Role of Cytokines in Behcets Disease
Behcets disease (BD) is considered a chronic relapsing multisystem inflammatory disorder. It has a worldwide distribution, but it is more prevalent in Mediterranean countries. Although its etiopathogenesis remains elusive, Immunological investigations have demonstrated the presence of immune dysregulation among the patients with BD. The disease is characterized by infiltration of lymphocytes and neutrophils into the affected organs.the Th1 type cytokine profile is predominant in. The serum concentrations of mainly Th1 type cytokines were reported to be increased in BD and probably contribute to neutrophil and endothelial cell activation.
Introduction
Behcet's disease is a chronic, relapsing, systemic vasculitis of unknown etiology with the clinical features of mucocutaneous lesions and ocular, vascular, articular, gastrointestinal, urogenital, pulmonary and neurologic involvement. The disease is particularly prevalent in ‘Silk Route’ populations but has a global distribution. Behcet's disease affects primarily young subjects [1]. Behcets disease (BD) is a chronic, inflammatory multisystemic condition of unknown etiology. It is clinically characterized by recurrent orogenital ulcerations, skin eruptions; ocular manifestations; arthritis; Vasculitis and in some cases neurological and large vessel involvement. An etiology has not been defined, but genetic, environmental, viral, bacterial and immunological factors have been proposed as causative agents. The treatment includes colchicines, thalidomide, steroids and immuno-suppressive agents and it is based on the severity of systemic manifestations, such as central nervous system involvement, arterial aneurysms and thrombosis of the major veins. Mortality is related to major system involvement. In this article the different clinical features [2]. Although its etiopathogenesis remains elusive, the most accepted hypothesis is that the excessive inflammatory response is triggered by an infectious agent in a genetically susceptible host. Immunological investigations have demonstrated the presence of immune dysregulation among the patients with BD. The disease is characterized by infiltration of lymphocytes and neutrophils into the affected organs. Because cytokines are involved in the regulation of functions of lymphocytes and phagocytes [3]. As for most other autoimmune disorders and vasculitides, the Th1 type cytokine profile is predominant in BD [4]. The serum concentrations of mainly Th1 type cytokines were reported to be increased in BD and probably contribute to neutrophil and endothelial cell activation [5]. The synthesis profiles of cytokines are considered to cause one of two types of responses: T-helper cell type 1
(Th1) responses, produces interleukin (IL)-2, IFN-γ, TNF and lymphotoxin and facilitates cell-mediated immune responses and elicit delayed hypersensitivity reactions; or Th2 responses, produces mainly IL-4, IL-5, IL-6 , IL-10 and IL-13 and assists in antibody production (humoral immunity), and suppress cell mediated immunity [6]. The Th1 ⁄ Th2 cell paradigm may be important in BD, because Th1 and Th2 cells imbalance may modulate some immune functions, sustain inflammatory reactions and aggravate the disease. The ratio of Th1 to Th2 cytokine- producing cells can reflect cytokine homoeostasis and indicate Th1 or Th2 predominance during disease activity. Many reports showed that there is Th1/ Th2 imbalance with strong polarization toward Th1 in BD [5].
Cytokine Classification Involved in BD
Sophisticated interlacing cytokine network is implicated in the onset, evolution and even organ damages of the disease. Cytokines involved can be categorized as Th1 type, Th2 type, chemokines and other proinflammatory cytokines, etc [7]. Stimulation of peripheral blood mononuclear cells from patients with BD with either phytohemagglutinin or anti CD3/anti-CD40 all showed a strong polarization to Th1 cytokine production [8]. In active BD, enhanced entry into the Th1 response effector pathway of CD4+ T cells was observed after stimulation with Concanavalin A (ConA) followed by PMA Ion. Analysis of CD4+ T cells at an identical cell division number in response to ConA followed by PMA Ion revealed that IFN-γ-producing cells were increased in active BD patients compared with normal subjects. These results suggest that the Th1 response of dividing CD4+ T cells is predominantly operating in active BD [9]. The in vitro maximal capacity of immune cells to produce different cytokines in response to mitogen stimulation has been shown to vary among individuals. Such differences can be attributed to several molecular mechanisms, including variations in transcription, translation and secretion pathways. An additional potential mechanism was described involving conservative mutations within cytokine-coding regions, and nucleotide variations within more pronounced regulatory regions [10]. Genetic polymorphisms in several cytokine genes have been described and demonstrated to influence gene transcription, leading to interindividual variations in cytokine production. Therefore, it is reasonable to speculate that genetic polymorphisms that regulate the production of certain cytokines may be important determinants of susceptibility to BD and some of its clinical and laboratory features [11].
