Neonatal Sepsis Caused by Listeria Monocytogenes at the San Jeronimo De Monteria Hospital: About a Case
Case Presentation: The clinical and paraclinical findings that led to the diagnosis, the paraclinical follow-up of the infectious picture, the treatment established and the outcome of resolution of the disease are included. A review of the literature is carried out on the infectious and epidemiological characteristics of L. monocytogenes infection, as well as its clinical presentation and repercussions during the gestational period and in the neonatal stage. Discussion: neonatal listeriosis is a highly lethal disease, whose epidemiology is not clearly described at the national and regional level, which makes it difficult to create prevention strategies in high-risk groups. It is suggested to make this infection a mandatory notification event to allow the identification of risk factors, lethality, outcome and usual presentation of this infectious disease in Colombia.
Introduction
Listeria monocytogenes is a rare pathogen in the general population, with an annual incidence that varies between 0.1 and 11.3 cases per million people, mainly associated with secondary outbreaks due to contamination of food and beverages; It can cause severe infections in the population at risk, which includes people with diabetes mellitus, those who are immunosuppressed, pregnant, and at extreme ages of life, such as neonates [1].
The importance of listeriosis is not sufficiently recognized since it is a relatively rare disease, in fact, it is considered a rare disease and as such, included in ORPHANET, the European Consortium for Orphan Diseases and Medicines with the reference ORPHA533 [2]. It does not present specific clinical manifestations neither in the mother nor in the new-born. During pregnancy it assumes various clinical forms: pseudo-flu, flu-like and latent. In the NB, its symptoms are equally varied and the infection is not recognized quickly enough to carry out a quick and timely treatment [3]. The objective of our work is to provide a new case of early presentation of neonatal listeriosis and to make some general considerations of interest about this condition and neonatal sepsis [4].
Case Report
New-born of 35 weeks of gestation and 2250grams, who was decided to hospitalize in the san jeronimo de monteria hospital after presenting a history of urinary tract infection, premature rupture of membranes of 12hours and respiratory difficulty, considering a high risk of sepsis due to her history. On admission, she presented a general state with a tint of jaundice without cyanosis, respiratory distress with striking moans, normal heart tone, normal BP. There was no hepatosplenomegaly or neurological depression.
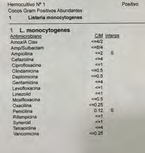
Among the analytical data, a bilirubin report stands out for BT: 11.31 MG/DL, BD: 0.63 MG/DL, BI: 10.68 MG / DL. As a result of the above, phototherapy is started for jaundice and evolution is monitored. Due to suspected infection, antibiotic treatment with ampicillin (110GR every 12hours) and gentamicin (10 GR every 24 hours) is started. Among the complementary tests performed urgently, a normal CRP (1.9 mg/l), marked leukocytosis (20,400/mm3) stood out, later the positivity of the blood culture to Listeria monocytogenes sensitive to ampicillin and penicillin was confirmed (Figure 1). The culture of the peripheral smears and the CSF were negative. She received antibiotic treatment with ampicillin that was later replaced by amoxicillin (250 MG orally every 8 hours) and gentamicin that was maintained for 14 days, with support with oxygen support through a cephalic chamber at 8 litters per minute, with 100% Fio2, the evolution being favourable.
Discussion
Neonatal listeriosis has an approximate occurrence of 2.3 to 8.6 cases per 100,000 live births in the United States and Western Europe and, despite adequate antibiotic treatment; the fatality associated with listeriosis is close to 30%. L. monocytogenes is the third etiological agent implicated in neonatal meningitis in Western countries, with a fatality ranging between 3% and 60% and pregnant women have a 13 to 20times higher risk of suffering from listeriosis, compared to with non-pregnant women. Neonatal death occurs in one fifth of maternal infections; additionally, about 60% of neonates who survive to delivery of a woman who has suffered from listeriosis will develop neonatal infection [5]. The definitive diagnosis is established by blood culture and/or culture of skin lesions. Listeria grows well on blood agar and other conventional enriched culture media and can be confused with hemolytic streptococci or enterococci. Serological studies are not useful for diagnosis [6].
The treatment of choice is ampicillin, better associated with gentamicin in severe cases. Listeria is also sensitive to penicillin, erythromycin, and tetracyclines, but not to cephalosporins. To avoid infection during pregnancy, pregnant women should refrain from eating fresh cheese and undercooked meats. If Listeria grows on vaginal smear cultures, it must be eradicated before delivery [7].
Conclusion
Neonatal listeriosis is an infection with a high lethality, despite the correct and timely antibiotic treatment established, for which all health professionals must know, prevent and in some cases treat this pathology in the fastest and most effective way to avoid complications and sequelae, since it is important to have adequate knowledge of this pathology to know when a case can be suspected, to identify it and to give it timely management [8].
Conflicts of Interest
The authors do not declare any conflict of interest.
Authors Contribution
All the authors contributed to this work. All of them have read and approved the manuscript.
References
-
Gelbicova T, Kolackova I, Pantucek R, Karpiskova R (2015) A novel mutation leading to a premature stop codon in inlA of Listeria monocytogenes isolated from neonatal listeriosis. New Microbiol 38(2): 293-296.
-
Dyatlov VA, Lawrence DA (2002) Neonatal lead exposure potentiates sickness behavior induced by Listeria monocytogenes infection of mice. Brain Behav Immun 16(4): 477-492.
-
Anand V, Holmen J, Neely M, Pannaraj PS, Bard JD (2016) The brief case: neonatal meningitis caused by Listeria monocytogenes diagnosed by multiplex molecular panel J Clin Microbiol 54(12): 2846-2849.
-
Tortajada C, Porta R, Riba M, Santoma MJ, Palacin E, et al. (2012) Brote nosocomial por Listeria monocytogenes en una Unidad de Neonatos. Enfermedades Infecciosas y Microbiologia Clínica 30(3): 143-146.
-
Torres KJ, Sierra SC, Poutou RA, Vera H, Carrascal AK, et al. (2004) Incidencia y diagnostico de Listeria monocytogenes; microorganismo zoonotico emergente en la industria de alimentos.
-
Sapuan S, Kortsalioudaki C, Anthony M, Chang J, Embleton ND, et al. (2017) Neonatal listeriosis in the UK 2004-2014. J Infect 74(3): 236-242.
-
Siegman-Igra Y, Levin R, Weinberger M, Golan Y, Schwartz D, et al. (2002) Listeria monocytogenes infection in Israel and review of cases worldwide. Emerging Infect Dis 8(3): 305-310.
-
Rodriguez-Auad JP (2018) Panorama de la infeccion por Listeria monocytogenes. Revista chilena de infectologia 35(6): 649-657.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?