Zika Virus: Mode of transmission, Outrageous Effects and Clinical Trials
Zika has become one of the most worldwide spreading dangerous infection over the past decade because of its perpetual spread, initially in Asia-Pacific region, followed by its expeditious entry into the Western world. Zika virus was initially discovered in rhesus monkey in the forest of Uganda. But due to Unique genetic recombination in the genome of Zika virus has made the Zika infection more dangerous than the last one. Zika virus can be transmitted through both vector and non-vector means such as mosquito and sexual transmission. Eighty percent patient with Zika virus showed asymptomatic symptoms on the initial stage of disease onset but later symptoms can become severe. Zika has become one of the most dangerous infections of the 21stcentury because of its association with microcephaly and Guillain-Barre syndrome. Due to the rapid spread of virus WHO declares Zika virus as public health emergency in the end of 2016. There are many methods of early Zika virus diagnosing but the most common method used all over the world is RNA NAT analysis. RT PCR can also use for the early diagnoses of Zika virus. At this time, clinical trials in different countries are continuing for the development of successful vaccines against Zika until now the most effective vaccine developed against Zika is DNA vaccine due to its effective mechanism of action and high efficacy. Various antiviral drugs against Zika have also approved by FDA. In our review, we emphasize on every aspect of Zika virus from the genetic basis to its effective treatment strategies.
Pervaiz Anwar*, KKU Malik, Nida Bashir, Marium Shehzadi and Zunairaaslam
treatment strategies.
Barre syndrome; Vaccines; DNA vaccines; mRNA vaccine
Introduction
Zika is one of the most prominent infections of 21st century which is caused by the Zika virus. Zika virus (ZikaV) is an icosahedral, enclosed, virus whose segmented genome consists of single layer RNA. The Zika V genome codes three operational genes which encode protein for basic structure of virus and seven non- structural proteins (NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5). Zika V has become one of the most worldwide spreading dangerous flavivirus over the past decade because of its perpetual spread, initially in Asia-Pacific
region, followed by its expeditious entry into the Western world [1]. Zika V was initially discovered in Sentinel Rhesus monkey in Uganda in 1947 later in 2007 ZikaV outbreak was reported in 57 countries. Due to genetic recombination and integration of fragments of the Spondweni virus into coding regions of ZikaV the infection cycle of Zika V become very chronic. These genetic changes might also accountable for deviations in the virulence of the Zika V. In 2015 researchers in Brazil find an association of ZikaV with microcephaly and Guillain-Barre syndrome. Zika is also interconnected to a wider set of complications in pregnancy, comprising miscarriage, stillbirth, premature birth and eye problems [2]. Due to rapid the spread of virus WHO declares Zika V as emergency for public health in 2016. Later in the end of 2016 researchers demonstrate the accurate mechanisms of transmission and pathogenesis of Zika V, which leads toward accurate diagnostic tests, which later help to developed prophylactic vaccines and antiviral drugs against Zika V [3]. Zika V predominately transmitted through the bite of an infected mosquito (Aedes family).Zika virus can also be transmitted through an non vector means such as sexual and blood transfusion means [4]. The common symptom of Zika V includes rash, temperature, joint pain, infected red eyes, muscle pain, vomiting, and headache. Preclinical trials for understanding Zika V infection cycle were performed on the various animal model which includes rat, mouse, rhesus monkey [3]. There are many methods of early Zika V diagnosing but most common method used all over the world is RNA NAT analysis (nucleic acid testing) in this method serum of infected person collected after several weeks of symptoms inception. RNA NAT analysis can also be performed by using urine or saliva sample which would be collected in less than 40 days after onset of infection. RT PCR can also use for diagnostic purpose. Zika virus can be diagnosed in pregnant women during 18-20 weeks of pregnancy [5]. Many technologies developed by researchers have reduced the infection and disease burden caused by the flavivirus and RNA virus. Several groups of scientist is continuously working for development of antibodies and vaccine against Zika V until now only one antibiotic like Duramycin was suggested for Zika V, which have a capability of decreasing Zika V infection cycle. An Alternative approach like vaccine can prevent the cycle of diffusion of Zika virus. Perhaps there is a need for vaccine development in corresponding with drug development. Most effective vaccine made until now against Zika V is DNA vaccines because of its effective mechanism of action [6].
