Prevalence of Urinary Tract Infection and its Related Factors in a Sample of School Age Children from Baghdad Iraq
Background: Urinary tract infection is considered an important risk factor for the development of renal insufficiency or endstage renal disease. Children have a wide variety of clinical presentation, ranging from the asymptomatic presence of bacteria in the urine to potentially life- threatening infection of the kidney. Objective: To measure the prevalence of urinary tract infection, bacteriuria whether symptomatic or not, the type of bacteria detected in urine, and to identify the factors that may be associated with urinary tract infection in primary in school going children. Methodology: A cross-sectional study with analytic elements was conducted within five months in pediatric department of Al Imamain Kadhimain Medical city. A consecutive sample of 300 children of school age (6-12) years old included, data were collected by direct interview with children and/or their caregiver using a questionnaire with measurement of weight and height, general urine examination and urine culture were done. Results: The prevalence of children having positive urine culture was 14.7% of which 1.6% was of children without any symptoms. E.coli being the most frequent detected organisms 65.9%, with significant predisposing behaviors including: intake of carbonated beverages, holding back urine, not washing hands after toilet and using tight clothing. Conclusion: The prevalence of urinary tract infection among school age children in is relatively low and it is significantly related to school dropout, low educational level of parents, rural residence, and low family income.
Introduction
Urinary tract infection (UTI) has been considered an important risk factor for the development of renal insufficiency or end-stage renal disease [1]. It is one of the most common bacterial infections encountered by clinicians in developing countries [2]. Approximately 3–5% of girls and 1% of boys have UTI. Symptomatic UTI are reported in 7.8 and 1.6% of school-aged girls and boys, respectively [3]. Current observations and information point out that UTI are more often seen in females than in males. 10–35% of females have a UTI at least once in a lifetime and in 5% it recurs within 1–2 years, the main cause being due to the short urethra and feces contamination which easily leads to infection, also UTI more common in uncircumcised males. Holding back urine in the bladder, not paying attention to hygiene in the genital area, and failure in protective mechanisms in the bladder are other reasons that increase the risk of UTI [3]. It is very necessary to identify children with UTI and treat them as soon as possible to avoid any long-term complications and to reduce the risk of any significant morbidity. However, data about UTI among primary school age children is infrequent especially in Iraq, for that this study was justified to measure the rate of urinary tract infection and its related factors in a sample of children of school age attending Al-Imamein Kadhimaein Medical city. As well as to detect bacteriuria in urine culture whether symptomatic or not and identify the type of bacteria detected in urine.
Methodology
A descriptive, cross-sectional design with an analytic element was adopted for this study. A consecutive sample of school age (6-12) years old recruited from pediatric department outpatient clinic of Al-Imamain Kadhimain Medical city from 15th January-July 2020. The sample size was estimated according to the equation of sample size calculation [4] N=Z2P(Q)/W2 =278 taking a prevalence (P) of 7% [5], 5% level of confidence (Z), and 3% precision (W) (effect size). Any child in the specified age not using antibiotic within last week for any reason was invited to participate in the study. Data were collected by direct interview with children and/or their caregiver using a questionnaire prepared by the researchers after reviewing related literature [2, 3, 4, 5, 6]. It includes three dimensions covering socio-demographic characteristics, risk behaviors like daily water intake, holding back urine, prior history of UTI, familial history of the infection and personal hygiene of students, and asking about UTI symptoms. All children enrolled in the study were asked to provide mid-stream urine specimens after implementing standard precautions of clean catch urine specimen for general urine exam, culture and antibiotic sensitivity. Also body weight and height of the child were measured. Prior to data collection, students, care givers were informed about the purpose of the study, the procedures, the right of voluntary participation, keeping confidentiality and their oral consent were obtained. Data were coded, entered and analyzed using SPSS (Statistical Packages for Social Sciences, IBM, version 20). Descriptive data were expressed as means and standard deviations for continuous measurements and as frequencies and percentages for categorical measurements. Chi-square test or Fisher exact test was used to test the association of categorical data. P- Value of less than 0.05 was considered statistically significant.
