Williams Syndrome A Rare Case Report
We report a rare case of Williams Syndrome diagnosed at an age of two months based on subtle facial dysmorphism elfin facies and a pulmonary systolic murmur at birth. Echocardiogram revealed mild supravalvular aortic stenosis and mild supravalvular pulmonary stenosis extending into branch pulmonary arteries. Mild developmental delay, hypotonia, feeding problems, constipation and failure to thrive were present. In view of distinctive facial phenotype in combination with cardiac abnormalities, Williams Syndrome was strongly suspected. It was confirmed by fluorescence in situ hybridisation test demonstrating a deletion of elastin gene on chromosome 7. This case highlights the importance of pediatricians awareness about malformation syndromes which can help in early diagnosis, timely genetic counselling to the family and better patient outcomes.
Introduction
Williams syndrome (WS) is a rare congenital neurodevelopmental disorder occurring in 1 per 25,000 live births [1] characterized by facial dysmorphism, cardiovascular, renal and skeletal anomalies, endocrine, cognitive and intellectual disorders. Phenotype is char¬acterized by short stature and craniofacial abnormalities. It is associated with a microdeletion in chromosome region 7q11.23, encompassing the elastin gene [2]. Most frequent cardiovascular anomalies are supravalvular aortic stenosis (SVAS) and/ or supravalvular pulmonary stenosis [3]. Combination of a typical clinical phenotype and echocardiographic profile aid in the diagnosis. However, the definitive diagnosis is made by demonstration of elastin gene hemizygosity assessed by fluorescent in situ hybridization (FISH) test.
Clinical Description
A female neonate was born to a 32 year old second gravida (non-consanguineous marriage, dichorionic twin pregnancy) at 34+5 weeks of gestation by caesarean section in view of premature labour and cord prolapse. Apgar score was normal and birth weight was 1900 grams. Neonate required non-invasive ventilation due to moderate respiratory distress at birth. On general examination, subtle facial dimorphism in form of broad forehead, flat nasal bridge, long philtrum and wide mouth were noted Figure 1.

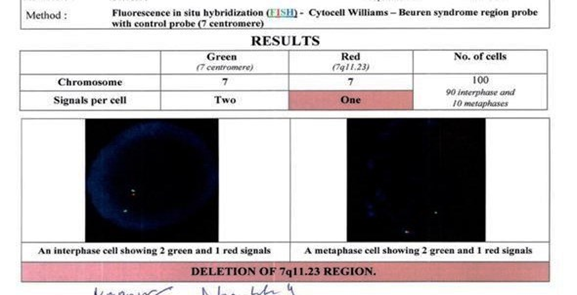
A pulmonary ejection systolic murmur (grade 3/6) was heard on second day of life. Echocardiogram detected mild SVAS, supra-pulmonary stenosis with significant branch pulmonary artery stenosis, patent foramen ovale and normal biventricular contractility. Abdominal, renal and cranial ultrasound findings were normal. Primary metabolic screening and serum calcium were also normal. Hearing and eye screening were found to be normal. Baby was discharged by twelfth day of life on breast feeds, formula feeds and supplements. As there were no signs of cardiac hypertrophy or heart failure, no active cardiac intervention was advised. WS was strongly suspected due to a combination of subtle facial phenotype with cardiac abnormalities. Diagnosis was confirmed by FISH test which demonstrated a deletion of elastin gene on chromosome 7q11.23 Figure 2.

Genetic analyses (FISH test) of the parents were normal. Baby developed constipation and feeding difficulty leading to failure to thrive. Mild developmental delay and hypotonia were present. Early intervention programs were initiated as advised by pediatric neurologist in form of oromotor, occupational and speech therapies. At one year of age, echocardiogram showed no significant supra-valvular aortic stenosis and mild right pulmonary artery stenosis. In view of spontaneously resolving cardiac lesions, further follow up was advised after three years. Upon regular follow ups and serial evaluation, a steady improvement in feeding, growth and developmental milestones, speech and school performance were noticed Figure 3.
Discussion
WS is a rare familial multisystem disorder characterized by distinct facial appearance, cardiovascular anomalies, hypercalcemia and a characteristic neurodevelopmental and behavioural profile. It affects males and females equally [1]. It is considered a segmental aneusomy due to a hemizygous deletion in 7q11.23 region containing 26 to 28 genes and 2 mi RNA loci. A clear genotype-phenotype correlation has been established in WS for elastin gene which is responsible for vascular and connective tissues disorders. The confirmation of diagnosis is carried out by FISH test [2]. In our patient, FISH test demonstrated a deletion of elastin gene on chromosome 7. A characteristic “elfin face” consists of a prominent metopic suture, small chin, sunken nasal bridge, eye puffiness, wide mouth and prominent lower lip. Facial dysmorphism can be subtle early in life and may lead to difficulty in diagnosis. Subtle facial dysmorphism was identified at birth in our patient. During neonatal and infancy period, cardiovascular manifestations are most common in WS and help in making an early diagnosis when other features can remain unrecognized. A detailed cardiovascular screening including four limb blood pressure and echocardiogram must be performed [4]. Most patients with supravalvular aortic stenosis are diagnosed during evaluation of an asymptomatic heart murmur as was the case in our patient [5]. Systolic murmur is similar to valvular aortic stenosis, most prominent at upper right sternal border with radiation into the suprasternal notch and neck. Branch PA stenosis murmurs are extensively conducted on both the left and the right sides of the thorax depending on the severity of stenosis. In our patient, since the stenosis of branch PAs was mild, the murmurs were quite localized and were superimposed on the murmur of SVAS.
