An Aberrant Position of Peripherally Inserted Central Venous Catheter in Extreme Preterm Infant
The use of a Percutaneously inserted central catheter (PICC) has increased with improved survival of extremely premature infants. Catheter malposition and perforation are associated with serious complications. PICC line position always needs to be confirmed after insertion. An Anteroposterior (AP) view radiograph is commonly used to confirm catheter tip position. We report a case of an unusual PICC position despite confirmation of the PICC tip position on the AP view radiograph. It is a potentially fatal complication and timely intervention can be lifesaving. Performing lateral X-rays to confirm the PICC tip or USG-guided placement of the catheter tip can prevent untoward serious complications. In the case of ascites, upper-extremity catheter insertion should be preferred instead of lower-extremity central venous catheters.
Background
With improved Survival of extremely premature infants, the use of central venous access has increased. Central lines are known as “Lifeline.” Securing central venous catheters (CVC) is important for ease of fluid and drug delivery. CVCs are also used to infuse dextrose solution with a high glucose infusion rate and vasoactive infusions. CVCs can be used for longer duration and thereby avoiding repeated venous cannulation in tiny infants. In neonates, PICC lines are commonly used and are inserted at basilic, cephalic, and axillary veins in the upper extremity; the great saphenous and popliteal veins in the lower extremity. The advantages of PICC lines are low insertion cost, decreased risk of infection, elimination of risk of postinsertion pneumothorax, and smooth removal. Approximately, 8-33% of neonates admitted to an intensive care unit require PICC insertion [1]. Position of CVCs is usually confirmed by AP view X-ray. PICCs are generally inserted safely, but complications may arise relating to device insertion, functionality, or post-procedure infection. These catheters are known to cause complications including arrhythmias, intracardiac thrombosis, systemic/ pulmonary embolization, endocarditis, pulmonary infarction, hemorrhage, and catheter-related infections [2, 3, 4]. Infrequent complications like myocardial perforation, cardiac tamponade, hydrothorax, chylothorax, phrenic nerve injury, and pericardial and pleural effusion have been reported as a complication of PICC [5, 6]. We are reporting an extremely preterm neonate with ascites who had PICC line extravasation leading to superficial abdominal wall/chest wall fluid collection.
Case
We report a case of a female infant (birth weight-525gm and GA-23 weeks) with an aberrant position of PICC. An umbilical venous catheter (Vygon-4Fr) was inserted at admission for the administration of parenteral nutrition. On day 3, the infant had TPN extravasations through the umbilical venous catheter as evidenced by ascites and abdominal distension; the umbilical venous catheter was removed on day 3. On the same day, PICC (Vygon- 28G) was inserted via the right lower extremity via a saphenous vein. The position of PICC was confirmed on an anteroposterior view; the tip of PICC was seen at the upper border of the T12 vertebra (Figure 1A). The infant developed chest wall edema insidiously over the next 36 hours. Ultrasonography chest performed showed an extension of PICC from a long saphenous vein through the superficial subcutaneous plane and cranially into a superficial epigastric vein (Figure 1C). A fluid pocket with echogenic areas in a subcutaneous plane was visualized in the abdominal and chest wall. The PICC line was withdrawn under sonography guidance to have a tip of the catheter in the external iliac vein. The infant’s chest wall edema reduced gradually over the next 24-36 hours. This PICC line was then used for 12 days period and was removed electively when the administration of parenteral nutrition was no longer required. This complication was attributed to an aberrant course of PICC into the collaterals, ultimately leading to perforation and tip lodgement in the superficial anterior abdominal.
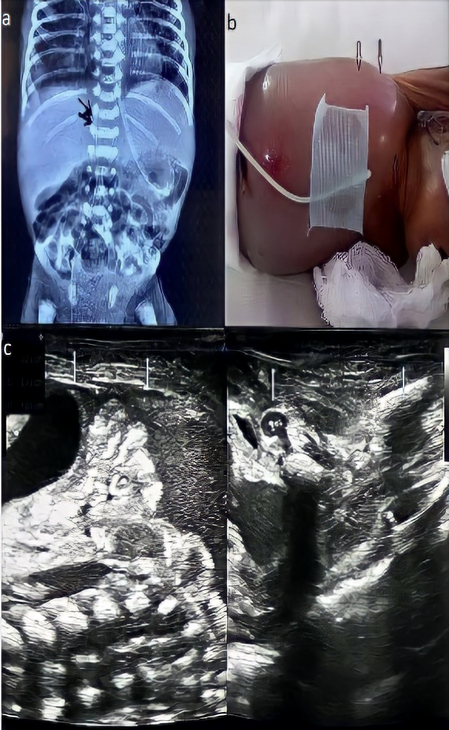
Figure 1a: Anteroposterior radiograph view showing tip of PICC at upper border of T12 vertebra, Figure 1b- Clinical photograph of the infant showing chest wall edema and ascites, Figure 1c- Ultrasonography images showing PICC traversing in subcutaneous plane (3.73cm).
Discussion
The ideal recommended position of the lower extremity PICC line catheter is T9-T10 outside of the cardiac silhouette and the upper extremity PICC line is in the distal portion of the SVC or at the SVC and right atrial junction. Centrally placed catheter tips are associated with fewer complications than non-centrally placed catheter tips [7]. Traditionally, central venous lines were placed using superficial anatomical landmarks. In this case, the position of the PICC was thought to be in an inferior vena cava based on AP view X-ray (Figure 1A); but the tip had an aberrant course and went into one of the superficial veins of the abdomen causing extravasation. In our case, the infant had ascites at the time of insertion of the PICC line which led to a superficial extension of PICC.