Results
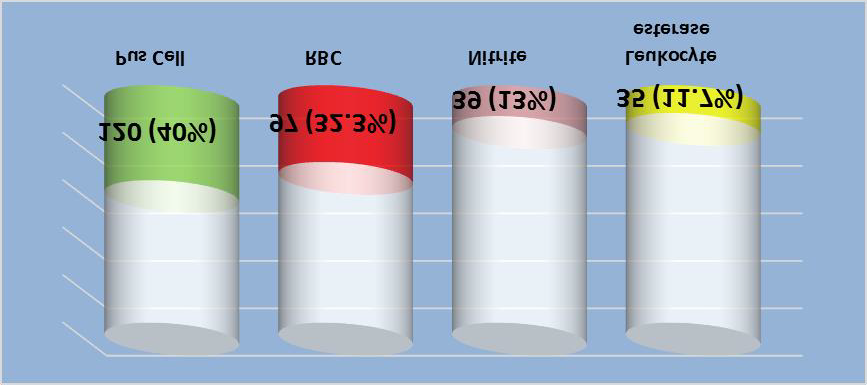
A total of 300 school age children were recruited for this study, their mean age was 9.34 ± 1.64 years with girls to boy’s ratio of 1.27:1. The mean calculated BMI was 23.32 ± 4.57 kg/m2, and more than half of them 173 (57.7%) had normal BMI level. Concerning child grade at school, about one quarter of the children 74 (24.7%) was at 4th grade. More than half of the children 156 (52%) gave history of previous UTI, 196 (65.3%) were with positive family history of UTI, 261 (87%) and 286 (95.3%) had no chronic diseases or renal problems, respectively. Circumcision was done for all of the 132 recruited boys. Results of GUE revealed pyuria, hematuria, nitrites, and leukocyte esterase were positive in 120 (40%), 97 (32.3%), 39 (13%), and 35 (11.7%) of urine samples, respectively (Figure 1).
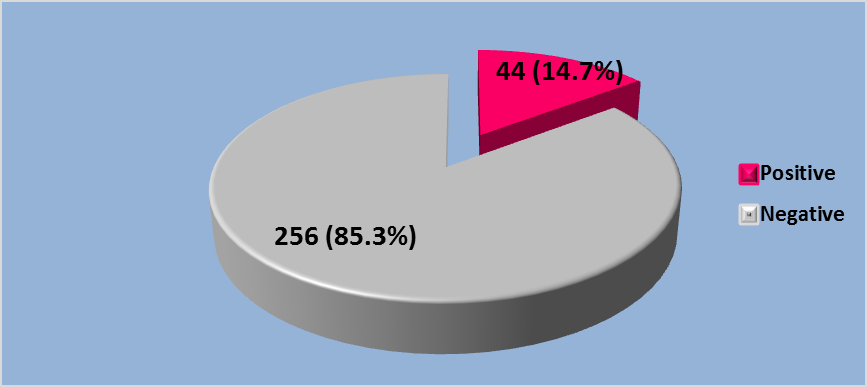
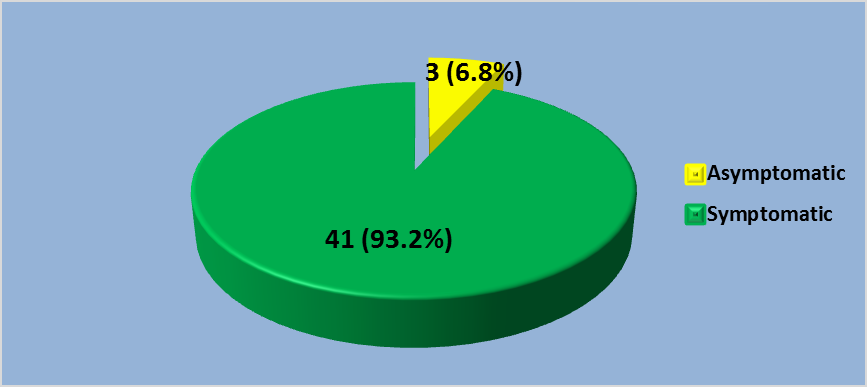
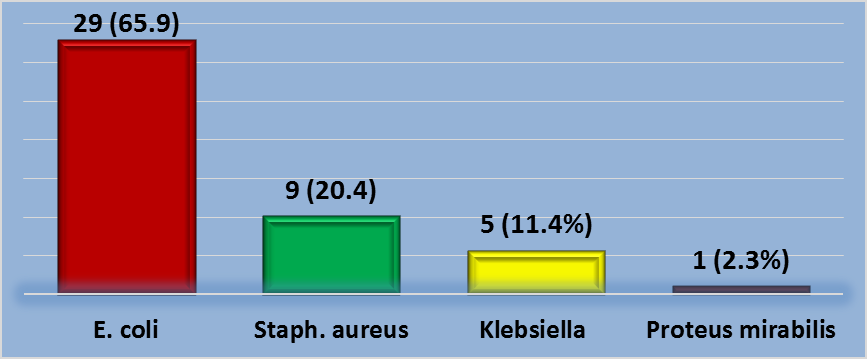
On the other hand, out of the 300 enrolled children, 44 (14.7%) had positive urine culture of which three (6.8%) of these positive cultures were of children without any symptoms. Concerning bacterial growth, E.coli being the most frequent detected organisms 29 (65.9%), followed by Staphylococcus aureus 9 (20.4%), and Klebsiella 5 (11.4%), while only one case (2.3%) was with Proteus mirabilis growth, as shown in (Figures 2-4).