Complete coding information or genome sequence of Zika V was uploaded to public databases on 31stMarch 2016. For the very first time in 2017, the full genome of the African Zika V strain MR 766 derived from the monkey was sequenced. The genome of Zika V is 10.8-kb long consist of single-stranded positive sense RNA, which encodes a polyprotein of 3419 amino acids [7]. The Smaller polypeptide of Zika V was only segregated from monkey and mosquitoes. The untranslated regions in Flaviviruses have conserved sequence such as CS1, CS2, and CS3 which play an essential role in genomic stabilization of virus. While sequencing MR 766 strain of Zika V scientist concludes that MR 766 strain OF Zika V contains certain variation in capsid proteins. In some strains of Zika V polymorphism was also observed which increase the pathogenicity of Zika V [8]. Open reading frame encodes single chain of proteins which is further cleaved by viral or host proteases and then convert into structural proteins such as the capsid protein(C), the precursor membrane protein (prM), and the envelope protein (E) and seven nonstructural proteins such as (NS1, NS2A, NS2B, NS3, NS4A, NS4B and NS5). All the members of Flavivirus genus have certain similar structure and functional properties. These viruses have the same gene order from5′ to 3′ UTR [7]. The gene order of Zika V is 5'-C-prM(M)-E-NS1- NS2A-NS2B-NS3- NS4A-2K-NS4B-NS5-3' [8]. The viral capsid consists of the C protein, which is icosahedral in shape and enclosed by globular lipid bilayers. The E proteins are translated into the viral surface and have transmembrane coils that attached them on the outside membrane. The M protein initially translated into the immature form known as prM and then this protein is cleaved by furin that produced mature protein segment and pr segment then a complete virion exit from the cell as explained in the fig 1. During virion assembly, prM complex plays vital role in protection of protein E from degradation. The seven nonstructural proteins encoded by the Zika V genome (NS1, NS2A, NS2B, NS3, NS4A, NS4B, and NS5) play an important role in viral replication and also activate cell-mediated immune response of the host the whole genome components described in fig 1.
Single-stranded positive sense RNA
genome Polyprotein structure
Structural protein Nonstructural protein
encodes encodes capsid (C), precursor membrane (prM), the envelope protein (E)
Viral partical, membrane fusion,
receptor binding, host immune recogination translation Host/viral protease NS1, NS2A, NS2B, NS3, NS4A, NS4B and NS5 Genome replication, polyprotein processing Figure 1: Flow chart of the genome of Zika virus.
Manifestation of Zika virus
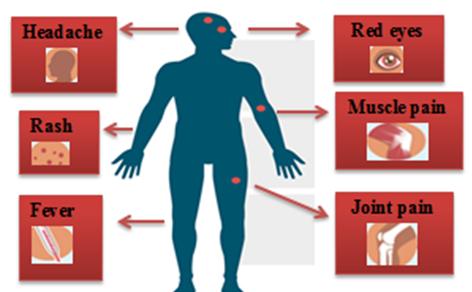
The incubation period of Zika V is from week to 15- days.The symptoms caused by Zika V is similar to the symptoms caused by arbovirus. The most common symptoms caused by Zika V include fever, skin rashes, muscle and joint pain, and headache (mentioned in figure 2). In 2016 WHO declares that Zika V infection during pregnancy caused more serious disease like microcephaly and Guillain-Barre syndrome.