Chemokines and Chemokines Receptors: IL-8 possesses the function of neutrophil chemotactic and angiogenesis. IL-8 was reportedly elevated in active stage of BD in a number of studies [12]. Showed that IL-8 level was higher in BD patients with vessel involvement than those with oral, genital ulceration or uveitis [13]. Genetic studies did not establish positive result, suggesting that there might be other cause(s) that lead to the enhanced secretion of IL8 [14]. Inflammatory Cytokines IL-1 gene family: is composed of IL-1α, IL-1β, and IL- 1Ra.IL-1α, IL-1β are pleiotropic cytokines with primarily proinflammatory effects, which induce acute phase responses, activate endothelial cells, and lead to expression of adhesion molecules and coagulation factors [15]. Ever since 1990, IL-1 has been found elevated in sera of patients with BD [16]. Demonstrated a significantly higher level of IL1β in synovial fluid of BD [17]. TNF-α: is a multifunctional, pro-inflammatory cytokine, which performs a variety of functions in innate immune response, including activation of macrophages and apoptosis, which appears to be responsible for the recurrent inflammatory reactions encountered in BD patients. TNF-α level tend to be significantly elevated in active BD patients, and increased production of TNF-α have been associated with clinical deterioration [18]. T lymphocytes expressing the γδ receptors in BD are activated in vivo and produce increased amounts of TNF- α compared with healthy controls [3]. Treatment with anti-TNF-α monoclonal antibodies has resulted in improvement of various manifestations of BD [19]. Th17 type Cytokines: IL-17 producing Th cells, referred as Th17 cells, were identified as a new subset of T helper cells unrelated to Th1 or Th2 cells, and several cytokines, e.g. IL-21 and IL-23, are involved in regulating their activation and differentiation [20]. IL-17: is a novel cytokine family with a proinflammatory nature, and consists of similar cytokine members IL-17A, IL-17B, IL-17C, IL-17D, IL-17E, and IL-17F [21]. IL-17 cytokine induced the production of diverse proinflammatory cytokines, chemokines with neutrophil- recruiting activity, cell adhesion molecules, and growth factors [22]. Demonstrated that the IL-17 serum level in active BD patients is enhanced to a higher degree than in that of BD patients in remission [5]. IL-23: shares a p40 subunit with IL-12, it has additional inflammatory effects apart of IL-12. A previous study has shown higher IL-23 in sera of BD patients with uveitis and found that there was a meaningful correlation between IL-23 content and disease activity [23]. An increased expression of IL-23 p19 mRNA in erythema nodosum-like lesions of BD patients. IL23 is an indispensible cytokine for the differentiation of Th17 [7, 24]. These results suggest that the IL-23/IL-17 pathway may make a contribution for immunological aberrations of BD [25]. Th1 Cytokines IFN-γ: possess antiviral, antitumor and immunomodulatory properties. IFN-γ has a critical role in modulating the IL-4, IL-10 and IL-12 cytokine network pathway. It is also considered as a proinflammatory cytokine because of its effects on TNF activity .IFN-γ level is elevated in BD patients suffering from uveitis [26]. IL-12: mainly produced by APC, such as macrophages and monocytes, and plays a crucial role in the obligatory transformation of naive T cells into Th1 cells [26]. According to the study of IL12 level are elevated in BD patients with uveitis [27]. IL-18: Activates NK cell and stimulates the secretion of IFN-γ from it. IL-18 promotes the differentiation of Th0 to Th1 instead of Th2 [7]. Identified that the IL-18 level in sera of patients with BD elevated substantially [18]. IL-18 is associated with disease activity of BD, level of IL-18 in remission stage of patients is also higher than that in normal population, catching the potential role of IL-18 in both the initiation step and sustained inflammatory activation status of the disease [28].
Th2 Cytokines IL-6: IL-6 (26 kDa) is a multifunctional pro-inflammatory cytokine with an important role in the regulation of immune response [29]. It is produced by monocytes, epithelial cells and fibroblasts, and causes polyclonal B- cell activation, hypergammaglobulinaemia, and autoantibody production with T-cell activation [30]. The major effect of IL-6 described is the proliferation and differentiation of cells, as well as increasing secretion of acute-phase proteins by the liver [31]. Abnormal IL-6 production has been implicated in some autoimmune diseases and chronic inflammatory reactions [32]. BD has been labeled as a Th1 driven disease. Conversely IL-6, which promotes Th2 cell differentiation, inhibits IFN-γ production and inhibits Th1 cell differentiation was shown in many studies to be elevated in serum of BD compared to control [33]. Increased IL-6 plasma levels and enhanced IL-6 mRNA expression have been found in patients with BD especially those in active state [9]. IL-10: Th2 type cytokine, plays a role in the inhibition of cytokines derived from Th1 cell which turn out to down- regulate the function of Th1 immune responses, inhibiting antigen-presenting capacity of Macrophage, promoting B cell proliferation and therefore antibody production [7]. Significant IL-10 high levels have been found in the active lesions, stimulated PBMC cultures and serum from patients with BD [34]. Found over expression of IL-10 (75 fold increase) from biopsy specimens obtained from oral and genital ulcers, pseudofolliculitis lesions, and lesions at the site of pathergy testing [35].