The proportion of UTI was significantly higher among children who are not in school (85.7%, P= 0.001), their parents of lower educational level (21%, P= 0.038 for mothers and 26.6%, P= 0.001 for fathers, respectively), living in rural area (20.7%, p= 0.019), and with monthly income of less than one million Dinars (17.4%, P= 0.038). Age and gender of child, BMI level and the occupation of parents didn’t show a statistical significant association with UTIs (Table 1).
| General Characteristics | UTI | Total (%) n= 300 | P- Value | |
|---|---|---|---|---|
| Yes (%) n= 44 | No (%) n= 256 | |||
| Child’s age (Years) | ||||
| 6 – 9 | 21 (13.7) | 132 (86.3) | 153 (51.0) | 0.638NS |
| > 9 | 23 (15.6) | 124 (84.4) | 147 (49.0) | |
| Gender | ||||
| Male | 17 (12.9) | 115 (87.1) | 132 (44.0) | 0.438NS |
| Female | 27 (16.1) | 141 (83.9) | 168 (56.0) | |
| Child’s grade at School | ||||
| Not in School | 6 (85.7) | 1 (14.3) | 7 (2.3) | 0.001** |
| 1st Grade | 5 (12.2) | 36 (87.8) | 41 (13.7) | |
| 2nd Grade | 4 (8.2) | 45 (91.8) | 49 (16.3) | |
| 3rd Grade | 9 (15.5) | 49 (84.5) | 58 (19.3) | |
| 4th Grade | 13 (17.6) | 61 (82.4) | 74 (24.7) | |
| 5th Grade | 2 (5.3) | 36 (94.7) | 38 (12.7) | |
| 6th Grade | 5 (15.2) | 28 (84.8) | 33 (11.0) | |
| BMI Level | ||||
| Underweight | 10 (27.8) | 26 (72.2) | 36 (12.0) | 0.082NS |
| Normal | 25 (14.5) | 148 (85.5) | 173 (57.7) | |
| Overweight | 7 (10.6) | 59 (89.4) | 66 (22.0) | |
| Obese | 2 (8) | 23 (92) | 25 (8.3) | |
| Mother’s education | ||||
| Primary | 22 (21.0) | 83 (79.0) | 105 (35.0) | 0.038* |
| Secondary | 21 (12.5) | 147 (87.5) | 168 (56.0) | |
| High | 1 (3.7) | 26 (96.3) | 27 (9.0) | |
| Mother’s occupation | ||||
| Employee | 2 (5.1) | 37 (94.9) | 39 (13.0) | 0.071NS |
| Not Working | 42 (16.1) | 219 (83.9) | 261 (87.0) | |
| Father’s education | ||||
| Primary | 17 (26.6) | 47 (73.4) | 64 (21.3) | 0.001** |
| Secondary | 23 (15.1) | 129 (84.9) | 152 (50.7) | |
| High | 4 (4.8) | 80 (95.2) | 84 (28.0) | |
| Father’s Occupation | ||||
| Professional | 4 (7.1) | 52 (92.9) | 56 (18.6) | 0.096NS |
| Governmental Employee | 4 (10.5) | 34 (89.5) | 38 (12.7) | |
| Self-employee | 32 (19.2) | 135 (80.8) | 167 (55.7) | |
| Military | 4 (10.3) | 35 (89.7) | 39 (13.0) | |
| Residence | ||||
| Urban | 20 (10.9) | 164 (89.1) | 184 (61.3) | 0.019* |
| Rural | 24 (20.7) | 92 (79.3) | 116 (38.7) | |
| Monthly Income | ||||
| < 1 Million | 37 (17.4) | 176 (82.6) | 213 (71.0) | 0.038* |
| ≥ 1 Million | 7 (8.0) | 80 (92.0) | 87 29.0) |
Table 1: Association between socio-demographic characteristics of the sample with the occurrence of UTI.