Zika Virus Transmission Dynamics
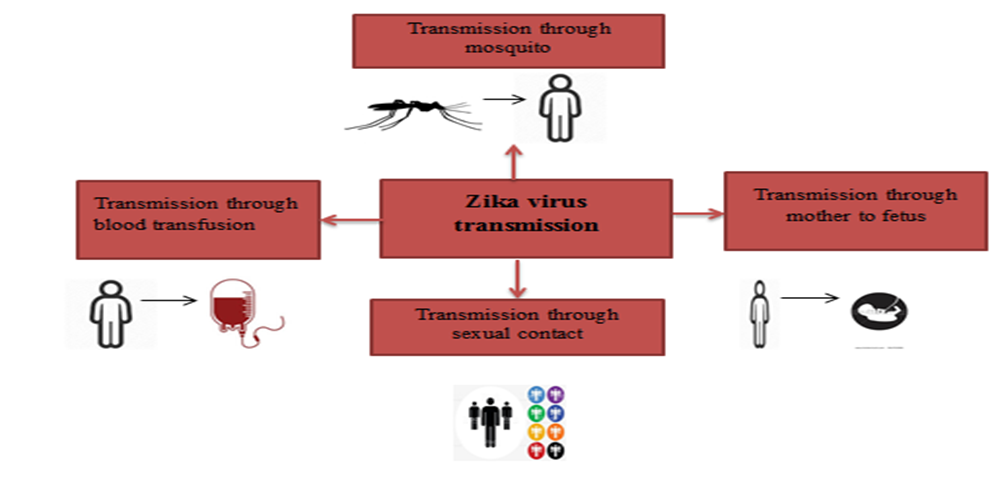
Mosquito Borne Transmission Zika V is transmitted by the mosquitos Aedesaegypti, it is regarded as the trajectory of Zika virus and widely distributed in the tropical and subtropical areas. Aedes are also trajectory for the MENV and the virus Chikungunya (CHIKV). Zika V has a sylvatic not-human cycle for transmission [9]. More precisely, the United States has relatively low rates of obstructions urban, the omnipresent use of shades, air-circulation system and use of better waste managing system can help to reduce mosquito propagation rate. Man serves as a principal vertebrate host for Zika V in the urban environment. Moreover, the United States established a monitoring system of the arboviruses permanently by using early inventions like pathogenic vectors (IE, the reduction of the sites of reproduction and the use of the biological pesticides/methods to control the larvae of mosquitos and the mosquitos adult) [10]. Sexual Transmission Zika virus can also be conveyed by sexual contact between infected carriers to non-infected persons (as describe in fig 3). In 2016 a case study indicated that Zika V can diffuse by the virus carrier man to his female partner by sexual contact [11]. In most cases foreign traveler can carry the virus from place to place and transmit it. In many cases the sexual intercourses took place earlier before the appearance of the viral disease indications, whereas in other circumstances, the sexual intercourses took place during the appearance of indications and soon after. Viral particles replicative of Zika virus, as well as the viral RNA were found in infected person in high number, and the viral RNA, was spotted up to 62 days afterward the appearance of the signs. Many patients show symptoms after sexual transmission, but the sexual transmission was also shown in that patients are asymptomatic at the time of the sexual contact. Male to female transmission is the most common, but there have also been reports of sexual transmission from female to male and from male to male. The growing number of case of sexual transmission led to a recommendation for the abstinence or of protective equipment at the time of sexual contacts for one long period of time after the infection by the Zika V. Transmission Through Blood The transmission risk in the donating blood component transfused was a concern after the detection of the viral RNA into the blood of the healthy donor (as mentioned in figure 3). Report of Brazil describes two cases of Zika V transmission by transfusion of blood of an infected person who donated presymptomatic plates per apheresis, on January 16th, 2016. The two units of plates leukodepleted were irradiated with 25 Gy delivered by irradiative gamma IBL-437C (international organic CIS) and were transfused with different patients on January 19th (day 0). On January 21st, the giver called the bank of blood to announce a skin eruption, retro orbital pain, and the pain in the two knees which had begun on January 18th. An investigation was open under the terms of the clinical hospital of the protocol of the undesirable effects associated with the transfusion, with the giver and the two patients to provide a written enlightened assent. Two samples which were obtained from the donor before and after the transfusion were negative for the virus chikungunya (CHIKV) and the virus of dengue (DENV) on the (RT-PCR), but the index of the samples of plasma and the 14-day old urine later were positive for the Zika V [12]. Maternal Transmission of Zika Virus Significant evidence now specifies that Zika V can also diffuse from mother to fetus throughout the pregnancy [13]. The RNA of the Zika virus was recognized in the amniotic liquescent of the mothers whose off springs has cerebral lesions perceived by echography, the 40-54 antigen and viral RNA were recognized in fabrics of the CNS and the placentas of the newborns with microcephaly and died shortly afterwards the birth, viral fabrics were found in blood sample. The incidence and the hazard aspects of diffusion are still unknown. Three cases of perinatal spread of the Zika virus were described in couples of mother’s infants. The RNA of Zika virus was spotted in the two children; a child had a light eruption and a thrombocytopenia, while the other was asymptomatic. fig 3 define the whole route of transmissions [14].
