Spontaneous Emphysema, Pneumomediastinum and Pneumopericardium Revealing Unrecognized Inhalation of a Foreign Body
Inhalation of a foreign body is a frequent problem in pediatrics with a very difficult diagnosis in the absence of penetration syndrome. It is a very rare cause of emphysema moreover the combination of emphysema, pneumomediastinum or pneumopericardium is an exceptional form. We report an unrecognized case of inhalation of a foreign body, a 5-year-old girl was admitted for respiratory distress with diffuse subcutaneous emphysema in the eyelids , face, neck and chest more marked on the left . A chest CT revealed emphysema with pneumomediastinum, pneumopericardium and a focus of LIG condensation. The diagnostic bronchoscopy was performed under general anesthesia. A sunflower seed, landlocked completely obstructing the bronchial lumen was detected and recovered in the left main bronchus. The removal of the foreign body resulted in improvement of the emphysema and the gradual disappearance of symptoms.
Summary
Introduction
Inhalation of tracheobronchial foreign bodies is a frequent situation in pediatric emergencies and represents the most feared location due to their morbidity and mortality, particularly in children under three years old. Penetration syndrome is the key to early diagnosis, however it can go unnoticed and therefore diagnosis can be delayed [1, 2]. Such delay increases the risk of complications; emphysema and subcutaneous pneumomediastinum are rare presentations of foreign body inhalation [3, 4]. We report a case of an unrecognized bronchial foreign body in a 5-year-old girl, revealed by emphysema, pneumediastinum and pneumopericardium.
Observation
A 5 year old girl was admitted to our ward with rapidly worsening facial puffiness. Having a history of influenza-like illness a month ago, fever with cough, the child was treated with macrolide and paracetamol. Ten days later, swelling of the neck appeared. Her attending physician had concluded that she had angioedema and the girl was referred to our hospital.

The vital parameters at reception were found in a conscious child with significant emphysema of the face and spongy swelling of the eyelids on inspection (Figure 1). Clinical examination revealed diffuse snowy crepitation on palpation of the face, eyelids, neck and chest more marked on the left. There was dyspnea and suprasternal indrawing, bilateral snoring rales on pulmonary auscultation with a respiratory rate of 34 cycles / minute, arterial oxygen saturation (SaO2) at 95% in ambient air and a fever in the air. 38.9C. Cardiovascular examination was normal with blood pressure (BP) at 11/06 and heart rate at 114 beats / minute. In addition, there was no ascites, edema of the lower limbs, or oliguria.
The chest x-ray confirmed the presence of air in the subcutaneous tissue with pneumomediastinum (Figure 2).

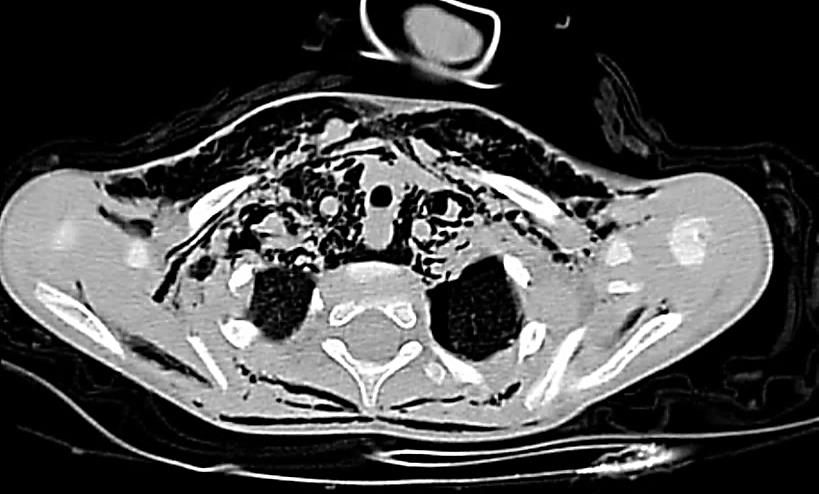
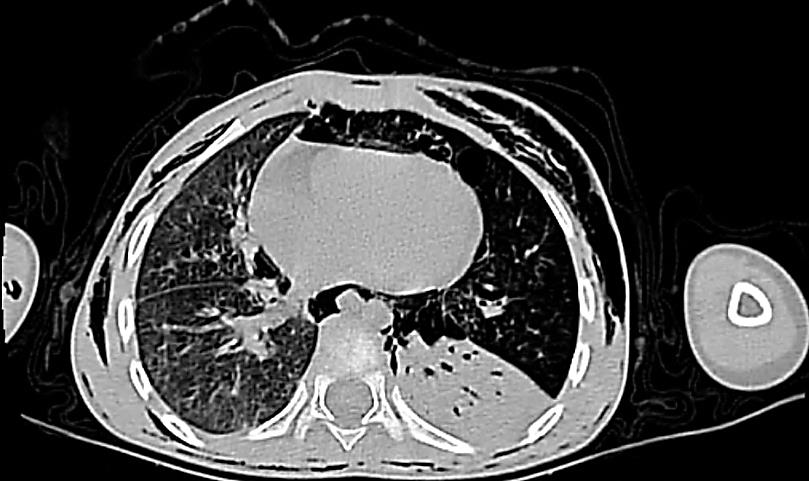
Computed tomography (CT) of the chest revealed the presence of massive subcutaneous emphysema infiltrating the soft tissues of the face and neck (Figure 3). There was also a diffuse and septate pneumomediastinum dissecting the proximal peribronchovascular spaces more marked on the left side with a pneumopericardium (Figure 4). Furthermore, there was no individualization of foreign body or breach in the tracheobronchial tree.