*P<0.05, **P<0.01 Significant by Chi square test, NS= Not Significant. Table 1: Association between socio-demographic characteristics of the sample with the occurrence of UTI.
It was obvious that, previous history and family history of UTIs, and having a diagnosed chronic diseases or renal problems were significantly associated with current UTIs. The proportion of UTIs was significantly higher among children who had previous history of UTI (26.9%, P= 0.001), family history of UTI (17.9%, P= 0.039), diagnosed chronic diseases (51.3%, P= 0.001), diagnosed renal problems (42.3%, P= 0.002) and having encopresis (87.5%, P= 0.001) (Table 2).
| Previous History | UTI | Total (%) n= 300 | P- Value | |
|---|---|---|---|---|
| Yes (%) n= 44 | No (%) n= 256 | |||
| History of UTI | ||||
| Yes | 42 (26.9) | 114 (73.1) | 156 (52.0) | 0.001 |
| No | 2 (1.4) | 142 (98.6) | 144 (48.0) | |
| Family History of UTI | ||||
| Yes | 35 (17.9) 161 (82.1) | 161 (82.1) | 196 (65.3) | 0.039 |
| No | 9 (8.7) 95 (91.3) | 95 (91.3) | 104 (34.7) | |
| Diagnosed Chronic Disease | ||||
| Yes | 20 (51.3) | 19 (48.7) | 39 (13.0) | 0.001 |
| No | 24 (9.2) | 237 (90.8) | 261 (87.0) | |
| Diagnosed Renal Problem | ||||
| Yes | 6 (42.9) | 8 (57.1) | 14 (4.7) | 0.002 |
| No | 38 (13.3) | 248 (86.7) | 286 (95.3) | |
| Chronic Constipation | ||||
| Yes | 7 (26.9) | 19 (73.1) | 26 (8.7) | 0.08 |
| No | 37 (13.5) | 237 (86.5) | 274 (91.3) | |
| Encopresis | ||||
| Yes | 7 (87.5) | 1 (12.5) | 8 (2.7) | 0.001 |
| No | 37 (12.7) | 255 (87.3) | 292 (97.3) | |
| Pinworm Infestation | ||||
| Yes | 12 (12.6) | 83 (87.4) | 95 (31.7) | 0.498 |
| No | 32 (15.6) | 173 (84.4) | 205 (68.3) | |
| Risk behaviors | UTI | Total (%) n= 300 | P- Value | |
| Yes (%)n= 44 | No (%)n= 256 | |||
| Daily Water Intake | ||||
| < Liter | 21 (12.1) | 153 (87.9) | 174 (58.0) | 0.135 |
| ≥ Liter | 23 (18.3) | 103 (81.7) | 126 (42.0) | |
| Taking Carbonated Beverages | ||||
| Yes | 41 (16.6) | 206 (83.4) | 247 (82.3) | 0.041 |
| No | 3 (5.7) | 50 (94.3) | 53 (17.7) | |
| Holding Back Urine | ||||
| Yes | 36 (18.0) | 164 (82.0) | 200 (66.7) | 0.023 |
| No | 8 (8.0) | 92 (92.0) | 100 (33.3) | |
| Using School Bath for Urination | ||||
| Every Day | 8 (17.8) | 37 (82.2) | 45 (15.0) | 0.195 |
| 2-3 Times/ Week | 4 (7.3) | 51 (92.7) | 55 (18.3) | |
| Once/ Week | 24 (19.4) | 100 (80.6) | 124 (41.4) | |
| Never | 8 (10.5) | 68 (89.5) | 76 (25.3) | |
| Washing Hands After Toilet | ||||
| Yes | 37 (13.3) | 241 (86.7) | 278 (92.7) | 0.018 |
| No | 7 (31.8) | 15 (68.2) | 22 (7.3) | |
| Using Tight Clothing | ||||
| Yes | 31 (18.9) | 133 (81.1) | 164 (54.7) | 0.023 |
| No | 13 (9.6) | 123 (90.4) | 136 (45.3) |
Table 2: Association between past medical and surgical history and occurrence of UTI.