Outrageous effects of Zika virus
Microcephaly: Microcephaly is a medical condition in which head size of the person is less than the standard head size. There are two types of microcephaly observed in humans the first type of microcephaly occurred when brain fails to grow to its suitable size during 32 weeks of gestation period and mainly caused due to inadequate amount of neuron production but in second type of microcephaly brain normally grow during gestation period but later some deformities occurred in the dendritic portion. Form the observation of recent evidence it is suggested that Zika V have some association with microcephaly during pregnancy period if mother suffered from Zika V there is many chances that new born suffer from the type 1 of microcephaly. Zika V primarily affects the fibroblast and keratinocytes of the target individuals. Zika V also effectively targets the placenta macrophages and induces production of the cytokines due to which antiviral gene expression occurred. Zika V particles entered into cell by interacting with cell surface receptors such as TYRO3 and AXL and TAM. When Zika V entered into the cells cause alternation in the genes which associated with the cell cycle, cell differentiation, and apoptosis and in result of these alternation brain deformation occurs. Such brain deformity is categorized as microcephaly. Guillain-Barre syndrome: It is a mysterious sickness of the nervous system in which persons own immune system injuries the nerve cell due to which muscle weakness occurred and sometime in severe cases paralysis. Form the recent evidence in America it is suggested that Zika have some association with Guillain- Barre syndrome. Zika virus complications can find the association with guillian barre syndrome (GBS) and it was confirmed by magnetic resonance imaging. GBS is an autoimmune neuropathy which attacks peripheral nervous system that leads to muscle weakness, numbness, paralysis and might be death [15]. In the outbreak of French Polynesia in 2013-2014, 38 cases of ZIKV disease were established to have the Guillain-Barré syndrome. Although, the complete association of Guillain- Barré syndrome with ZIKV still remains imprecise. In 2016 scientist reported that ZIKV relation with GBS was described by inflammation, demyelization and collapsing of blood-brain barrier. During the outbreak, scientist observed that 98% of patients have anti-ZIKV IgM or IgG which diagnosed with this syndrome. One report from brazil refers to that due to increased ZIKV infection outbreak also expected increased number of GBS in patients. In addition to GBS, it might be possible to increased problems in other neurological disorder [16].
Vaccine Strategies against Zika virus
Many Vaccines approaches have been developed against flavivirus. But, three vaccines are present against Zika (as mentioned in figure 4). Currently, many clinical trials are performing in different regions of the world for the development of the vaccine against Zika V. Among them, only DNA Vaccines has been approved for phase 2 clinical trials. mRNA Vaccines against Zika V is still in progress.
DNA Vaccines
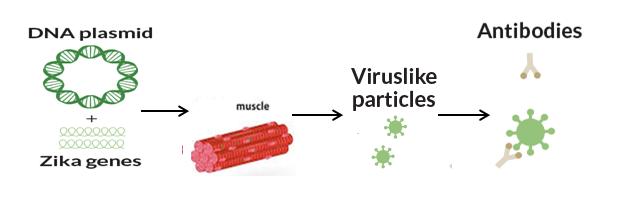
DNA vaccine against Zika V was formed by the scientist of NIAID. DNA vaccines in phase 1 trials successfully induce protection in the mouse and monkey. For checking its effectiveness in human phase 2 trials were performed. For experimentation purpose, they enroll the 2,490 persons from different areas like Brazil and America where Zika V is most activated. Among them most people have little or significant symptoms of the Zika V [17]. For the formation of DNA vaccine scientist inserted two genes in the small piece of DNA or plasmid these genes encode two proteins that were found on the surface of the Zika V. For the trial purpose this vaccine was injected in the muscle of the healthy volunteers in the result of these trails it was observed that DNA vaccine can trigger the immune response of the infected person without causing any damage. Among immune cells, myeloid cell and B cell possibly support the Zika V infection. Still, this DNA vaccine against Zika V is not commercialized due to certain safety and efficacy issues. But until now DNA vaccine is most successful vaccine strategy against Zika V due to its unique mechanism of action. The process of formation of DNA vaccine described in figure 5.
Live Attenuated Vaccine
In this type of vaccine, viruses are adequately attenuated or debilitated which are still able to show immune response and can immune us from Zika V infection. Live attenuated vaccine has various advantages such as single dose is enough for activating immune response and it can give us long-lived protection but still live attenuated vaccine have certain safety issues especially in the case of Zika V. For the formation of the live attenuated vaccine scientist deleted the one particular segment from the genome of the virus the same approach was used for the formation of successful vaccine against dengue. Until now these vaccines are very effective in mice and non-human primate but no human trials are performed until now by using live attenuated Zika V. The dose of the live attenuated organisms recommended according to the patient disease history and intentness or gravity of its disease. It is not a very efficient vaccine against Zika V as compared to DNA vaccine. Characteristics of live attenuated vaccine describe in table 1.
