by administering several standardized tests such as REELS (Receptive Expressive Emergent Language Scale) and Kannada articulation Test (KAT). Results of REELS showed age adequate receptive and expressive language skills. KAT results revealed substitution errors and cluster reduction was seen.
Hearing Evaluation
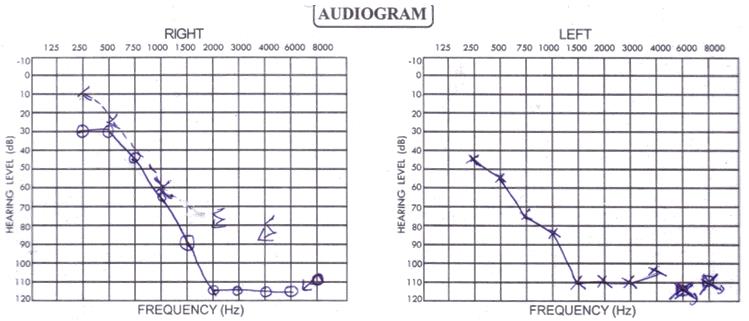
Pure tone audiometry was done and a sloping type of audiogram was obtained (Figure 2). Both Air conduction and bone conduction thresholds were affected indicating a sensori-neural type of hearing loss. The pure tone average obtained was 81.25 dB and 88.75dB for right ear and left ear respectively indicating a severe degree of hearing loss.
Tympanometry and Reflexometry were conducted to assess the functioning of middle ear. Bilateral ‘A’ type tympanogram indicated normal middle ear functioning. Absence of iplsilateral and contralateral reflex thresholds signify abnormal reflex pathway. Distortion Product Oto Acoustic Emission (DPOAE’s) test was done to evaluate outer hair cell functioning. Bilateral absence of DPOAE’s indicated outer hair cell dysfunction.
Diagnosis and Treatment
Based on the history collected from the patient’s family, physical examination, findings of other disciplines and results of the both objective and subjective tests, she was diagnosed as having Speech sound disorder secondary to bilateral severe sensori-neural hearing impairment.
Parents were counseled regarding fitting of a high gain hearing aid along with continuous speech therapy which will help her in her overall communication and development.
Discussion
Sensorineural Hearing Loss has been reported rarely in GBS patients [9, 10, 11, 12, 13, 14]. Researchers studied evoked potentials (EPs) in 27 patients with typical acute Guillain- Barré syndrome and 3 with Fisher's syndrome. Three of 21 had BAEP abnormalities: 1 with bilateral I-III, 1 with unilateral I-III, and another with unilateral III-V interwave latency prolongations [15].
Another study showed Left side-dominant bilateral hypoacusia with audiogram, and left side-dominant bilateral prolongation of I wave latency with auditory brainstem response (ABR). The ABR findings indicated that the auditory nerve was impaired on the peripheral side, which may have been associated with GBS [16].
Conclusion
In conclusion, we have herein highlighted the speech and hearing complications in a child with Guillian- Barre’ Syndrome. The present study shows absence of ABR waves which may suggest a connection between GBS and Hearing impairment. Abnormal ABR was reported previously in GBS patients [7, 15]. One of these studies mentioned the presence of facial nerve palsy in three of five GBS patients with abnormal ABR [7]. Thus, physicians should pay more consideration to auditory dysfunction in GBS patients with facial nerve palsy and also speech and hearing evaluation should be made a mandatory test in the test battery of GBS.
The authors state that they have no Conflict of Interest (COI).
References
-
Asbury AK, Cornblath DR (1990) Assessment of current diagnostic criteria for Guillain-Barré syndrome. Ann Neurol 27(Suppl): S21-S24.
-
Dimachkie MM, Barohn RJ (2015) Peripheral Neuropathies. Nerves and Nerve Injuries pp: 857- 888.
-
Andrea CA (2008) Sensory Loss and Paresthesias. Mayo Clinic Essential Neurology pp: 135-158.
-
Yardimci N, Avci AY, Kayhan E, Benli S (2009) Bilateral facial nerve enhancement demonstrated by magnetic resonance imaging in Guillain-Barré syndrome. Neurol Sci 30(5): 431-433.
-
Smith AW (2001) WHO activities for prevention of deafness and hearing impairment in children. Scandinavian Audiology 30(2): 93-100.
-
Kevin RN, Robin LG, Andrew M (1988) Acoustic nerve conduction abnormalities in Guillain-Barre syndrome. Neurology 38(8): 1263-1263.
-
Schiff JA, Cracco RQ, Cracco JB (1985) Brainstem auditory evoked potentials in Guillain-Barré syndrome. Neurology 35(5): 771-773.
-
Wijnhoven TM, De Onis M, Onyango AW, Wang T, Bjoerneboe GA, et al. (2004) Assessment of Gross Motor Development in the who Multicentre Growth Reference Study. Food and Nutrition Bulletin 25(1_suppl_1): S37-S45.
-
Sugiyama K, Inafuku S, Takimoto I, Kihara M, Takahashi A (1985) A case of polyradiculitis with hearing loss: analysis of auditory brain stem response. Auris Nasus Larynx 12(2): 59-66.
-
Pall HS, Williams AC (1987) Subacute polyradiculopathy with optic and auditory nerve involvement. Arch Neurol 44(8): 885-887.
-
Nagai T, Shinohara Y, Kametsu Y, Yamamoto M (1991) A case of postinfectious polyradiculoneuropathy initially manifested as sudden and severe bilateral hearing loss. Rinsho Shinkeigaku 31(4): 422-426.
-
Herinckx C, Deggouj N, Gersdorff M, Evrard P, Guérit JM (1995) Guillain-Barré syndrome and hypacusia. Acta Otorhinolaryngol Belg 49(1): 63-67.
-
Tamura M, Tajiri N, Sakamaki S, Tada Y, Takasu T (1997) Acute polyradiculoneuritis with severe hearing loss. A case report. Neurol Med 46: 181-184.
-
Yano S, Goto H, Fujishita S, Matsuo H, Shibuya N (1999) Bilateral severe perceptive deafness in Guillain-Barré syndrome, after IVIG treatment. A case report. Neurol Med 51: 457-460.
-
Ropper AH, Chiappa KH (1986) Evoked potentials in Guillain-Barré syndrome. Neurology 36(4): 587-590.
-
Ueda N, Kuroiwa Y (2008) Sensorineural deafness in Guillain-Barré syndrome. Brain Nerve 60(10): 1181- 1186.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?