*P<0.05, **P<0.01 Significant by Chi square test, NS= Not Significant. Table 2: Association between past medical and surgical history and occurrence of UTI.
Regarding the association between UTI and certain risk behaviors of the enrolled children, a statistically significant association was found between the occurrence of UTI and taking carbonated beverages (P= 0.001), holding back urine (P= 0.004), not washing hands after toilet (P= 0.018), and using tight clothing (P= 0.023) (Table 3).
* P<0.05, **P<0.01 Significant by Chi square test, NS= Not Significant. Table 3: Association of UTI according to the risk behaviors.
Discussion
The present study found that prevalence of urinary tract infection among school age children in Al Imamein Kadhimaein Medical city was (14.7%). This rate is close to results of Kareem and Issa descriptive cross sectional study in Iraq [2] which found that 18.3% of children from five hospitals in Basra city had positive urine culture, but far less than the rate found in another Iraqi study conducted in Tikrit city in 2012 that revealed culture positive rate in school age children to be 42.9% [7]. On the other hand, the current study prevalence of (14.7%) is higher than the prevalence among school age children of (6%) that was reported by Mohammed, et al. [3] study in Egypt on 1000 school age children and the results of Zincir, et al. [5] cross sectional study in Turkey on 2,511 school students which showed a prevalence of (7.1%), while lower than results of Isa, et al. [8] study in Nigeria which revealed that (31.7%) primary school age children had positive urine culture for bacterial growth.
These differences in rates of urinary tract infection among school age children might be attributed to differences in socioeconomic status, culture, personal hygiene, health infrastructure and school health services between different communities. Additionally, the rate reported by present study is representative for symptomatic UTI, while for asymptomatic UTI the rate was 1.6% from our sample that is lower than results of Al-Rawi study in Iraq [9] who reported a prevalence of (6.6%) for asymptomatic urinary tract infection among school children and results of Kumar, et al. [10] study in India which found a positive asymptomatic bacteriuria among (10.57%) of school age children. However, Shaikh, et al. [11] meta-analysis study in USA reported that prevalence of asymptomatic bacteriuria was 0.37% in boys and 0.47% in girls. In current study, E. coli was the most common bacterial organism (65.9%). This finding is close to results of Abdul-Mohammed, et al. [12] study in Iraq which reported that main bacterial growth findings of Iraqi children were E. coli (44.8%).Other Iraqi studies also documented the same causative microorganisms of urinary tract infection commonly the E. coli but with different proportions [2, 7, 9, 13]. Our study findings are similar to results of Hameed, et al. [14] retrospective review study in Saudi Arabia on 202 children which found that E. coli was the most common pathogen causing UTI among children.
This study showed no significant association between the age and gender of the child and having UTI. This is inconsistent with results of Shaikh, et al. [11] study in USA which reported that prevalence of UTI among children varied by age, gender, race and circumcision status. This finding is also inconsistent with results of many literatures such as Al- Qaidi, et al. [7] study in Iraq and Magliano, et al. [15] study in Italy which all documented that female gender school age children were more prone for UTI than male school age children and this risk may be related to anatomical reasons and pubertal differences. The present study showed a statistically significant association between UTI and children who were not engaged in school (school dropouts). This finding coincides with results of Abu Salem, et al. [16] study in Egypt which stated that school dropout children were at high risk of nocturnal enuresis and recurrent urinary tract infections. Low mothers’ education in current study is significantly related to high risk of UTI among school age children (P=0.001). This finding is similar to results of Abu Salem, et al. [16] study in Egypt. Also low fathers’ educational level is significantly related to higher risk of UTI among school age children (P=0.001) in our findings. This finding coincides with results of Hashem, et al. [17] study in Iran which stated that low educational level of parents is a significant risk factor for nocturnal enuresis and high risk of UTI among school age children. The educational level of parents is related to socioeconomic status, culture, personal hygiene which all affect the health behavior and hygiene of the children.