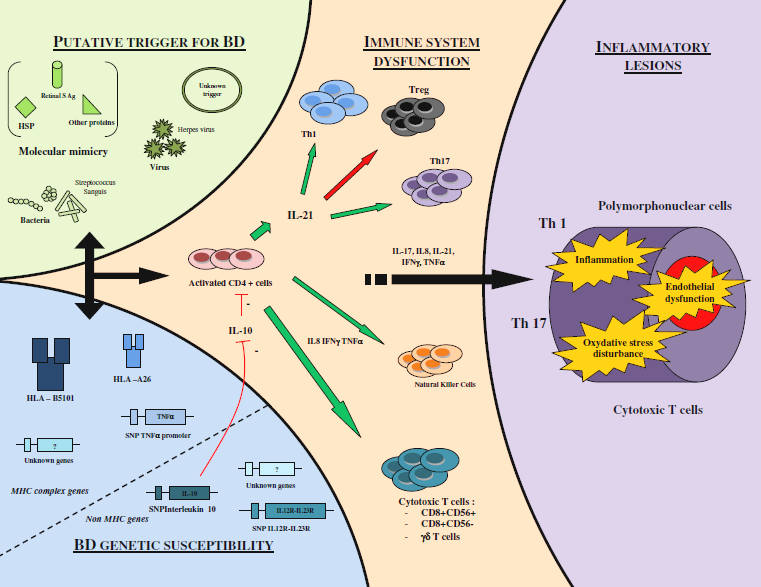
Figure: T cell homeostasis perturbation, especially Th1 and Th17 expansions and decrease regulation by Tregs are now supposed to be involved in the pathogenesis... Inflammatory cytokine such as IL-17, IL-23 and IL21 seems to play a critical role in pathogenesis of BD.
References
-
Alpsoy E, Akman A (2006) Treatment of Behçet’s disease Therapy. 3(1): 139-151.
-
Önder M, Gürer MA (2001) The multiple faces of Behçet's disease and its aetiological factors. Journal of the European Academy of Dermatology and Venereology 15(2): 126-136.
-
Gül A (2001) Behcçet’s disease: an update on the pathogenesis. Clin Exp Rheumatol 19(5): S6-12.
-
Direskeneli H (2001) Behcet’s disease: infectious aetiology, new autoantigens, and HLA-B51. Ann Rheum Dis 60(11): 996-1002.
-
Hamzaoui K, Hamzaoui A, Guemira F, Bessioud M, Hamza M, et al. (2002) Cytokine profile in Behcet’s disease patients. Relationship with disease activity. Scand J Rheumatol 31(4): 205-210.
-
Rajendram R, Rao NA (2003) Molecular mechanisms in Behcet’s disease. Br J Ophthalmol 87(10): 1199- 200.
-
Zhou ZY, Chen SL, Shen N, Lu Y (2012) Cytokines and Behcet's Disease. Autoimmun Rev 11(10): 699-704.
-
Triolo G, Acardo-Palumbo A, Dieli F, Ciccia F, Ferrante A, et al. (2002) Humoral and cell mediated immune responses to cow’s milk proteins in Behçet’s disease. Ann Rheum 61(5): 459-462.
-
Koarada S, Haruta Y, Tada Y, Ushiyama O, Morito F, et al. (2004) Increased entry of CD4+ T cells into the Th1 cytokine effector pathway during T-cell division following stimulation in Behcet's disease. Rheumatology (Oxford) 43(7): 843-851.
-
Pravica V, Asderakis A, Perrey C, Hajeer A, Sinnott PJ, et al. (1999) In vitro production of IFN-gamma correlates with CA repeat polymorphism in the human IFN-gamma gene. Eur J Immunogenet 26(1): 1-3.
-
Warlé MC, Farhan A, Metselaar HJ, Hop WCJ, Perrey C, et al. (2003) Are cytokine gene polymorphisms related to in vitro cytokine production profiles?. Liver Transpl 9(2): 170-181.
-
Gür-Toy G, Lenk N, Yalcin B, Aksaray S, Alli N (2005) Serum interleukin-8 as a serologic marker of activity in Behçet's disease. Int J Dermatol 44(8): 657-660.
-
Durmazlar SPK, Ulkar GB, Eskioglu F, Tatlican S, Mert A, et al. (2009) Significance of serum interleukin-8 levels in patients with Behcet's disease: high levels may indicate vascular involvement. Int J Dermatol 48(3): 259-264.