Extravasation of PICC could be diagnosed after 36 hours of PICC insertion. Neonate could not be diagnosed earlier because there was existing ascites and edema due to prior umbilical venous catheter extravasation. Initial X ray (Figure 1a) also showed central position of PICC line and therefore there was low suspicion of any extravasation of PICC line. Furthermore, it was in subcutaneous plane and was not associated with any clinical worsening or hemodynamic compromise. There is case report where extravasation was diagnosed late when vital organs were not involved (e.g. Heart, lung) [8]. The insertion site is usually selected as per the inserter’s preference and visualization/accessibility of veins. Upper extremity should be preferred for PICC insertion in case of ascites instead of the lower extremity considering anatomical distortion. We repositioned PICC under USG
guidance; however, pulling of PICC should be performed cautiously as it has been reported to be associated with endothelium damage, and aneurysms or rupture.
The use of PICC has become ubiquitous in neonatal intensive care units; efforts to confirm the tip position should be made before using the PICC. An ideal method for PICC line placement is Fluoroscopic placement; however, it is costly and requires an interventional radiology team. Ultrasound- guided PICC insertion is proven efficient in prospective, randomized studies comparing anatomical landmarks versus ultrasound-guided cannulation. Lower complication rates were significantly reported in these studies by ultrasound- assisted PICC insertion [9, 10]. An anteroposterior X-ray chest is routinely performed to determine the position of the PICC after catheterization. Factors such as inter-operator variations, congenital anatomical variations and insertion techniques predispose catheter malposition. Vein branches, tortuosity, force applied during insertion and guide wire are other possible factors. Resistance or need of excessive force during catheter insertion should raise suspicion of a problem, and further imaging should be performed. Clinician should make intensive analysis through much of anatomical acknowledgment to locate catheter tip. Few studies have suggested the concomitant use of lateral view abdominal radiographs to confirm the position of the PICC line in a 3-dimensional plane, however it has been rarely used [11]. In case of dubious line position, imaging (USG/contrast computer tomography) is should be performed immediately to prevent further sequalae. Ultrasonography is preferred over computer tomography because of feasibility, easy access and does not expose patients to ionising radiation [12, 13].
Complications related to PICC though rare, can be fatal; therefore, these neonates should be monitored vigilantly for PICC related complications. Confirmation of catheter tip position and frequent monitoring by experienced personnel will help reducing complications. Immediate intervention is extremely useful to avoid fatal complications. Though bedside X ray chest is routinely used to locate PICC tip, low threshold should be kept to do imaging in case of suspicion of PICC extravasation. Non-invasive investigations such as ultrasonography may provide a rapid yet safe means to assess PICC. Authors suggest that in case of ascites which led to congenital anatomical variation upper extremity central cannulation should be preferred. Education, standard insertion techniques and high level of awareness about likely UVCs related complications of may assist in decreasing the complications.
Funding: No funding was received.
Conflict of Interest: The authors declare no conflict of interest.
References
-
Chien LY, Macnab Y, Aziz K, Andrews W, McMillan DD, et al. (2002) Variations in central venous catheter related infection risks among Canadian neonatal intensive care units. Pediatr Infect Dis J 21(6): 505-511.
-
Mehta S, Connors AF, Danish EH, Grisoni E (1992) Incidence of thrombosis during central venous catheterization of newborns: a prospective study. J Pediatr Surg 27(1): 18-22.
-
Abdellatif M, Ahmed A, Alsenaidi K (2012) Cardiac tamponade due to umbilical venous catheter in the new born. BMJ Case Rep 2012: 2012-6160.
-
Hou A, Fu J (2020) Pericardial Effusion/Cardiac Tamponade Induced by Peripherally Inserted Central Catheters in Very Low Birth Weight Infants: A Case Report and Literature Review. Front Pediatr 8: 235.
-
Garden AL, Laussen PC (2004) An unending supply of “unusual” complications from central venous catheters. Paediatr Anaesth 14(11): 905-909.
-
Tosello B, Michel F, Merrot T, Chaumoitre K, Hassid S, et al. (2011) Hemidiaphragmatic paralysis in preterm neonates: a rare complication of peripherally inserted central catheter extravasation. J Pediatr Surg 46(7): E17- 21.
-
Racadio JM, Doellman DA, Johnson ND, Bean JA, Jacobs BR (2001) Pediatric peripherally inserted central catheters: complication rates related to catheter tip location. Pediatrics 107(2): E28.
-
Garg M, Rajan N, Dhua A, Krishnan L (2016) Malpositioned Central Line in A Neonate Presenting as Superficial Abdominal Abscess. J Neonatal Surg 6(1): 24.
-
Mussa FF, Towfigh S, Rowe VL, Major K, Hood DB, et al. (2006) Current trends in the management of iatrogenic cervical carotid artery injuries. Vasc Endovascular Surg 40(5): 354-361.
-
Leung J, Duffy M, Finckh A (2006) Real-time ultrasonographically-guided internal jugular vein catheterization in the emergency department increases success rates and reduces complications: a randomized, prospective study. Ann Emerg Med 48(5): 540-547.
-
Sneath N (2010) Are Supine Chest and Abdominal Radiographs the Best Way to Confirm PICC Placement in Neonates? Neonatal Netw 29(1): 23-35.
-
Wang L, Liu ZS, Wang CA (2016) Malposition of Central Venous Catheter: Presentation and Management. Chin Med J (Engl) 129(2): 227-234.
-
Randen AV, Lameris W, Es HW, Heesewijk HPM, Ramshorst B, et al. (2011) A comparison of the Accuracy of Ultrasound and Computed Tomography in common diagnoses causing acute abdominal pain. Eur Radiol 21(7): 1535-1545.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?