Renal Involvement in Acute Gastroenteritis under 5 years of Age in a Tertiary Care Hospital of Western Nepal–A prospective Observational Study
Background: Acute renal failure is one of the important complications of acute gastroenteritis in children. Early intervention and proper fluid replacement may lessen this risk. Acute gastroenteritis (AGE) is an infection of the gastrointestinal tract that commonly affects young children. It causes an increase in loss of water and electrolytes due to vomiting and diarrhea resulting to dehydration, which is the main cause of mortality in children under five years with acute gastroenteritis. Therefore, this study was designed to find out the incidence of AGE and the status of associated electrolyte derangements, renal involvement and other biochemical and haematological variables. Material and Methods: This cross sectional study comprised of 100 cases of AGE in children aged <5 years of age. Demographic profile of the patients, details of diarrhea, and accompanying degree of dehydration (defined as per World health Organization criteria) with any associated complication were included. Various electrolyte parameters along with biochemical and hematological parameters (serum urea, serum creatinine, hemoglobin, total leukocyte count) were investigated Results: This study found that urea and creatinine were elevated in 29(29%) and 62(62%) of the cases respectively. Electrolyte disturbances were seen in 42% of cases among which hyponatremia was the most common electrolyte disturbance seen.Majority of patients had isonatremic dehydration 58%. Hyponatremic dehydration was most common in some dehydration, which was 30%. We found hypokalemia in 31% cases. Conclusion: Measurements of renal parameters early can help to predict the complications due to AGE and may help in the prevention of diarrhea related complications in children.
Introduction
Acute gastroenteritis is generally defined as a decrease in the consistency of stools (loose or liquid) and/or an increase in the frequency of evacuations (typically ≥3 in 24 hours), with or without fever or vomiting; however, a change in stool consistency versus previous stool consistency is more indicative of diarrhea than stool number, particularly in the first months of life. Acute diarrhea typically lasts <7 days and not >14 days [1]. The term Gastroenteritis denotes infections of the gastrointestinal (GI) tract caused by bacterial, viral, or parasitic pathogens [2]. Worldwide, Gastrointestinal diseases are considered as common illnesses, the second most common cause for visits to physicians, and of morbidity and mortality among infants and children under five throughout the developing world. It has been estimated that in Latin America, Africa, and Asia depending on nutritional and socio – economic factors, a child’s chance of dying by diarrheal illness before the age of five years can be as high as 50%. In developing countries, a quarter of infants and childhood mortality is related to diarrhea. In Iraq, according to the annual report of the Iraqi Ministry of Health (M.O.H), the average of diarrheal patients visiting the medical and health care facilities related to M.O.H for the years 2009 and 2010 is 201 and 212 / 1000 child under five years of age. Also, it is estimated that the percentage of diarrhea cases to the total pathological cases requiring hospitalization in children less than five years of age is 19.1 % for the year 2009, and 24.9 % for the year 2010 [3]. Diarrheal disease occupied the second place among the top ten diseases in Nepal [4]. Poverty, illiteracy, lack of health care facilities at local level, demographical distribution and traditional beliefs are the major obstacles for getting proper and timely healthcare [5].
The main route of transmission of enteropathogens is faecal-oral through the ingestion of contaminated food or fluids or by direct person-to-person contact. The factors that increase the transmission of enteropathogens in developing countries include contaminated water and food, poor sanitation and hygiene, lack of breastfeeding, malnutrition, deficiencies in micronutrients like zinc or vitamin A, crowded environment, and living close to domestic animals. The key reservoirs of human enteropathogens are food, water and humans, but some of these infections (e.g. Salmonella, Campylobacter and Yersinia) are zoonoses that are transmitted from live animals, or by unsafe preparation of food. Children less than 2 years of age are particularly exposed to enteric pathogens, because of poor hygiene of hands and feet, and their explorative behaviour. When exposed, they often develop gastroenteritis due the lack of immunity induced by previous infections. The transition from breastfeeding, which provides some protection against enteropathogens to formula or cow milk, also increases the risk of gastroenteritis [6].