-
Duymaz-Tozkir J, Yilmaz V, Uyar FA, Hajeer AH, Saruhan-Direskeneli G, et al. (2005) Polymorphisms of the IL-8 and CXCR2 genes are not associated with Behçet's disease. J Rheumatol 32(1): 93-97.
-
Dinarello CA (1996) Biologic basis for interleukin-1 in disease. Blood 87(6): 2095-2147.
-
Hamzaoui K, Hamza M, Ayed K (1990) Production of TNF-alpha and IL-1 in active Behçet's disease. J Rheumatol 17(10): 1428-1429.
-
Pay S, Erdem H, Pekel A, Simsek I, Musabak U, et al. (2006) Synovial proinflammatory cytokines and their correlation with matrixmetalloproteinase-3 expression in Behcet's disease. Does interleukin-1b play a major role in Behçet's synovitis?. Rheumatol Int 27: 608-613.
-
Oztas MO, Onder M, Gurer MA, Bukan N, Sancak B (2005) Serum interleukin 18 and tumor necrosis factor-alpha levels are increased in Behcet’s disease. Clin Exp Dermatol 30: 61-63.
-
Arayssi T, Hamra R, Homeidan F, Uthman I, Awwad ST, et al. (2005) The efficacy of a single dose of infliximab in the treatment of Behcet’s disease uveitis. Clin Exp Rheumatol 23(3): 427.
-
Harrington LE, Hatton RD, Mangan PR, Turner H, Murphy TL, et al. (2005) Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat Immunol 6(11): 1123-1132.
-
Kawaguchi M, Adachi M, Oda N, Kokubu F, Huang SK (2004) IL-17 cytokine family. J Allergy Clin Immunol 114(6): 1265-1273.
-
Moseley TA, Haudenschild DR, Rose L, Reddi AH (2003) Interleukin-17 family and IL-17 receptors. Cytokine Growth Factor Rev 14(2): 155-174.
-
Habibagahi Z, Habibagahi M, Heidari M (2010) Raised concentration of soluble form of vascular endothelial cadherin and IL-23 in sera of patients with Behçet's disease. Mod Rheumatol 20(2): 154-159.
-
Lew W, Chang JY, Jung JY, Bang D (2008) Increased expression of interleukin-23 p19 mRNA in erythema nodosum-like lesions of Behçet's disease. Br J Dermatol 158(3): 505-511.
-
Leng RX, Chen GM, Pan HF, Ye DQ (2010) The role of IL-23/IL-17 axis in the etiopathogenesis of Behçet's disease. Clin Rheumatol 29(10): 1209.
-
Trinchieri G (1993) Interleukin-12 and its role in the generation of TH1 cells. Immunol Today 14(7): 335- 338.
-
Belguendouz H, Messaoudene D, Hartani D, Chachoua L, Ahmedi ML, et al. (2008) Effect of corticotherapy on the production of interleukin 8 and 12 and nitric oxide production during Behçet and idiopathic uveitis. J Fr Ophtalmol 31(4): 387-395.
-
Musabak U, Pay S, Erdem H, Simsek I, Pekel A, et al. (2006) Serum interleukin-18 levels in patients with Behçet's disease. Is its expression associated with disease activity or clinical presentations?. Rheumatol Int 26(6): 545-550.
-
Lie JT (1992) Vascular involvement in Behcet’s disease: arterial and venous vessels of all sizes. J Rheumatol 19(3): 341-343.
-
Schmitz-Huebner U, Knop J (1984) Evidence for an endothelial cell dysfunction in association with Behcet’s disease. Thromb Res 34(4): 277-285.
-
Orem A, Cimşit G, Değer O, Vanizor B, Karahan SC (1999) Autoantibodies against oxidatively modified low-density lipoprotein in patients with Behcet’s disease. Dermatology 198(3): 243-246.
-
Kallen KJ (2002) The role of transsignalling via the agonistic soluble IL-6 receptor in human diseases. Biochem Biophys Acta 1592(3): 323-343.
-
Nalbant S, Sahan B, Durna M, Ersanli D, Kaplan M, et al. (2008) Cytokine profile in Behçet uveitis. Bratisl Lek Listy 109: 551-554.
-
Guenane H, Hartani D, Chachoua L, Lahlou-Boukoffa OS, Mazari F, et al. (2006) Production of Th1/Th2 cytokines and nitric oxide in Behçet's uveitis and idiopathic uveitis. J Fr Ophtalmol 29: 146-152.
-
Ben Ahmed M, Houman H, Miled M, Dellagi K, Louzir H (2004) Involvement of chemokines and Th1 cytokines in the pathogenesis of mucocutaneous lesions of Behçet's disease. Arthritis Rheum 50(7): 2291-2295.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions