Lyme Borreliosis Associated with Ramsay-Hunt Syndrome: A Case Presentation of Bilateral Facial Nerve Palsy in a 14-Year-Old Patient
Background: In children, facial neuropathy is the most common disease that occurs due to the damage of the cranial nerves. Facial nerve palsy (FNP) in children can be congenital or acquired. Congenital FNP may occur at birth due to the trauma and with certain genetic syndromes. Acquired FNP can be caused by HSV types 1,2, HHV-6, cytomegalovirus, EBV, VZV, bacterium B. burgdorferi or can result from inflammatory diseases, trauma and tumors. Unilateral or bilateral FNP is the most common complication of Lyme disease in children. The study that was conducted by Furuta Y. et al. indicates that reactivation of VZV infection is an important cause of acute peripheral FNP in children aged 6-15 years. Case Report: We have described a rare clinical case of bilateral peripheral FNP in a 14-year-old child with a confirmed diagnosis of Lyme disease and reactivation of VZV infection. Conclusions: Prescribed therapy with doxycycline for 21 days and valaciclovir for 7 days made it possible to achieve functional recovery of nerve on both sides.
Introduction
Lyme disease is a multisystem infectious disease caused by spirochetes that are part of the Borrelia burgdorferi sensu lato complex. The course of the disease is characterized by 3 stages: early localized, early disseminated and late disseminated. Peripheral facial nerve palsy is the most common manifestation of neurological involvement in the early localized stage of Lyme borreliosis (LB) [1]. In children with neuroborreliosis (NB), in addition to facial nerve palsy, paralysis of other cranial nerves and subacute meningitis may occur. Young children diagnosed with NB may have such nonspecific symptoms as loss of appetite, fatigue, mood swings [2]. Residual symptoms in Lyme-associated neuropathy are not typical, but such patients require specific antibiotic therapy to prevent further complications of Lyme borreliosis. Also, the presence of erythema migrans is not characteristic of patients with facial nerve palsy [3]. Ramsay-Hunt syndrome (RHS) is a reactivation of varicella zoster virus in the geniculate ganglion of the facial nerve in people who have previously had chickenpox. This syndrome is characterized by facial nerve palsy, herpes zoster oticus on the ipsilateral side and cochleovestibular symptoms. Herpetic rash can also be in the mouth (on the tongue, the palate) and on the lips [4].
RHS usually begins with the prodromal period which is characterized by pain, fever, fatigue for 1-3 days. Then herpes rash is formed in the external auditory canal, auricle, eardrum or in the oral cavity (inner surface of the lips, 2/3 of the anterior surface of the tongue, palate). Often RHS is accompanied by symptoms of the 8th cranial nerve involvement (dizziness, tinnitus, nausea, vomiting, nystagmus, hearing loss). The development of facial palsy occurs 1-2 weeks after the onset of herpes rash [4]. Detection of VZV infection by PCR of vesicle content is a better diagnostic method for the confirmation of Ramsay-Hunt syndrome than PCR of nasopharyngeal mucus, saliva, blood, urine, bronchial lavage and cerebrospinal fluid, because the latter shows a larger number of false-negative results [5]. It is recommended to start treatment as soon as possible, in the early phase of the disease, with glucocorticosteroids and antiviral drugs. Antiviral drugs prevent VZV replication and facial nerve involvement, steroids prevent inflammation and edema. Early administration of treatment is essential for functional recovery of facial nerve [6].
Case Report
In early July, a 14-year-old girl was bitten by a tick in her left eyelid, between her eyelashes. The girl’s mother removed the tick by herself, the spot of the bite was slightly red and healed quickly. From the medical history it is known that 3 years ago (2017) the child had chickenpox. She was treated as an outpatient, antiviral therapy was not prescribed. Ten days after the tick bite, the girl started having headaches, pain in the upper and lower jaws, episodes of vertigo and tinnitus. Due to severe headaches, the girl was consulted by maxillofacial surgeon and a neurosurgeon. They denied any pathology in their area. The girl was consulted by an orthopedist, who suspected a problem with the temporomandibular joint, and together with an orthodontist, prescribed orthodontic caps to treat the child’s pain. On July 20th, a herpetic rash developed on the girl’s lower lip(inside and outside of the lip). She was examined by an otorhinolaryngologist and no pathological changes were detected during examination.
From late July to mid-August, the child was wearing orthodontic caps, but the pain did not subside. Then there appeared pain behind the right ear which radiated to the right side of the neck and right shoulder. Also, our patient had a headache which was accompanied by nausea, muscle and bone pain, general weakness, drowsiness. On August 20, the girl’s mother noticed changes in the right side of the child’s face and consulted with a neurologist. The girl was diagnosed with right facial nerve palsy, which was characterized by incomplete eye closure, immobile eyebrow, flat nasolabial fold, drooping of the mouth ipsilateral to the lesion, immobile right side of the face. The patient was prescribed treatment (dexamethasone, diclofenac, vitamins B1, B6, B12) for 7 days with no positive dynamics. On August 27th, the child was admitted to the neurological department of the Children’s clinical hospital with a diagnosis of right facial nerve palsy. The results of electroneuromyography (27.08.20) revealed a decrease in the speed of conduction on the right facial nerve and it was 76% of normal speed on the 2nd branch and 60% of normal speed on the 3rd branch. M-responses were significantly reduced in amplitude from the 3rd branch.
Figures: Flat nasolabial on the left.
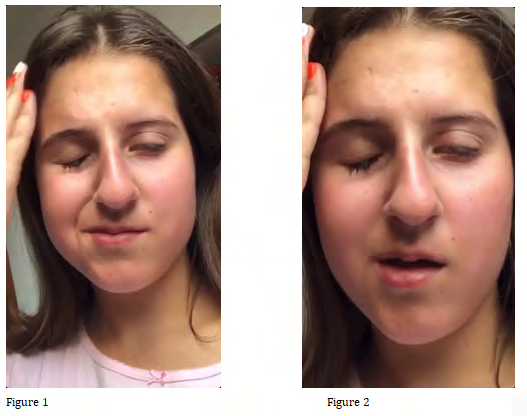
After two weeks of intensive treatment (dexamethasone, NSAID, B vitamins, magnetic therapy, phonophoresis, carbamazepine), all the symptoms of facial nerve damage disappeared and the child was discharged. Two days later, the child woke up in the morning with facial droop on the left side of the face involving the left side of the mouth and left eye. 14.09.20 the girl was hospitalized again with a diagnosis of left facial nerve palsy. The child was bothered by pain behind the left ear, headache, the left side of the face was completely motionless, there was incomplete eye closure, immobile eyebrow, flat nasolabial fold on the left (Figures 1 & 2). There was no hearing loss.
16.09.20 herpes rash appeared on the upper lip on the left and under the nose. The doctor suspected Ramsay-Hunt syndrome and prescribed acyclovir 600mg TID p.o. for 3 weeks. Otorhinolaryngologist’s examination reveled no herpetic rash in the area of the auditory canal and no changes in the eardrum. Having examined the girl ophthalmologist prescribed lubricating drops called artificial tears. The results of electroneuromyography (07.10.20) revealed a decrease in the speed of conduction on the left facial nerve and it was 75% of normal speed on the 2nd branch and 42% of normal speed on the 3rd branch 42%. M-responses were sharply reduced in amplitude. One should expect long and incomplete restoration of function of the affected nerve (especially 3rd branch). After treatment (acyclovir, NSAID, B vitamins, magnetic therapy, phonophoresis) the child was discharged from the hospital. At discharge, the child could close her eyelids but the droop of the corner of the mouth and flat nasolabial fold on the left were still present. In early October, the girl’s mother sought additional advice from an infectious disease doctor at the Pediatric infectious diseases department who, taking into account the history of a tick bite and frequent herpetic rash, prescribed analysis for IgM and IgG antibodies to B. burgdorferi, PCR to herpes simplex type 1 and 2, and taking into account the pain before and during facial nerve palsy she also prescribed IgM and IgG antibodies and PCR to Varicella zoster virus (Tables 1 & 2).
The Lyme Immunofluorescent assay (ELISA) - antibodies to B.burgdorferi was positive:
| IgM | ||
|---|---|---|
| 36.88 IU / ml | positive> 22 | |
| IgG | ||
| 163.05 IU / ml | positive> 22 | |
Table 2: IgM, IgG to B.burgdorferi (IFA, ELISA).
IgM and IgG immunoblot (euroimmun) results:
| IgM immunoblot | |
|---|---|
| p 41 | Positive |
| OspC Bb | Equivocal |
| OspC Ba | Equivocal |
| Ospc Bg | Equivocal |
| IgM | Equivocal |
| IgG immunoblot | |
| VlsE (Borrelia afzelii) | Positive |
| VlsE (Borrelia burgdorferi) | Positive |
| VlsE (Borrelia garinii) | Equivocal |
| p83 | Positive |
| p 41 | Positive |
| p 39 | Positive |
| IgG | Positive |
Table 1: IgM, IgG immunoblot to B.burgdorferi.
PCR to herpes viruses type 1, 2 - negative. Antibodies to VZV IgM - 2,365 (positive> 1,0), IgG - 6,239 (positive> 1,0). PCR to VZV-negative. Complete blood count: RBC - 4.83 x 1012 / l, HGB- 13.1 g / dl, Plt- 325 x109 / l, WBC- 9.63 x109 / l,neutrophils- 44%, lymphocytes- 40%, monocytes - 6%, eosinophils - 1%, basophils - 0%, ESR - 7 mm / h. According to the examination results, the girl was prescribed doxycycline 100 mg BID p.o. for 21 days and Valacyclovir 1000 mg TID p.o. for 7 days.
Discussion
Differential diagnosis of facial nerve palsy can be a challenge not only for a young specialist, but also for an experienced doctor. There are many reasons for the development of this pathology, including infectious and non-infectious ones [7]. The clinical case presented to your attention is interesting because the patient developed two types of infections (viral and bacterial) and each of them can lead to the development of facial nerve palsy. Bilateral facial nerve palsy is quite rare in pediatric practice, but Lyme disease is one of its most common causes. Therefore, when symptoms of unilateral or bilateral FNP are detected, it is necessary to exclude Lyme borreliosis as the main cause [8]. Examinations assigned by us confirmed the presence of Lyme borreliosis infection, but due to the clinical signs of Ramsay-Hunt syndrome, the prodromal period with a rise in body temperature to 38.6 degrees, herpetic rash on the mucous membrane of the mouth, headache and pain in the ear first on the right and then on the left, symptoms of vestibulocochlear nerve involvement - dizziness, tinnitus, nausea, prompted us to conduct additional researches, namely IgM i IgG antibodies to VZV and PCR to VZV. In our case, the patient had positive IgM and IgG antibodies to VZV, which indicated reactivation of the previous infection. PCR to VZV was negative. But according to the literature and our observations, the results of PCR to determine VZV in the blood can often be false-negative [9].
Conclusion
In our opinion, Lyme borreliosis could be a trigger for reactivation of VZV infection and the development of Ramsay-Hunt syndrome. Initially, our patient developed paralysis of the right side of the face, which was preceded by a typical prodromal period, herpetic rash, headaches and pain in the right ear, dizziness, tinnitus, nausea and radiating pain to the neck and shoulder. But due to the late diagnosis and late start of the treatment, which was incomplete, because the child received corticosteroids without antiviral drugs, after the recovery of the right facial nerve, our patient developed paralysis of the left side with pain in the left ear and herpetic rashes on the left lip, headaches. According to the final diagnosis the girl received doxycycline antibiotic therapy due to the Lyme borreliosis and valaciclovir therapy to prevent relapse of VZV infection. Prescribed therapy made it possible to achieve functional recovery of nerve on both sides.
Authors Contributions Statement
HL participated in the care of the patient and approved the final version, NB (corresponding author) participated in the care of the patient, wrote the first draft and approved the final version, KSK contributed to the data collection and ID approved the final version. All authors read and approved the final version of the manuscript.
Consent: Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Acknowledgments
We are thankful to the patient’s parents for permission to publish the child’s photos. We thank neurologists of Children’s Clinical Hospital for their cooperation in this clinical case.
References
-
Tveitnes D, Øymar K, Natås O (2007) Acute facial nerve palsy in children: how often is it lyme borreliosis?. Scand J Infect Dis 39(5): 425-431.
-
Skogman BH, Croner S, Nordwall M, Eknefelt M, Ernerudh J, et al. (2008) Lyme Neuroborreliosis in Children. Pediatr Infect Dis J 27(12) 1089-1094.
-
Gilchrist JM (2009) Seventh cranial neuropathy. Semin Neurol 29(1): 5-13.
-
Aydoğdu I, Atac E, Salturk Z, Atar Y, Özdemir E, et al. (2015) Pediatric Ramsay Hunt Syndrome: Analysis of Three Cases. Case Rep Otolaryngol 2015: 971249.
-
Laboratory Confirmation of Suspected Varicella.
-
Derin S, Derin H, Sahan M, Caksen H (2014) A pediatric case of ramsay hunt syndrome. Case Rep Otolaryngol 2014: 469565.
-
Ciorba A, Corazzi V, Conz V, Bianchini C, Aimoni C (2015) Facial nerve paralysis in children. World J Clin Cases 3(12): 973-979.
-
Wong K, Sequeira S, Bechtel K (2020) Pediatric Bilateral Facial Paralysis: An Unusual Presentation of Lyme Disease. Pediatr Emerg Care 36(11): e651-e653.
-
Furuta Y, Ohtani F, Aizawa H, Fukuda S, Kawabata H, et al. (2005) Varicella-zoster virus reactivation is an important cause of acute peripheral facial paralysis in children. Pediatr Infect Dis J 24(2): 97-101.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?