Besides diagnosis, severity of cardiovascular involvement also helps in prognostication. SVAS is the most common cardiac anomaly (64%) of which (30%) requires surgical correction’s before 5 years of age and the same can be done with low morbidity and mortality [5]. Other cardiac lesions include mitral valve prolapse (15%), pulmonary artery stenosis (13%), coarctation of aorta (8%), aortic hypoplasia, ventricular or atrial septal defects [4]. If significant SVAS is left untreated, cardiac hypertrophy followed by cardiac failure is probable. Although balloon dilation and stenting have been performed but close proximity to aortic valve and coronary artery orifices are significant obstacles and operation is the treatment of choice currently [6]. Rate of restenosis after operation with current surgical techniques is very low. Branch pulmonary artery stenosis may occur as an isolated finding or in conjunction with other cardiac malformations. Trans catheter management with balloon pulmonary angioplasty (BPA) and/or endovascular stenting is considered the procedure of choice [7]. In our case, mild SVAS with bilateral branch pulmonary artery stenosis showed spontaneous resolution of SVAS and LPA stenosis with mild RPA stenosis. Hence the child was advised conservative treatment without any surgical intervention.
Infants are often small for gestational age and show intrauterine growth retardation antenatally. On the contrary, antenatal ultrasound findings and Doppler study were normal in this case. Vomiting, gastroesophageal reflux, constipation and excessive irritability are common in infancy. Constipation and feeding difficulty lead to failure to thrive as seen in the present case. Patients may develop hypertension because of renal artery stenosis and infantile hypercalcaemia leading to neph-rocalcinosis [8, 9]. Renal ultrasound with Doppler is routinely obtained to screen for renal artery stenosis. Regular monitoring of serum calcium at diagnosis, 2 years, 5 years and annually in adolescence is recommended. Hyperkalaemia is managed by low-calcium diet and no supplemental vitamin-D [9]. Serum calcium was within normal limits in our patient. WS accounts for 6% of all cases of mental retardation of genetic origin. Neurocognitive profile commonly includes mild mental retardation. Cognitive strengths and weaknesses relative to other patients with mental retardation include relatively good auditory rote memory but extreme difficulty with visuospatial construction tasks [10].
WS is diagnosed by primary clinical findings such as ‘elfin face’, congenital heart defects and neurocognitive defects. Diagnosis is usually made during late infancy when patients have distinctive facial appearance. However, WS was strongly suspected in early infancy in this case due to a combination of subtle facial dysmorphism and cardiac abnormalities, which was confirmed subsequently by genetic testing at two months of age. Annual evaluation of every child should include growth and developmental assessment, blood pressure monitoring, auditory and vision screening, cardiovascular evaluation (to look for progressive vascular stenosis which is generally seen in first 5 years of life) [11]. An early suspicion of WS, multidisciplinary team approach, serial evaluation and investigations, early intervention programs lead to a successful neonatal outcome in this case.
Conclusion
WS should be kept as a differential diagnosis in infants and children presenting with facial dysmorphism and cardiovascular abnormalities. Detailed cardiovascular screening and examination must be performed in presence of distinctive facial phenotype. Early cardiac as well as non- cardiac interventions yield a better patient outcome and good prognosis. Although our patient did not need cardiovascular interventions, a multidisciplinary team approach and implementation of early intervention programs lead to a successful outcome as was seen in our case.
References
-
Moris CB, Mervis CA (2000) Wiliams syndrome and related disorders. Annu Rev Genomics Hum Genet 1: 461-484.
-
Merla G, Pierri NB, Micale L, Carmela F (2010) Copy number variants at Williams Beuren Syndrome 7q11.23 region. Hum Genet 128(1): 3-26.
-
Eronen M, Peippo M, Hiippala A, Raatikka M, Arvio M, et al. (2002) Cardiovascular manifestations in 75 patients with Williams syndrome. J Med Genet 39(8): 554-558.
-
Collins RT, Kaplan P, Somes GW, Rome JJ (2010) Long-term outcomes of patients with cardiovascular abnormalities and Williams Syndrome. Am J Cardiol 105(6): 874-878.
-
Beuren AJ, Schulze C, Eberle P, Harmjanz D, Apitz J (1964) The syndrome of supravalvular aortic stenosis, peripheral pulmonary stenosis, mental retardation and similar facial appearance. Am J Cardiol 13(4): 471-483.
-
Roemers R, Kluin J, Arrigoni S, Regina B, Joost van M, et al. (2018) Surgical Correction of Supravalvar Aortic Stenosis: 52 Years Experience. World J Pediatr Congenit Heart Surg 9(2): 131-138.
-
Zablah JE, Morgan GJ (2019) Pulmonary artery stenting. Journal of Interventional Cardiology 8:33-46.
-
Sforzini C, Milani D, Fossali E, Barbato A, Grumieri G, et al. (2002) Renal tract ultrasonography and calcium homeostasis in Williams-Beuren syndrome. Pediatr Nephrol 17(11): 899-902.
-
Sindhar S, Lugo M, Levin MD, Danback JR, Brink BD, et al. (2016) Hypercalcemia in patients with Williams-Beuren Syndrome. J Pediatr 178: 254-260.
-
Mervis CB, Robinson BF, Bertrand J, Morris CA, Klein- Tasman BP, et al. (2000) The Williams syndrome cognitive profile. Brain Cogn 44(3): 604-628.
-
Committee on Genetics (2001) American Academy of Pediatrics: health care supervision for children with Williams syndrome. Pediatrics 107(5):1192-204.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?