Bronchoscopy was performed under general anesthesia with non-invasive blood pressure monitoring, an electrocardiogram, and pulse oximetry. After pre- oxygenation with inspiratory fraction of oxygen (FIO 2) at 100% for 3 min, a standard induction was performed using propofol at a dose of 2.5 mg / kg, fentanyl at a dose of 1 mcg / kg and rocuronium at a dose of 0.6 mg / kg. Anesthetic maintenance was provided by sevoflurane with gentle manual ventilation between attempts to extract the foreign body.
Endoscopic exploration showed the presence of a foreign body (sunflower seed) safely recovered (Figure 5), completely obstructing the upper left bronchial lumen with a slightly obstructive granuloma opposite, followed by aspiration of purulent secretions in sheets from the left lower lobe without residual fragment. Endoscopic control was satisfactory.

At the end of the procedure, waking up consisted of a decurarization by sugammadex at a dose of 4 mg / kg with nasal and oral aspiration soft without bronchial stimulation. Subsequently, the patient was treated with antibiotic therapy and corticosteroid therapy, the subsequent course was favorable with progressive reduction of emphysema within 48 h without further intervention. On day 3, the chest X-ray revealed no abnormalities (Figure 3) and the child was declared out.
Discussion
Inhalation of the foreign body may go unnoticed and the child may present with asthma, bronchiectasis, recurrent pneumonia or hemoptysis without an underlying cause and is often misdiagnosed. Inhaling a body foreign should always be considered in children in the event of sudden onset of respiratory symptoms even in the absence of penetration syndrome.
Snowy crepitations on skin palpation are the key semiologic element in the diagnosis of subcutaneous emphysema. A spongy appearance of the skin can be noted in massive emphysema such as in the eyelids in our observation. The search for a pneumomediastinum is an essential step, the etiological investigation of which is the basis of the treatment. Pneumomediastinum is the presence of air in the interstices of the mediastinum, which originates primarily from the tracheobronchial tree [5].
The most common causes of pneumomediastinum are pulmonary infections, asthma and any cause of sudden increase in intra-bronchial pressure (closed chest trauma, recurrent vomiting), the possibility of inhaling a foreign body should be considered, especially in children.
Pneumomediastinum and subcutaneous emphysema due to inhalation of foreign body are rare in the pediatric population. A study in Taiwan showed that 81% of spontaneous pneumomediastinum were preceded by cough and 75% by dyspnea. The most common underlying medical causes were asthma (50%) and idiopathic origin (31%) [6].
The main triggering factors in another study, analyzing the etiologies of spontaneous pneumomediastinum in children, were infections (43.2%) and asthma (21%) and only one child had a foreign body inhalation. In a review, Gasser et al. reported that the most common comorbidity in children was asthma (22.2%), bronchospasm (49%), cough (45.6%), vomiting (10.3%) and inhalation foreign body (8.3%) [7].