Other direct consequences of diarrhea in children include growth faltering, malnutrition, and impaired cognitive development in resource-limited countries [7]. Ramshackle housing, lack of piped water and sanitation, widespread fecal contamination of the environment, lack of personal hygiene, high incidence of malnutrition and infection, overcrowding of children under five years of age in one house have been found to be the contributing factors [8].
Childhood mortality rate is higher in families that are poor, living in rural areas and whose mothers lack basic education. Diarrhoea is about 13% higher in rural children than urban in the age group between 6 to 23 months. Moreover, there is a higher incidence of diarrhoea in children with uneducated mothers as compared to those whose mothers have some primary education [5]. Children, especially infants, are more susceptible than adults to dehydration because of the greater basal fluid and electrolyte requirements per kg and as they are dependent on others to meet these demands [2].
Acute gastrointestinal illnesses are amongst the most common diseases worldwide: ranging from mild annoyances to devastating, dehydrating illnesses that can kill within hours [9]. AGE causes an increase loss of water and electrolytes through vomiting and diarrhea resulting to dehydration which is the main cause of mortality in children [10]. Serum electrolyte and acid base disturbances are common in under-five children with acute diarrhea but may remain unrecognized, resulting in morbidity and sometimes mortality. Of the electrolyte abnormalities observed, hyponatremia and hypokalemia ranked first and second in frequency, respectively [11]. Timely recognition, a high index of suspicion and a thorough understanding of common electrolyte abnormalities is necessary to ensure their correction [12]. Episodes of acute diarrhoea occur most commonly in the first year of life, at a time when not only brain development is incomplete, but also when the wide variety of intestinal transport mechanisms which are concerned with the absorption and secretion of fluid and electrolytes are poorly developed [13]. Samadi, et al. [14] in their study in Bangladesh reported that 20.8% were hyponatremic, 72.8% isonatremic and 6.4% were hypernatremic.
During the past three decades, factors such as the widespread availability and use of Oral Rehydration Solution (ORS), improved rates of breastfeeding, improved nutrition, better sanitation and hygiene, and increased coverage of measles immunization are believed to have contributed to a decline in the mortality rate in developing countries. However, the morbidity from diarrheal diseases has remained relatively constant during the past two decades [7]. Urea showed good specificity, and anion gap was the most sensitive laboratory parameter for assessment of dehydration.
Material and Methods
This hospital based prospective observational cross sectional study was conducted in Universal College of Medical Sciences (UCMS), a tertiary care hospital in western Nepal over a period of five months (July-Nov 2019).Detailed history, examination and investigations were recorded in specially designed proforma. Demographic profile of the patients, details of diarrhea such as duration, frequency, consistency of stools and accompanying degree of dehydration as per WHO criteria and any associated complication were recorded and investigated. Note was made about use of ORS before arriving to the hospital. A detailed examination was done by a pediatrician to assess the degree of dehydration, presence or absence of features suggestive of dyselectrolytemia and renal involvement.
The levels of serum sodium (Na+), potassium (K+), serum urea, serum creatinine, packed cell volume (PCV), hemoglobin (Hb), with total leukocyte count (TLC) along with differential leukocyte count was investigated. Serum sodium and potassium were analyzed by biochemical analyzer (Ion Selective Method) based on the principle of electrochemistry. Similarly, serum urea and creatinine concentration were determined by kinetic urease-GLDH and alkaline picrate method respectively. Chest X-ray was done when required.
Study Definitions
- Sodium level was considered normal between 135-145 mmol/L
- Potassium level was considered normal between 3.5- 5.5 mmol/L
- Blood urea was considered normal in between 15-40 mg/dl
- Serum creatinine was considered normal in the range of0.4–0.7 mg/dL in children (up to 5 years of age).
Aims and Objectives
The aims and objectives of the present study was to study the incidence and outcome of renal involvement in acute gastroenteritis in children <5 years of age and to study the relation of severity of dehydration with renal injury.
Inclusion Criteria
• All children aged one month to 5 years acute gastroenteritis admitted in the pediatric department.
Exclusion Criteria
- Any child with history of diarrhea more than two weeks at the time of admission
- Children with dysentery (blood and mucus in stool)
- Children with known pre-existing renal disease, children who underwent renal replacement therapy before admission.
Statistical Analysis
The data was entered in predesigned proforma and was analyzed with SPSS version 22 (Statistical Package for the Social Science) software. Frequency of the qualitative variables was presented in the percentage. Value of continuous variables was presented as mean±SD. Data was analyzed using Chi square test for qualitative variables and analysis of variance (ANNOVA) was used for comparison of mean of continuous variables. Odd’s ratio was calculated for risk assessment. Status of hydration biochemical variables was analyzed by Spearman’s rho correlation coefficient. P value of less than 0.05 was considered statistically significant. Results Out of total 175 admitted gastroenteritis cases, 100 children were enrolled in the study as per the inclusion criteria. Out of 100 cases enrolled 66 (66%) were males and 34(34%) were females with male to female ratio of 1.94:1 (Table 1).
| 01-12 | 13-24 | 25-36 | 37-48 | 49-60 | P-value | |
|---|---|---|---|---|---|---|
| Na+ | 136.34±4.66 | 136.47±3.82 | 134.16±4.40 | 137.15±2.92 | 135.70±3.93 | 0.2 |
| K+ | 4.00±0.76 | 3.92±0.60 | 3.63±0.55 | 4.00±0.52 | 3.71±0.59 | 0.23 |
| Urea | 35.58±25.51 | 32.57±22.58 | 44.34±26.8 | 30.66±17.47 | 40.50±23.40 | 0.39 |
| Creatinine | 0.82±0.30 | 0.87±0.41 | 1.10±0.51 | 0.83±0.13 | 1.01±0.41 | 0.08 |
| Hb | 10.08±1.52 | 10.57±1.48 | 10.82±1.92 | 11.86±1.47 | 10.50±1.57 | 0.03 |
| TLC | 12006.45±6261.51 | 13025.00±6928.07 | 14267.39±6363.70 | 12291±4592.17 | 14600.00±6127.96 | 0.69 |
| PCV | 31.16±4.21 | 33.85±6.61 | 32.72±5.61 | 35.96±3.77 | 31.75±4.50 | 0.08 |
Table 1: Level of Biochemical and Hematological Parameters in Different Age Groups (Months).
Figure 1 show that children aged 1-12 months had the highest incidence of diarrhea (31%), which was followed by 13-24 months (28%), 25-36 months (23%), and 37-48 months (12%). The age group 49-60 months had the lowest incidence (6%).
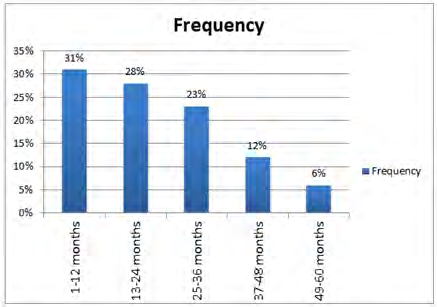
Table 2 depicts the frequency of different biochemical parameters in children with AGE. Majority of admitted children with AGE had normal urea (71%) and raised creatinine (62%). Urea was only raised in 29% of cases.
| Biochemical parameters | Frequency | |
|---|---|---|
| Serum Sodium | Normal | 58% |
| Low | 42% | |
| Serum Potassium | Normal | 67% |
| Low | 31% | |
| High | 2% | |
| Serum Urea | Normal | 71% |
| High | 29% | |
| Serum Creatinine | Normal | 38% |
| High | 62% |
Table 2: Frequency of Patients in Different Status of Electrolytes.
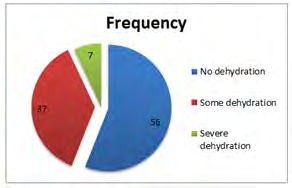
Figure 2 shows that out of 100 cases enrolled, no dehydration was observed in highest number of cases (56%) followed by some dehydration (37%) and severe dehydration (7%).