| Live Attenuated | References | |
|---|---|---|
| Advantages: | Single dose, Long-lasting immunity. | (Oehler, Watrin et al. 2014) |
| Disadvantages: | Safety and efficacy issues. | (Oliveira Melo, Malinger et al. 2016) |
| In development for Zika virus | phase I Trials. | (Oliveira Melo, Malinger et al. 2016) |
| Other flavivirus vaccines: | IMOJEV (JE), vaccine against dengue. | (Brasil, Pereira Jr et al. 2016) |
Table 1: Live Attenuated Vaccines against Zika Virus.
mRNA Vaccine
RNA vaccines have an open reading frame which encodes antigen of interest and then translated by the host cell. RNA vaccine has the safest advantage as compared to DNA vaccine because RNA cannot integrate into the host genome. Modified mRNAs encoding lipid nanoparticles encapsulated with prM / E from Asian lineage Zika V strain are shown to defend immunocompromised (AG129) mice as well as immunocompetent (C57BL/6) mice while treated with a blocking anti-IFNARl antibody. Further scientist modified mRNA vaccine by deleting four amino acids in or near the E-DII-FL regions to minimize the ADE response. Furthermore, scientist induced single immunization dose of different Zika V prM/E regions encoding mRNA lipid nanoparticle vaccine in rhesus macaque model show fifty times greater neutralizing effect on antibody titers as compared to DNA vaccine [18]. Production of RNA vaccine is cost-effective and only small doses are enough to induce for the protective immune response [19]. Currently, there is Phase I clinical trial of one mRNA vaccine are in progress. The basic characteristics of mRNA vaccine define in table 2.
| mRNA Vaccines | References | |||||||
|---|---|---|---|---|---|---|---|---|
| Advantages | Well tolerated, Rapid development. | (Hamel, Dejarnac et al. 2015) | ||||||
| New routes of immunization require trained | ||||||||
| Disadvantages | (Brasil, Pereira Jr et al. 2016) | |||||||
| persons, Limited commercial scale production. | ||||||||
| Complete protection against Zika in animal | ||||||||
| In development for Zika | (Hamel, Dejarnac et al. 2015) | |||||||
| models. | ||||||||
| Other flavivirus vaccines | No licensed human vaccines. | (Brasil, Pereira Jr et al. 2016) |
Table 2: mRNA Vaccines against Zika Virus
Conclusion & Future Perspective
A Few years back, Zika virus was considered inoffensive but due to its rapid spread throughout the world scientist are searching better way for diagnoses and treatment of Zika virus. Zika virus is a mosquito- borne virus belonging to the species of Aedes, which is also serving as a trajectory for diffusion of other Flaviviruses like Dengue and Chikungunya. Nevertheless, there is also other route of transmission like sensual interaction and blood transfusion; main distress must be granted to the mosquito control because it is the main cause of Zika virus transmissions. The existing rate of Zika V infection in the world is challenging to determine accurately because the symptoms are imprecise and asymptomatic or insignificant and workshop analyses of Zika virus is not available in every region of the affected area. Some current therapies discovered by the scientist show auspicious affect in controlling Zika virus infection and associated diseases. These therapies include inhibiting virus entry into the cells or by targeting viral infectious proteins which are responsible for causing infection. At this time various clinical trials are performing in laboratory for development of the most effective vaccine against Zika virus. The most successful trials are given by the DNA and mRNA vaccine which act by targeting the genome of the Zika virus or by inhibiting its protein synthesis mechanism. In future for controlling the further outbreak of Zika virus, certain preventive measure should be adopted and diagnoses method should be improved in urban areas of Africa where ratio of Zika virus infected patient is significantly high. Furthermore, trails should be performed in the laboratory for commercialization of vaccine and antiviral drugs against Zika virus. The current inauguration of a Zika vaccine enterprise by NIH might give the essential enhancement to the vaccine expansion practice, and many nations have introduced movements to accelerate research on this facade. Furthermore, the main points of future perspective described in figure 6.
Conflict of interest
There is no affiliation or involvement of any organization in financially supporting us.
Acknowledgement
We specially like to thanks our respected professors Dr Zunaira and Dr Parvez for guiding us.
References
-
Sikka V, Chattu VK, Popli RK, Galwankar SC, Kelkar D, et al. (2016) The emergence of Zika virus as a global health security threat: a review and a consensus statement of the INDUSEM Joint Working Group (JWG). Journal of global infectious diseases 8(1): 3-15.
-
Gebre Y, Forbes N, Gebre T (2016) Zika virus infection, transmission, associated neurological disorders and birth abnormalities: A review of progress in research, priorities and knowledge gaps. Asian Pacific Journal of Tropical Biomedicine 6(10): 815-824.
-
Boeuf P, Heidi ED, Jack SR, Michelle JL, Scoullar, et al. (2016) The global threat of Zika virus to pregnancy: epidemiology, clinical perspectives, mechanisms, and impact. BMC medicine 14(1): 112.
-
Musso D, Roche C, Robin E, Nhan T, Teissier A, et al. (2015) Potential sexual transmission of Zika virus. Emerging infectious diseases 21(2): 359-361.
-
Hennessey M, Fischer M, Staples JE (2016) Zika virus spreads to new areas-region of the Americas, May 2015-January 2016. American Journal of Transplantation 16(3): 1031-1034.
-
Fernandez E, Diamond MS (2017) Vaccination strategies against Zika virus. Curr Opin Virol 23: 59- 67.
-
Wang A, Thurmond S, Islas L, Hui K, Hai R (2017) Zika virus genome biology and molecular pathogenesis. Emerging microbes & infections 6(3): e13.
-
Singh RK, Dhama K, Malik YS, Ramakrishnan MA, Karthik K, et al. (2016) Zika virus-emergence, evolution, pathology, diagnosis, and control: current global scenario and future perspectives-a comprehensive review. Veterinary Quarterly 36(3): 150-175.
-
Petersen LR (2016) Zika virus. New England Journal of Medicine 374(16): 1552-1563.
-
Aliota MT, Bassit L, Bradrick SS, Cox B, Garcia-BMA, et al. (2017) Zika in the Americas, year 2: What have we learned? What gaps remain? A report from the Global Virus Network. Antiviral Res 144: 223-246.
-
Mansuy JM, Dutertre M, Mengelle C, Fourcade C, Marchou B, et al. (2016) Zika virus: high infectious viral load in semen, a new sexually transmitted pathogen. Lancet Infect Dis 16(4): 405.
-
Motta IJ, Spencer BR, Cordeiro da Silva SG, Arruda MB, Dobbin JA, et al. (2016) Evidence for Transmission of Zika Virus by Platelet Transfusion. New England Journal of Medicine 375(11): 1101- 1103.
-
Villamil-Gómez WE, Rodríguez-Morales AJ, Uribe- García AM, González-Arismendy E, Castellanos JE, et al. (2016) Zika, dengue, and chikungunya co-infection in a pregnant woman from Colombia. International Journal of Infectious Diseases 51: 135-138.
-
Jimenez A, Shaz BH, Bloch EM (2017) Zika virus and the blood supply: what do we know?. Transfusion medicine reviews 31(1): 1-10.
-
Pawitwar SS, Dhar S, Tiwari S, Ojha CR, Lapierre J, et al. (2017) Overview on the Current Status of Zika Virus Pathogenesis and Animal Related Research. Journal of Neuroimmune Pharmacology 12(3): 371- 388.
-
Dos Santos T, Rodriguez A, Almiron M, Sanhueza A, Ramon P, et al. (2016) Zika virus and the Guillain- Barré syndrome-case series from seven countries. New England Journal of Medicine 375(16): 1598- 1601.
-
Larocca RA, Abbink P, Peron JPS, Zanottoet PMA, Iampietro MJ, et al. (2016) Vaccine protection against Zika virus from Brazil. Nature 536(7617): 474-478.
-
Richner JM, Himansu S, Dowd KA, Butler SL, Salazar V, et al. (2017) Modified mRNA vaccines protect against Zika virus infection. Cell 168(6): 1114-1125.
-
Pardi N, Michael JH, Rebecca SP, Hiromi M, Hanne A, et al. (2017) Zika virus protection by a single low- dose nucleoside-modified mRNA vaccination. Nature 543(7644): 248-251.
- hMPV: Is It Another Covid-19 Like Situation?
- Streptomyces: Sources of Novel Discoveries in Antibiotic Research to Combat Antimicrobial Resistance
- A Review of Mosquitoes (Diptera: Culicidae) and Their Biodiversity, Medical and Veterinary Importance
- Past and Current Immunotherapy in Cancer
- Hematological Cancer and Viral Infection
- The Growing Threat of Antimicrobial Resistance in India: Challenges and Solutions