This respiratory damage following inhalation of a foreign body may be related to the exertion of an expulsive cough, direct trauma to the foreign body, air entrapment or pulmonary emphysema. The clinical presentation varies depending on the intensity and chronicity of the air leak. Early diagnosis associated with aetiologic treatment and measures reducing intra-alveolar pressure lead to resorption of the pneumomediastinum. In other situations, the air gradually diffuses, and once it reaches the soft tissues, it can dissect the soft parts of the neck and pericardium [8]. Infiltration of these tissues exerts pressure on the vascular structures and upper respiratory tract, constituting all of the severity of subcutaneous emphysema and pneumomediastinum.
The anesthetic management of such a child is a challenge. Muscle relaxation is necessary for bronchoscopy, but intermittent positive pressure ventilation (IPPV) can worsen emphysema by facilitating the entry of air through the ruptured portion of the mucosa into the tissue, although in the literature no case has been published showing a worsening of the condition after IPPV in a patient with FAB. The IPPV, in the presence of pneumothorax, is not recommended before placing the chest tube. However in other patients, where the cause of emphysema is simply a disruption of the mucosa the authors believe that mild IPPV can be achieved with adequate tidal volume and slight gas leakage [9]. Without IPPV, oxygenation can be obtained by apneic diffusion of oxygen by ventilation using the rigid bronchoscope [10].
Conclusion
We conclude that cases of FAB that present respiratory distress and ECS without a history of aspiration may be misdiagnosed. The diagnosis of foreign body inhalation is a common problem in the absence of penetration syndrome. Bronchoscopy, a diagnostic and therapeutic procedure, is a challenge for anesthesiologists. IPPV can be used safely during bronchoscopy with caution in the absence of pneumothorax. Removal of the foreign body causes gradual absorption of air and disappearance of symptoms.
References
-
Oguzkaya F, Akcali Y, Kahraman C, Bilgin M, Sahin A (1998) Tracheobonchial foreign body aspirations in childhood: a 10-year experience. Eur J Cardiothorac Surg 14(4): 388-392.
-
Burton EM, Riggs Jr W, Kaufman RA, Houston CS (1989) Pneumomediastinum caused by foreign body aspiration in children. Pediatr Radiol 20(1-2): 45-47.
-
Midulla F, Guidi R, Barbato A, Capocaccia P, Forenza N, et al. (2005) Foreign body aspiration in children. Pediatr Int 47(6): 663-668.
-
Findlay CA, Morrissey S, Paton JY (2003) Subcutaneous Emphysema secondary to foreign body aspiration. Pediatr Pulmonol 36(1): 81-82.
-
Damore DT, Dayan PS (2001) Medical causes of pneumomediastinum in children. Clin Pediatr (Phila) 40(2): 87-91.
-
Chiu CY, Wong KS, Yao TC, Huang JL (2005) Asthmatic versus non-asthmatic spontaneous pneumomediastinum in children. Asian Pac J Allergy Immunol 23(1): 19-22.
-
Lee CY, Wu CC, Lin CY (2010) Etiologies of spontaneous pneumomediastinum in children in middle Taiwan. Pediatr Pulmonol 45(9): 869-873.
-
Cummings RG, Wesly RL, Adams DH, Lowe JE (1984) Pneumopericardium resulting in cardiac tamponade. Ann Thorac Surg 37(6): 511-518.
-
Wong DT, McGuire GP (2000) Subcutaneous emphysema following transcricothyroid membrane injection of local anesthetic. Can J Anaesth 47(2): 165-168.
-
Ramadan HH, Bu-Saba N, Baraka A, Mroueh S (1992) Management of an unusual presentation of foreign body aspiration. J Laryngol Otol 106(8): 751-752.
- Understanding Pediatric Multiple Sclerosis: Clinical Presentation, Diagnostic Criteria, Therapeutic Advances, and Supportive Care Approaches
- Hemophilia in Children
- Xia-Gibbs Syndrome- A Case Report
- A Study to Assess Effectiveness of Play Therapy in Reducing Post-Operative Pain among Children Age 2 To 5 Year who have Undergone General Surgeries in Selected Pediatric Hospitals of Vadodara
- Preterm Birth: Scope of the Problem, Cost of Care, Potential Complications and Current Guidelines for Management
- Noradrenaline: Can we Use it to Manage Hemodynamic Instability among Neonatal Septic Shock at the NICU?