The present study found a significant association between rural residence of children and high risk of UTI (P=0.01). Consistently, Hussein, et al. [18] descriptive study in Erbil found a significant difference in prevalence of UTI among students between urban and rural areas and it also reported that culture of hand washing in urban areas was the common preventive method of UTI. The present study also found that school age children from low income families were significantly at higher risk of UTI (P=0.03). This finding is similar to results of Leung, et al. [19] study in Canada which revealed a significant relationship between low socioeconomic status of families and higher risk of UTI among school age children. Our study found that having a previous history of UTI was significantly related to higher risk of UTI (P=0.001). Similarly, Al-Rikabi and Abu-Raghif descriptive study in Iraq [20] on 120 prepubertal children from primary schools in Nasiriya city found that previous history of UTI is a significant risk factor for current UTI among school age children. The previous history of UTI may be an indicator for asymptomatic UTI, incompetent treatment, antibiotics resistance and poor personal hygiene. Also we found a significant association between family history of UTI and higher risk of UTI among school age children (P=0.03). This finding is similar to results of Zincir, et al. [5] study in Turkey which revealed that diagnosed UTI in family would be a significant risk factor for UTI among school age children.
In the current study results showed that having a diagnosed chronic disease was significantly related to higher risk of UTI (P=0.001) This finding is in agreement with reports of White study in USA [21] which documented that school age children with other chronic diseases especially type I diabetes mellitus would be at increased risk of UTI. Also our study showed a significant relationship between diagnosed renal problems and higher risk of UTI among school age children (P=0.002). This finding coincides with results of Al-Rikabi and Abu-Raghif descriptive study in Iraq [20] and Barakat study in USA [22] which stated that most school age children with renal disorders or anomaly presented with severe UTI. In this study results showed that the significant risky behaviors for UTI among school age children were intake carbonated beverages (P= 0.001), holding back urine (P= 0.004), not washing hands after toilet (P= 0.01), and using tight clothing (P= 0.02). These findings are in agreement with results of many studies such as Al- Rikabi and Abu-Raghif descriptive study in Iraq [20] and Sivaraj, et al. [23] study in India which reported that voiding dysfunction, poor personal hygiene and tight clothing are the common risk factors for UTI among school age children. Miller, et al. [24] study in USA stated that elimination of carbonated beverages intake is helpful in improving the lower urinary tract symptoms. The main limitations of present study were the cross sectional design in which the temporal relationship cannot be assessed, single center study and hospital based sample make it less representative to the general population.
Conclusions
- The rate of urinary tract infection among school age children in Al Imamein Kadhimaein Medical city is relatively low.
- The main pathogen responsible for urinary tract infection among school age children is E. coli.
- Urinary tract infection among school age children is significantly related to school dropout, low educational level of parents, rural residence, and low family income.
- The significant predisposing behaviors for urinary tract infection among school age children are intake carbonated beverages, holding back urine, not washing hands after toilet and using tight clothing.
- The predictors for urinary tract infection among school age children are significantly related to previous history of urinary tract infection, other renal problems, family history of urinary tract infection and history chronic disease.
References
-
Kligman RM (2019) Urinary Tract Infection. In: Joseph St. Geme (Eds.), Nelson Textbook of Pediatrics, 21st (Edn.), WB Sounder, Philadelphia pp: 3876.
-
Kareem NA, Issa SS (2017) Prevalence of Urinary Tract Infection in Children from One to Fifteen Years Old in Basra City in 2014. Journal of Health, Medicine and Nursing 36: 105-112.
-
Kligman RM (2018) In: Jenson HB (Eds.) Nelson Essentials of Pediatrics, 8th (Edn.), Elsevier Sounder, Philadelphia, pp: 414-415.
-
Pourhoseingholi MA, Vahedi M, Rahimzadeh M (2013) Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench 6(1): 14-17.
-
Zincir H, Erten ZK, Ozkan F, Sevig U, Baser M, et al. (2012) Prevalence of urinary tract infections and its risk factors in elementary school students. Urol Int 88(2): 194-197.
-
Sahin A, Ardahan M (2008) Determining urinary tract infections and affecting factors in primary school students. TTB Cont J Med Educ 17: 67-75.
-
AL-Qaidi HSA, Jasim TM, AL-Mazruai IAH (2012) Urinary Tract Infection among Children’s Under (12) Years Old In Tikrit City. AJPS 12(2): 171-177.
-
Isa M, Ismail H, Allamin I, Shettima A, Mustapha (2013) A Prevalence Of Urinary Tract Infection Among Primary School Children In Maiduguri, Borno State, Nigeria. International Journal of Environment 2(1): 9-15.
-
Al Rawi JR (2003) Prevalence of asymptomatic urinary tract infection among primary school children in Iraq [Hilla], Yemeni J Med Sci 3(2): 20-25.
-
Kumar CS, Jairam A, Chetan S, Sudesh P, Kapur I, et al. (2002) Asymptomatic bacteriuria in school age children. Indian J Med Microbiol 20(1): 29-32.
-
Shaikh N, Osio VA, Wessel CB, Jeong JH (2020) Prevalence of Asymptomatic Bacteriuria in Children: A Meta- Analysis. J Pediatr; 217:110-117.
-
Abdul-Mohammed HS, Mohammed AK, Hussein RAR (2012) The frequency of urinary tract infection according to age and sex in some of Iraqi children. Al-Taqnia 25(7): 9-15.
-
Hussein NH, Rasool KH, Taha BM, Hussein JD (2017) Prevalence And Antimicrobial Susceptibility Patterns Of Bacteria Isolated From Urinary Tract Infections (UTIs) In Children At Children Hospital In Baghdad. Al- Kindy College Medical Journal 13(1): 102-107.
-
Hameed T, Al-Nafeesah A, Chishti S, Al-Shaalan M, Al-Fakeeh K (2019) Community-acquired urinary tract infections in children: Resistance patterns of uropathogens in a tertiary care center in Saudi Arabia. Int J PediatrAdolesc Med 6(2): 51-54.
-
Magliano E, Grazioli V, Deflorio L, Leuci AI, Mattina R, et al. (2012) Gender and age-dependent etiology of community-acquired urinary tract infections. Scientific World Journal 2012: 349597.
-
Abu-Salem ME, El-Shazly HM, Hassan AZA (2016) Nocturnal enuresis among primary school children in Zarka district, Damietta governorate, Egypt. Menoufia Medical Journal 29(4): 1025-1032.
-
Hashem M, Morteza A, Mohammad K, Ahmad-Ali N (2013) Prevalence of nocturnal enuresis in school aged children: The role of personal and parents related socio- economic and educational factors. Iran J Pediatr 23(1): 59-64.
-
Hussein KA, Palpitany SA, Ahmed SH (2015) Prevalence of Urinary Tract Infection among Secondary School Students in Urban and Rural in Erbil: Comparative Study. Kufa Journal for Nursing Sciences 4 (3): 2223-4055.
-
Leung AKC, Wong AHC, Leung AAM, Hon K (2019) Urinary Tract Infection in Children. Recent Pat Inflamm Allergy Drug Discov 13(1): 2-18.
-
Al-Rikabi AAH, Abu-Raghif LF (2016) Screening Program for Urinary Tract Infection of Prepubertal Children at Al Nasiriya City Primary Schools. Iraqi National Journal of Nursing Specialties 29(1): 35-44.
-
White B (2011) Diagnosis and Treatment of Urinary Tract Infections in Children. Am Fam Physician 83(4): 409-415.
-
Barakat AJ (2012) Presentation of the child with renal disease and guidelines for referral to the pediatric nephrologist. Int J Pediatr 2012: 978673.
-
Sivaraj P, Pradhan S, Beriha SS, Barik RR, Tago N, et al. (2015) Study of risk factors associated with febrile urinary tract infection in children. Sri Lanka Journal of Child Health 44(3): 143-146.
-
Miller JM, Garcia CE, Hortsch SB, Guo Y, Schimpf MO (2016) Does Instruction to Eliminate Coffee, Tea, Alcohol, Carbonated, and Artificially Sweetened Beverages Improve Lower Urinary Tract Symptoms? A Prospective Trial. Journal of wound, ostomy, and continence, Nurses Society 43(1): 69-79.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?