Table 3 shows serum urea and creatinine were significantly high in severe dehydration [80.26±30.56 &1.81±0.56] as compared to some dehydration [43.05±23.98 & 0.97±0.38] and no dehydration [25.69±12.59 & 0.75±0.14].
| Group 1 | Group 2 | Group 3 | p value | |
|---|---|---|---|---|
| Urea (mg/dl) | 25.69±12.59 | 43.05±23.98 | 80.26±30.56 | 0.001 |
| Creatinine (mg/dl) | 0.75±0.14 | 0.97±0.38 | 1.81±0.56 | 0.001 |
Table 3: Odd’s Ratio of renal parameters and oral rehydrating solution use.
Table 4 shows the odd`s ratio of renal parameters seen in the present study in relation to ORS use. The study suggested that there was no significant changes in renal parameters with adequate ORS use.
| OR (CI) | p-value | |
|---|---|---|
| Urea | 0.399 (0.130-1.2290) | 0.095 |
| Creat | 0.357 (0.094-1.360) | 0.100 |
Table 4: Odd’s Ratio of renal parameters and oral rehydrating solution use.
Discussion
Studies in developing countries have shown that children in the first 2 years of life may have up to 10 episodes of diarrheal disease, often with significant mortality. The total incidence of acute gastroenteritis was 7.8% in the present study.
Poo, et al. [15] reported that acute gastroenteritis was responsible for 6% of the total pediatric admission, which was comparable to this study (178 diarrheal cases out of 2236 pediatric admission). Ramanaiah, et al. [16] found that the incidence of acute diarrheal disease among under five children admitted as 12.1%, which was higher than the present study. In another study done by Yilgwan, et al. [17] in Nigeria, the incidence of acute gastroenteritis was only 2.7%, which was very much lower than the present study.
The differences in the incidence between the present study and other studies may be attributed to the differences in the time period, setting of the study and region.
A study done by Stanly, et al. [18] reported that the average number of times of diarrhea per child per day was 5 with a minimum number of 3 and maximum of 10. Kolahi, et al. [19] reported the mean frequency of diarrhea was 5.1±5 episode per day.
In the present study, majority of the admitted cases 73,
(73%) suffered from 1-2 days of diarrhea before admission followed by 25(25%) from 3-4 days. Only 2 (2%) cases suffered from diarrhea from 5-6 days. Similar result was seen in a study done by Poo, et al. [15] who reported 50% had duration of symptoms of two days or less before admission, while 76% had symptoms for less than three days.
A study done by Poo, et al. [15] reported that 37% had vomiting less than 5 times per day whereas 29% had vomiting 5-10 times per day. In the same study it was reported that 24% had vomiting more than 10 times per day.
In this study, the most common chief complaint was vomiting (88%), followed by fever (74%), distention of abdomen (26%), thirst (23%), scanty urination (23%) and convulsion (2%) . The sensorium was affected in 42% of the cases; 35% irritable and 7% lethargic.
In a study done by Azemi, et al. [20] in Kosovo, loose stool was the most frequent symptom seen in 98.59% cases, followed by vomiting in 88.02% cases which was similar to our study and fever in 54.22% cases. Poo, et al. [15] in their study reported that vomiting was present in more than 90% of children on admission and loose stool was present in all children on admission, which was comparable to our study. Similarly, Khalili, et al. [21] reported that vomiting and fever were the most frequent concomitant symptoms during presentation in hospitalized children.
The present study shows that no dehydration was observed in most number of cases (n= 56, 56%), followed by some dehydration 37(37%) and severe dehydration 7 (7%). Tavakolizadeh, et al. [22] in their study reported that among children admitted with acute gastroenteritis, 64.9% had no dehydration, 32.7% had some dehydration, which was comparable to our study, and only 2.4% cases had severe dehydration. A study done by Azemi, et al. [20] in Kosovo reported some dehydration to be present in 42.29% of cases which was comparable to our study and severe dehydration in 14.08% cases.
These findings are in agreement with prior studies demonstrating that no dehydration is present in majority of hospitalized children with acute diarrhea. The main reason for some dehydration being seen in majority of the cases following no dehydration in our study may be because of the lack of knowledge among most of the mother’s about the use of ORS in diarrhea. As it has been noted that only 15% of the cases received ORS prior to hospitalization.
In our study majority of the patients had intact sensorium in mild and when dehydration was not present whereas in severe form of dehydration majority of the patients had altered sensorium. It is seen that when there is deterioration in the status of hydration in the children, there is worsening of the sensorium as well.
In the present study, electrolyte disturbances were seen in 42(42%) cases while 58 (58%) cases had no electrolyte disturbance. The most common electrolyte disturbance was hyponatremia (42%) followed by hypokalemia in 31%. Mixed electrolytes disturbances were seen in 33(33%) of the cases out of which the most common was hyponatremia with hypokalemia seen in 75.75% cases followed by normal sodium with hypokalemia (6%). Normal sodium with hyperkalemia was seen in 2% cases. In this study isolated hyponatremia was seen in 17% cases with isolated hypokalemia in 6% and isolated hyperkalemia was seen in 2% cases. Shah, et al. [23] in their study done in pediatric ward of BPKIHS, Dharan reported 79% of children suffering from diarrhea to have some form of electrolyte abnormalities, which was found to be higher than our study. In the same study, the second common electrolyte disturbance was hypokalemia (46%), which was isolated in 14% and associated with hyponatremia in 26%. Similarly, Ukarapol, et al. [24] in Thailand found electrolyte abnormalities in 69.8% of children having acute diarrhea.
Out of 100 cases enrolled in the study, 71(71%) had normal urea, whereas 29 (29%) had increased serum urea level. The present study shows that 62 (62%) had increased serum creatinine, while 38 (38%) had normal serum creatinine level. Further, the increase in serum urea was seen in more number of cases that is in 20% in some dehydration followed by severe dehydration (6%) whereas only 3% of the cases had increase urea in no dehydration. Moreover, serum creatinine was found to be increased in no, some and severe dehydration that is, in 27%, 28% and 7% respectively.
Malaki, et al. [25] found that BUN level was significantly higher in severe dehydration compared to mild or moderate dehydration whereas there was no difference in the serum creatinine level between mild and moderate dehydration but in severe dehydration creatinine level was significantly higher. Similar result was seen in the study conducted by Ukarapol, et al. [24] where 24% of the patient had increase BUN and the BUN correlated statistically with the degrees of dehydration. On the contrary, Tavakolizadeh, et al. [22] in their study using children with acute gastroenteritis reported the most common biochemical abnormality to be abnormal serum creatinine, which was reported in 14.2% cases. Gauchan, et al. [26] reported that out of 188 cases high blood urea was found in 20 of severe dehydration as compared to 63 of some and 15 of no dehydration. Further high serum creatinine was found in 18 of severe, 79 of some and 17 of no dehydration [26].
Thus, serum urea, creatinine and BUN should be done in all children having acute gastroenteritis with no, some and severe dehydration as it may be difficult to predict which children have significant abnormalities. But these laboratory tests should not be considered as definitive predictors of dehydration.
In the present study, only 15% cases had received ORS prior to hospitalization while 85% had not. It was observed that out of 15 cases that had been on ORS, hyponatremia was seen in 10 cases; as compared to 32 cases who had not been on ORS. Likewise 10 cases had hypokalemia who had received ORS as compared to 21 cases who had not received ORS. Similarly, 22 patients had high serum urea level and 50 patients had high creatinine level when ORS was not used.
Gauchan, et al. [26] reported that out of 72 children who had been on ORS prior to admission, hypernatremia was seen in 14 (19.4%) and hyponatremia in 6 (8.3%); as compared to 13.8% and 12.9% respectively in those who had not been on ORS.
Seddique, et al. [27] reported that the use of ORS, by 65% of the subjects in their study. Similarly, in a study done by Ukarapol, et al. [24] about 60.4% had a history of ORT before admission, which was higher compared to this study. Rasania, et al. [28] reported that 69.8% of mothers knew the role of ORS during diarrhea whereas 46% of them never used ORS. In the same study it was reported that only one- third (38.7%) of the subjects could tell the correct method of ORS. Mohsin, et al. [29] reported that 76% mothers had correctly prepared ORS and 24% had prepared incorrectly.
ORS has been considered the “gold standard” of oral rehydration therapy. However, a Cochrane review which included seventeen trials (1811 participants) did not show a significant advantage of ORS over intravenous hydration in the outcome in dehydration associated with diarrhea in children. According to Nepal Demographic Health Survey (NDHS) 2011, the percentage of children treated with ORS has increased from 29% in 2006 to 39% in 2011 [18].
ORT is the cheap, simple and effective way to prevent/treat dehydration caused by diarrhea. Timely and appropriate use of ORS is associated with reduced need for hospitalizations, intravenous infusions, risk of dehydration and electrolyte abnormalities. Improper preparation and intake of ORS hampers the prevention and treatment of diarrheal diseases, and may further lead to electrolyte disturbances and contribute to morbidity and mortality. Thus, lack of use of ORS hampers the prevention and treatment of diarrheal diseases, and may further lead to electrolyte disturbances and contribute to morbidity and mortality. Thus, lack of use of ORS in cases of diarrhea is considered as a risk factor as identified by the present study.
Conclusion
The level of serum sodium and potassium decreased and urea and creatinine increased with severity of dehydration. In this study majority of cases (85%) was not on ORS and had low sodium and potassium. Thus, electrolyte disturbances are one of the major concerns among children with acute gastroenteritis and timely recognition and correction is necessary to prevent morbidity and mortality. Early diagnosis and urgent management of gastroenteritis and dehydration can prevent AKI.
References
-
Guarino A, Ashkenazi S, Gendrel D, Lo Vecchio A, Shamir R, et al. (2014) European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases Evidence-Based Guidelines for the Management of Acute Gastroenteritis in Children in Europe: Update 2014. J Pediatr Gastroenterol Nutr 59(1): 132-152.
-
Bhutta ZA (2011) Acute Gastroenteritis in Children. In: Kliegman RM, Behrman RE, Stanton BF, Schor NF, Geme JWS, (Eds.), Nelson Textbook of Paediatrics, 19th (Edn.), Saunders Elsevier, Philadelphia, pp: 1323.
-
Ibrahim BM (2012) Isolation of Some Microbial Agents That Cause Acute Gastroenteritis in Children. J Fac Med Baghdad 54(3): 218-222.
-
Pokharel M, Sherchand JB, Upreti HC, Katuwal A, Gauchan P (2009) A Perspective Study on the Etiology of Diarrhea in Children Less than 12 Years of age attending Kanti Children’s Hospital. J Nepal Paediatr 29(1): 10-16.
-
Ansari M, Palaian S, Izham M, Ibrahim M (2009) The Millennium Development Goals Report: United Nations Department of Economic and Social Affairs (DESA) 2008. The Role of Mothers in the Management of Childhood Diarrhoea in Nepal. Australasian Medical Journal 1(14): 235.
-
Kabayiza JC (2014) Acute Gastroenteritis in Rwandan Children under five years of age Investigated by Real-time PCR. Depart of Infect Disease, Gothenburg University, pp: 1-81.
-
Farthing M, Salam M, Lindberg G, Dite P, Khalif I, et al. (2013) Acute Diarrhea in adults and children: A Global Perspective. J Clin Gastroenterol 47(1): 12-20.
-
Karki A, Tiwari BR (2007) Prevalence of Acute diarrhea in Kathmandu Valley. J Nepal Med Assoc 46(168): 175- 179.
-
Ukey UU, Shekhar R, Ganesh L (2012) Seasonal Patterns in Acute Gastroenteritis in a Hospital at Maharashtra, India. IJHSR 1(2): 101-108.
-
Wambui NM (2014) Barriers to Appropriate Home Management of Acute Gastroenteritis by Caregivers of Children under Five Years Attending Mbagathi District Hospital, pp: 1-109.
-
Onyiriuka AN, Iheagwara EC (2015) Serum Electrolyte Profiles of under-five Nigerian Children admitted for Severe Dehydration due to Acute Diarrhea. Niger J Health Sci 15: 14-17.
-
Shah GS, Das BK, Kumar S, Singh MK, Bhandari GP (2007) Acid Base and Electrolyte Disturbance in Diarrhea. KUMJ 5(17): 60-62.
-
Whyte LA, Jenkins HR (2012) Pathophysiology of diarrhea (Review).Paediatrics and Child Health 22(10): 443-447.
-
Samadi AR, Wahed MA, Islam MR, Ahmed SM (1983) Consequences of Hyponatraemia and Hypernatraemia in Children with Acute Diarrhoea in Bangladesh. Br Med J (Clin Res Ed.) 286(6366): 671-673.
-
Poo MI, Lee WS (2007) Admission to hospital with childhood acute gastroenteritis in Kuala Lumpur, Malaysia. Med J Malaysia 62(3): 189-193.
-
Ramanaiah VD, Arumugam SN A, Prabhu R (2015) Sociodemographic profile of acute diarrhoeal diseases in a tertiary care hospital, Tirupati. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) 14(5): 29-32.
-
Yilgwan CS, Okolo SN (2012) Prevalnce of diarrhea disease and risk factors in Jos University Teaching Hospital, Nigeria. Ann Afr Med 11(4): 217-221.
-
Stanly AM, Sathiyasekaran BWC, Palani G (2009) A Population based study of Acutediarrhoea among children under 5 years in a rural community in South India. Sri Ramachandra Journal of Medicine 1(1): 1-6.
-
Kolahi AA, Nabavi M, Sohrabi MR (2008) Epidemiology of acute diarrheal diseases among children under 5 years of age in Tehran, Iran. Archives of Clinical Infectious Diseases 3(4): 193-198.
-
Azemi M, Berisha M, Ismaili-Jaha V, Kolgeci S, Avdiu M, et al. (2013) Socio-demographic, Clinical and Laboratory features of Rotavirus Gastroenteritis in Children Treated in Pediatric Clinic. Mat Soc Med 25(1): 9-13.
-
Khalili B, Shahabi G, Khalili M, Mardani M, Cuevas LE (2006) Risk factors for hospitalization of children with diarrhea in Shahrekord, Iran. Iranian Journal of Clinical Infectious Diseases 1(3): 131-136.
-
Tavakolizadeh R, Sadeghi M, Namiranian N, Fahimi D, Barkhordari M (2013) Blood chemical analysis in children with acute gastroenteritis, When Is It Useful?. J Ped nephrology 1(2): 65-69.
-
Shah GS, Das BK, Kumar S, Singh MK, Bhandari GP (2007) Acid Base and Electrolyte Disturbance in Diarrhea. KUMJ 5(17): 60-62.
-
Ukarapol N, Wongsawasdi L, Chartapisak W, Opastirakul S (2002) Electrolyte Abnormalities In Children With Acute Diarrhea. Chiang Mai Med Bull 41(1): 7-12.
-
Malaki Majid (2012) Clinical versus laboratory for estimating of dehydration severity. Annals of Tropical Medicine and Public health year 5(6): 559-562.
-
Gauchan E, Malla KK (2015) Relationship of Renal Function Tests and electrolyte levels with severity of dehydration in acute diarrhea. J Nepal Health Res Counc 13(29): 84-89.
-
Ranjbar SA, Bavafa B (2007) Iranian mother’s child feeding practices during diarrhea: A study in Kerman. Pak J Nutrion 6(3): 217-219.
-
Rasania SK, Singh D, Pathi S, Matta S, Singh S (2005) Knowledge and Attitude of mothers about Oral Rehydration Solution in few urban slum of Delhi. Health and Population - Perspectives and Issues 28(2): 100- 107.
-
Mohsin A, Raza AB, Ahmad TM (2012) Knowledge, Attitude and Practices of the mothers regarding Oral Rehydration Solution, Feeding and use of drugs in childhood diarrhoea. P J M H S 6(1):108.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?